


 Sign Out
Sign Out

To avoid dosing errors, it is important that prescriptions of deferasirox specify both the type of formulation (dispersible tablet or film-coated tablet) and the prescribed dose in mg/kg/day.
Recommended Dose and Dosage Adjustment: For transfusional iron overload: The goals of iron chelation therapy are to remove the amount of iron administered in transfusions and, as required, to reduce the existing iron burden. The decision to remove accumulated iron should be individualized based on anticipated clinical benefit and risks of chelation therapy.
It is recommended that therapy with JADENU (deferasirox) be started when a patient has evidence of chronic iron overload, such as the transfusion of approximately 100 mL/kg of packed red blood cells (approximately 20 units for a 40 kg patient) and a serum ferritin consistently >1000 μg/L. Doses should be in mg/kg and must be calculated and rounded to the nearest whole tablet size. Changes in weight of pediatric patients over time must be taken into account when calculating the dose. JADENU is available in three strengths (90, 180 and 360 mg).
Starting Dose: The recommended initial daily dose of JADENU is 7, 14 or 21 mg/kg/day body weight, depending on the patient's transfusion rate and the goal of treatment: Patients requiring maintenance of an acceptable body iron level: An initial daily dose of 7 mg/kg/day is recommended for patients receiving less than 7 mL/kg/month of packed red blood cells (approximately <2 units/month for an adult) and for whom the objective is maintenance of an acceptable body iron level.
An initial daily dose of 14 mg/kg/day is recommended for patients receiving more than 7 mL/kg/month of packed red blood cells (approximately >2 units/month for an adult) and for whom the objective is maintenance of an acceptable body iron level.
Patients requiring reduction of iron overload: An initial daily dose of 14 mg/kg/day is recommended for patients receiving less than 14 mL/kg/month of packed red blood cells (approximately <4 units/month for an adult) and for whom the objective is gradual reduction of iron overload.
An initial daily dose of 21 mg/kg/day is recommended for patients receiving more than 14 mL/kg/month of packed red blood cells (approximately >4 units/month for an adult) and for whom the objective is gradual reduction of iron overload.
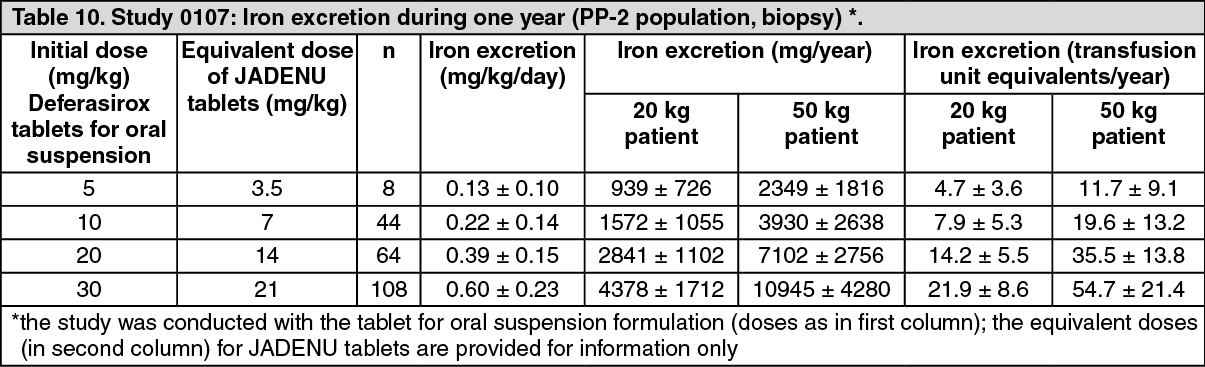
With deferasirox dispersible tablets for oral suspension, the dose dependent iron excretion (mg/kg/day) was calculated from the change in LIC over one year, the amount of blood transfused and the weight of the patient. Using two example patients of 20 kg and 50 kg, the amount of iron excreted over one year could be calculated in terms of mg/year and transfusion unit-equivalents/year (assuming that one unit of PRBC contains 200 mg iron). Thus in a 50 kg adult, deferasirox tablets for oral suspension doses of 10, 20 and 30 mg/kg (equivalent to JADENU 7, 14 and 21 mg, respectively) for one year can remove the amount of iron contained in about 20, 36 and 55 units of blood, respectively (i.e. about 1.5, 3 and 4.5 units of blood per month, respectively). In a 20 kg pediatric patient, deferasirox tablets for oral suspension doses of 10, 20 and 30 mg (equivalent to JADENU 7, 14 and 21 mg, respectively) for one year can remove the amount of iron contained in about 8, 14 and 22 units of blood, respectively (i.e. about 0.6, 1.2 and 1.8 units of blood per month; or 6, 12 and 18 mL/kg/month, respectively). (See Table 10.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageDose Adjustment: It is recommended that serum ferritin be monitored every month and that the dose of JADENU be adjusted if necessary every 3 to 6 months based on serum ferritin trends. Dose adjustments should be made in steps of 3.5 or 7 mg/kg and are to be tailored to the individual patient's response and therapeutic goals (maintenance or reduction of body iron burden). In patients with beta-thalassemia not adequately controlled with daily doses of 21 mg/kg, doses of up to 28 mg/kg may be considered.
If the serum ferritin falls consistently below 500 μg/L, consideration should be given to temporarily interrupting therapy with JADENU. As with other iron chelator treatment, the risk of toxicity of JADENU may be increased when inappropriately high doses are given in patients with a low iron burden or with serum ferritin levels that are only slightly elevated. Doses of JADENU should not exceed 28 mg/kg per day since, with the exception of beta-thalassemia patients, there is limited experience with doses above this level (See Pharmacology: Pharmacodynamics: Clinical trials under Actions).
The Liver Iron Concentration (LIC) should be assessed periodically by an appropriate method such as biopsy or MRI in order to verify treatment response.
For non-transfusion-dependent thalassemia syndromes: Chelation therapy should only be initiated when there is evidence of iron overload (liver iron concentration (LIC) ≥5 mg Fe/g dry weight (dw) or serum ferritin consistently >800 microgram/L). In patients with no LIC assessment, caution should be taken during chelation therapy to minimize the risk of over-chelation. Doses should be in mg/kg and must be calculated and rounded to the nearest whole tablet size. JADENU is available in three strengths (90, 180 and 360 mg).
Starting Dose: The recommended initial daily dose of JADENU is 7 mg/kg body weight.
Dose Adjustment: It is recommended that serum ferritin be monitored every month. Every 3 to 6 months of treatment, consider a dose increase in increments of 3.5 to 7 mg/kg if the patient's LIC is ≥7 mg Fe/g dw, or serum ferritin is consistently >2,000 microgram/L and not showing a downward trend, and the patient is tolerating the drug well. The incidence of adverse effects increases with increasing dose. Experience with doses of 14mg/kg is limited. Doses above 14 mg/kg are not recommended because there is no experience with doses above this level in patients with non-transfusion-dependent thalassemia syndromes.
In patients in whom LIC was not assessed and serum ferritin is ≤2,000 microgram/L, dosing should not exceed 7 mg/kg.
For patients in whom the dose was increased to >10 mg/kg, dose reduction is recommended to 7 mg/kg or less when LIC is <7 mg Fe/g dw or serum ferritin is ≤2,000 microgram/L.
Once a satisfactory body iron level has been achieved (LIC <3 mg Fe/g dw or serum ferritin <300 microgram/L), treatment should be interrupted. Treatment should be re-initiated when there is evidence from clinical monitoring that chronic iron overload is present.
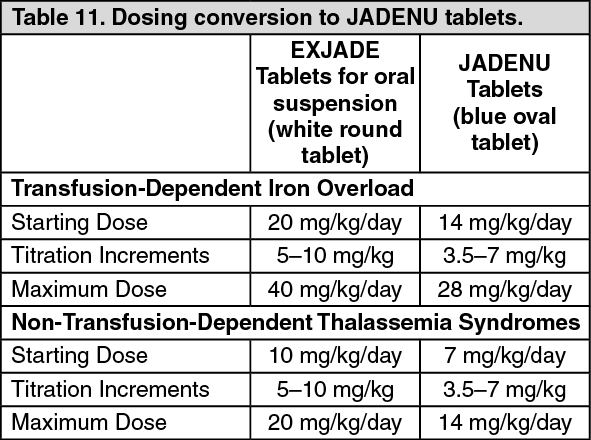
Dosing Considerations: Conversion from EXJADE to JADENU: For patients who are currently on chelation therapy with EXJADE (deferasirox tablets for oral suspension) and converting to JADENU tablets, the dose of JADENU should be about 30% lower, rounded to the nearest whole tablet. The table as follows provides additional information on dosing conversion to JADENU tablets. (See Table 11.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageGeriatrics (≥ 65 years of age): The pharmacokinetics of deferasirox have not been studied in geriatric patients. The dosing recommendations for elderly patients are the same as described above. In clinical trials, elderly patients experienced a higher frequency of adverse reactions than younger patients and should be monitored closely for adverse reactions that may require a dose adjustment.
Pediatrics (2 to 16 years of age): The dosing recommendations for pediatric patients are the same as for adult patients. In children < 6 years of age, exposure was about 50% lower than adults. Since dosing is individually adjusted according to response this difference in exposure is not expected to have clinical consequences. Changes in weight of pediatric patients over time must also be taken into account when calculating the dose.
Patients with renal impairment: Deferasirox has not been studied in patients with renal impairment (see Contraindications). For adult patients, the daily dose of JADENU should be reduced by 7 mg/kg if a non-progressive rise in serum creatinine by >33% above the average of the pre-treatment measurements is seen at two consecutive visits, and cannot be attributed to other causes. In clinical trials with deferasirox, from those patients who underwent dose reduction, creatinine levels returned to baseline in only 25% of patients and in 60% of them, creatinine levels remained elevated >33% of the average pre-treatment levels. For pediatric patients, the dose should be reduced by 7 mg/kg if serum creatinine levels rise above the age-appropriate upper limit of normal at two consecutive visits. A total of 6 patients < 16 years developed creatinine levels >ULN during the core phase of the registration studies. Dose reductions were performed in 5 patients, in 4 of whom the levels returned to baseline. Creatinine levels fell to < ULN in the fifth patient but remained higher than baseline.
If there is a progressive increase in serum creatinine beyond the upper limit of normal, JADENU therapy should be interrupted (see Abnormal Hematologic and Clinical Chemistry Findings under Adverse Reactions).
Patients with hepatic impairment: Deferasirox has been studied in a clinical trial in patients with hepatic impairment. For patients with moderate hepatic impairment (Child-Pugh B), the starting dose should be reduced by approximately 50%. JADENU should not be used in patients with severe hepatic impairment (Child-Pugh C) (see Pharmacology under Actions and Warnings and Precautions). Deferasirox treatment has been initiated only in patients with baseline liver transaminase levels up to 5 times the upper limit of normal range. The pharmacokinetics of deferasirox were not influenced by such transaminase levels. The treating physician should initiate treatment with a dose taking into account general dosing instructions together with the extent of hepatic impairment. Close monitoring of efficacy and safety parameters is recommended. It is recommended that serum transaminase, bilirubin and alkaline phosphatase be monitored before the initiation of treatment, every 2 weeks during the first month and monthly thereafter. If there is an unexplained, persistent, and progressive increase in serum transaminase levels JADENU treatment should be interrupted.
Patients with skin rash: Skin rashes may occur during JADENU treatment. Severe skin rashes may require interruption of JADENU treatment.
Gender: Females have a moderately lower apparent clearance (by 17.5%) for deferasirox compared to males. Since dosing is individually adjusted according to response this difference in clearance is not expected to have clinical consequences.
Missed Dose: If a dose is missed it should be taken as soon as remembered on that day, and the next dose should be taken as planned. Doses should not be doubled to make up for a missed dose.
Administration: JADENU tablets should be swallowed whole once daily with water or other liquids, preferably at the same time each day. JADENU should be taken on an empty stomach or with a light meal (containing less than 7% fat content and approximately 250 calories). Examples of light meals include 1 whole wheat English muffin, 1 packet jelly (0.5 ounces), and skim milk (8 fluid ounces) or a turkey sandwich (2 oz. turkey on whole wheat bread with lettuce, tomato, and 1 packet mustard). (See Pharmacology under Actions).
For patients who are unable to swallow whole tablets, JADENU tablets may be crushed and administered by sprinkling the full dose on a soft food (e.g, yogurt or applesauce). Commercial crushers with serrated surfaces should be avoided for crushing a single 90 mg tablet. The dose should be immediately and completely consumed, and followed with a glass of water. The dose should not be stored for future use.