


 Sign Out
Sign Out

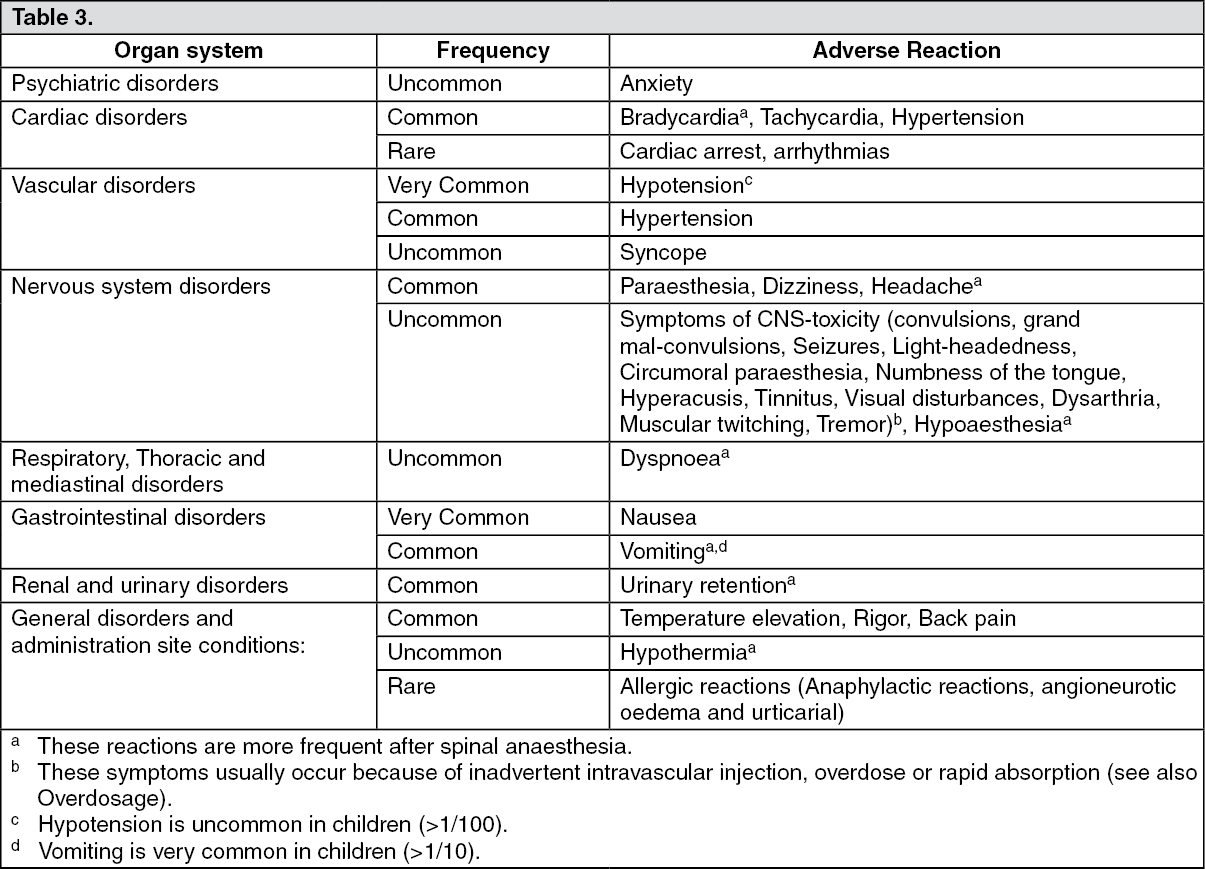
Undesirable effects (from all kinds of blockades): The adverse reactions are displayed within each organ class with the following frequencies: Very common (≥1/10), Common (≥1/100, <1/10), Uncommon (≥1/1 000, <1/100), Rare (<1/1 000).
Adults: (See Table 3.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageClass related adverse drug reactions: The adverse reactions as follows include complications related to the anaesthetic technique regardless of the local anaesthetic used.
Neurological complications: Neuropathy and spinal cord dysfunctions (e.g. anterior spinal artery syndrome, arachnoiditis, cauda equina) have been associated with intrathecal and epidural anaesthesia.
Total spinal block: Total spinal block may occur if an epidural dose is inadvertently administered intrathecally, or if a too large intrathecal dose is administered.
Acute systemic toxicity: Systemic toxic reactions primarily involve the central nervous system (CNS) and the cardiovascular system (CVS). Such reactions are caused by high blood concentration of local anaesthetics, which may appear due to (accidental) intravascular injection, overdose or exceptionally rapid absorption from highly vascularised areas (see also Precautions). CNS reactions are similar for all amide local anaesthetics, while cardiac reactions are more dependent on the drug, both quantitatively and qualitatively.
Central nervous system toxicity: CNS toxicity is a graded response with symptoms and signs of escalating severity. The first symptoms are usually light-headedness, circumoral paraesthesia, numbness of the tongue, hyperacusis, tinnitus and visual disturbances. Dysarthria, muscular twitching and or tremors are more serious and precede the onset of generalized convulsions. These signs should not be mistaken for neurotic behaviour. Unconsciousness and grand mal convulsions may follow which may last for a few seconds to several minutes. Hypoxia and hypercarbia occur rapidly following convulsions due to increased muscular, together with the interference with respiration and possible loss of functional airways. In severe cases even apnoea may occur. Acidosis, hyperkalemia, hypocalcemia and hypoxia increase and extend the toxic effects of local anaesthetics.
Recovery is due to redistribution of the local anaesthetic drug from the central nervous system and subsequent metabolism and excretion.
Recovery may be rapid unless large amounts of the drug have been injected.
Cardiovascular system toxicity: Cardiovascular system toxicity may be seen in severe cases and is generally preceded by signs of toxicity in the central nervous system.
In patients under heavy sedation or receiving a general anaesthetic, prodromal CNS symptoms may be absent. Hypotension, bradycardia, arrhythmia and also cardiac arrest may occur as a result of high systemic concentrations of local anaesthetics but in rare cases, cardiac arrest has occurred without prodromal CNS effects.
In children, early signs of local anaesthetic toxicity may be difficult to detect since they may not be able to verbally express them, or if they are under general anaesthesia (see Precautions).
Treatment of acute systemic toxicity: See Overdosage.
View ADR Monitoring Form