Naropin should only be used by, or under the supervision of, clinicians experienced in regional anaesthesia.
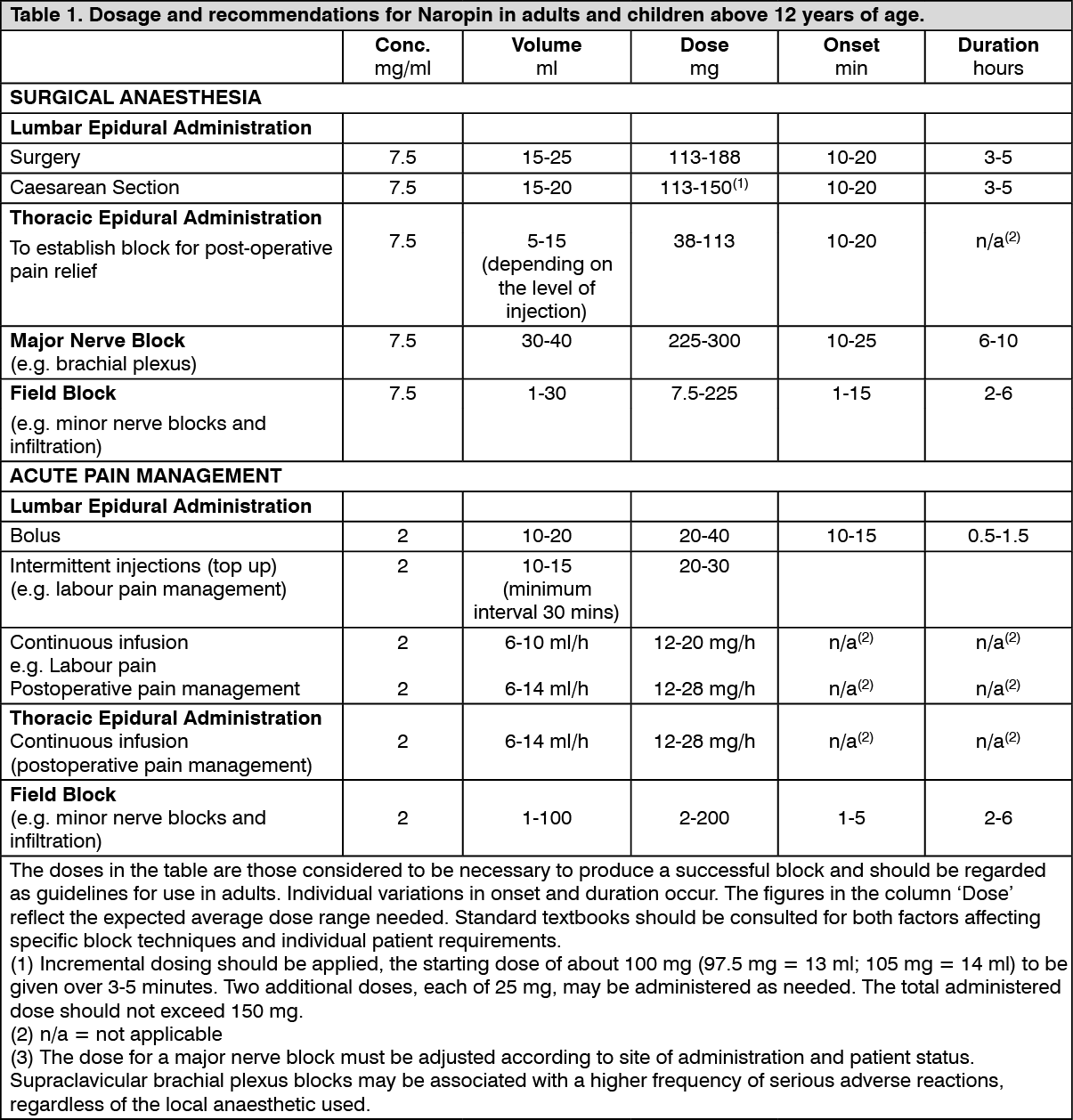
ADULTS AND CHILDREN ABOVE 12 YEARS OF AGE: The following table is a guide to dosage for the more commonly used blocks. The clinician's experience and knowledge of the patient's physical status are of importance when deciding the dose. In general, surgical anaesthesia (e.g. epidural administration) requires the use of the higher concentrations and doses. For analgesia the 2 mg/ml concentration of Naropin is generally recommended. (See Table 1).
 Click on icon to see table/diagram/image
Method of administration:
Click on icon to see table/diagram/image
Method of administration: In order to avoid intravascular injection, aspiration should be repeated prior to and during administration of the main dose, which should be injected slowly or in incremental doses, at a rate of 25-30 mg/min, while closely observing the patient's vital functions and maintaining verbal contact. When an epidural dose is to be injected, a preceding test dose of 3-5 ml lidocaine (lignocaine) with adrenaline (Xylocaine 1-2% with Adrenaline 1:200,000) is recommended. An inadvertent intravascular injection may be recognised by a temporary increase in heart rate and an accidental intrathecal injection by signs of a spinal block.
If toxic symptoms occur, the injection should be stopped immediately.
In epidural block for surgery, single doses of up to 250 mg ropivacaine have been used and well tolerated.
When prolonged blocks are used, either through continuous infusion or through repeated bolus administration, the risks of reaching a toxic plasma concentration or inducing local neural injury must be considered.
Cumulative doses up to 675 mg ropivacaine for surgery and postoperative analgesia administered over 24 hours were well tolerated in adults, as were postoperative continuous epidural infusions at rates up to 28 mg/hour for 72 hours. In a limited number of patients, higher doses of up to 800 mg/day have been administered with relatively few adverse reactions.
For treatment of postoperative pain, the following technique can be recommended: Unless preoperatively instituted, an epidural block with Naropin 7.5 mg/ml is induced via an epidural catheter. Analgesia is maintained with Naropin 2 mg/ml infusion. Infusion rates of 6-14 ml (12-28 mg) per hour provide adequate analgesia with only slight and non-progressive motor block in most cases of moderate to severe postoperative pain. The maximum duration of epidural block is 3 days.
However, close monitoring of analgesic effect should be performed in order to remove the catheter as soon as the pain condition allows it.
With this technique a significant reduction in the need for opioids has been observed.
In clinical studies an epidural infusion of Naropin 2 mg/mL alone or mixed with fentanyl 1-4 microgram/mL has been given for postoperative pain management for up to 72 hours. Naropin 2 mg/mL (6-14 mL/hour) provided adequate pain relief for the majority of patients. The combination of Naropin and fentanyl provided improved pain relief but caused opioid side effects. The combination of Naropin and fentanyl has been investigated only for Naropin 2 mg/mL.
For Caesarean section, neither intrathecal administration nor the use of the ropivacaine concentration 10 mg/ml for epidural administration, have been documented.
Naropin 2 mg/ml: Children (>30 days old and up to and including 12 years): (See Table 2.)
Click on icon to see table/diagram/image
The recommended strength of Naropin solution for injection/infusion for Single Caudal Epidural Block in children >30 days old and up to 12 years and for Continuous Epidural Infusion in children with a body weight up to 25 kg is 2mg/ml.
The doses in the table should be regarded as recommendations when used in children.
Individual variations occur. For overweight children a gradual reduction of the dosage, based on the ideal body weight, is often necessary. The volume for single caudal epidural block and the volume for epidural bolus doses should not exceed 25 mL in any patient.
Method of administration: To prevent inadvertent intravascular injections, great caution should be observed. Careful aspiration is recommended before and during injection of the total dose. The patient's vital functions should be carefully monitored during the injection. Should toxic signs appear, the injection should be immediately stopped.
When administering the calculated dose, fractionation of the total dose is always recommended.
A single caudal epidural injection of ropivacaine 2 mg/mL produces adequate postoperative analgesia below T12 in the majority of patients when a dose of 2 mg/kg is used in a volume of 1 mL/kg. The volume of the caudal epidural injection may be adjusted to control the spread of the sensory block. Doses up to 3 mg/kg of a concentration of ropivacaine 3 mg/mL have been used safely in children older than 4 years.
For children with a body weight over 25 kg there is limited experience of caudal blocks.
The use of ropivacaine in premature children has not been documented.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image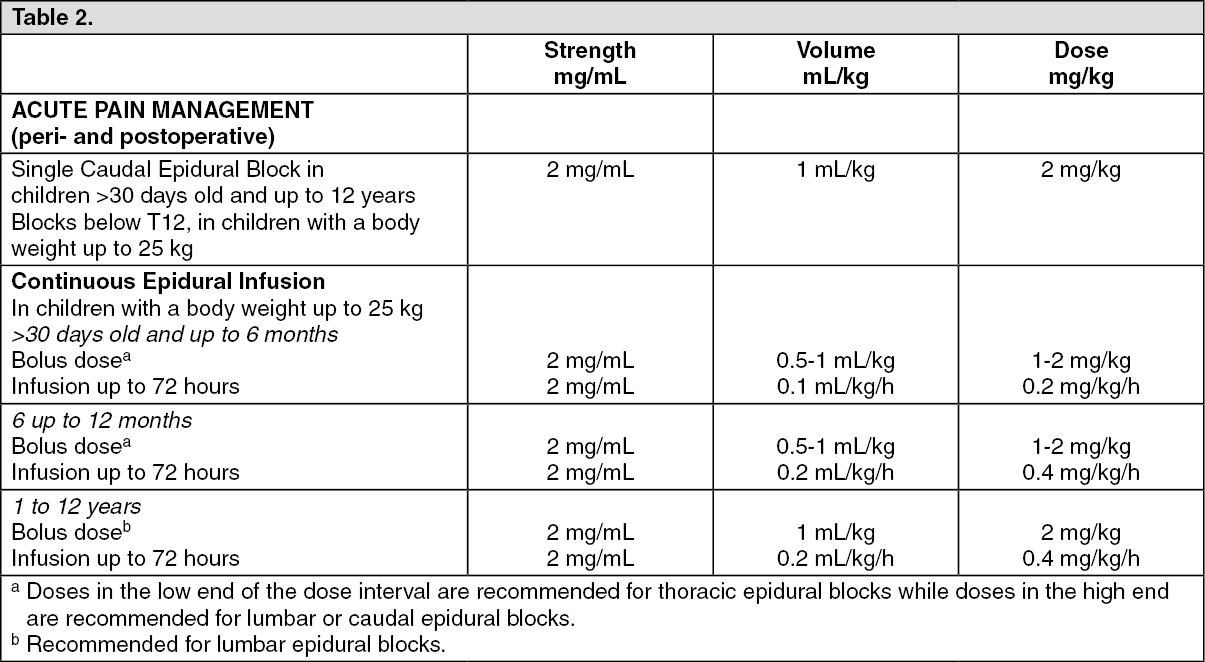 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out
