


 Sign Out
Sign Out

The most frequently occurring adverse events (all causalities) in the therapeutic trials of deferasirox were diarrhea, vomiting, nausea, headache, constipation, dyspepsia, abdominal pain, pyrexia, cough, proteinuria, increases in serum creatinine and transaminases, pruritis and skin rash. Gastrointestinal disorders, increases in serum creatinine and skin rash were dose related. Adverse events which most frequently led to dose interruption, dose adjustment, or discontinuation of therapy were skin rash, gastrointestinal disorders, infections, increased creatinine, and increased transaminases.
Clinical Trial Adverse Drug Reactions: Because clinical trials are conducted under very specific conditions the adverse reaction rates observed in the clinical trials may not reflect the rates observed in practice and should not be compared to the rates in the clinical trials of another drug. Adverse drug reaction information from clinical trials is useful for identifying drug-related adverse events and for approximating rates.
In clinical trials in patients with transfusional iron overload, the most frequent reactions reported during chronic treatment with deferasirox in adult and pediatric patients include gastrointestinal disturbances in about 26% of patients (mainly nausea, vomiting, diarrhea, or abdominal pain), and skin rash in about 7% of patients. Mild, non-progressive, dose-dependent increases in serum creatinine occurred in 34% of patients (see Abnormal Hematologic and Clinical Chemistry Findings as follows).
In clinical trials in patients with transfusional iron overload, elevations of liver transaminases as suspected drug-related adverse events were reported in about 2% of patients. The increases in liver transaminases were not dose-dependent. Forty percent of these patients had elevated levels (above the upper limit of normal) prior to receiving deferasirox. Elevations of transaminases greater than 10 times the upper limit of the normal range, suggestive of hepatitis, were uncommon (0.3%). High frequency hearing loss and lenticular opacities (early cataracts) have been observed in <1% of patients treated with deferasirox (see Ear/Nose/Throat and Ophthalmologic under Warnings and Precautions).
In a 1-year, randomized, double-blind, placebo-controlled study in patients with non-transfusion-dependent thalassemia syndromes, the most frequently reported AEs in the deferasirox 10 mg/kg/day group (at least 10%) were headache (16.4%), upper respiratory tract infection (14.5%), oropharyngeal pain (10.9%), pyrexia (10.9%), and rash (10.9%). Table 12 displays adverse events occurring in >5% of deferasirox -treated patients. (See Table 12.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageIn Study 2209, one patient in the placebo 10 mg/kg group experienced an ALT increase to >5 x ULN and >2 x baseline (Table 13). Three deferasirox-treated patients (all in the 10 mg/kg group) had 2 consecutive serum creatinine level increases >33% from baseline and >ULN. Serum creatinine returned to normal in all patients (in one spontaneously and in the other two after drug interruption). (See Table 13.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageA total of 652 patients were treated with deferasirox in therapeutic studies of adult and pediatric patients with β-thalassemia (n=421), rare anemias (n=99) and sickle cell disease (n=132). This population was 46% male, 70% Caucasian and included 292 patients ≤16 years of age. In the sickle cell disease population, 89% of patients were black. A total of 94% of β-thalassemia patients, 70% of patients with rare anemias, and 86% of patients with sickle cell disease patients received therapy for ≥ 48 weeks.
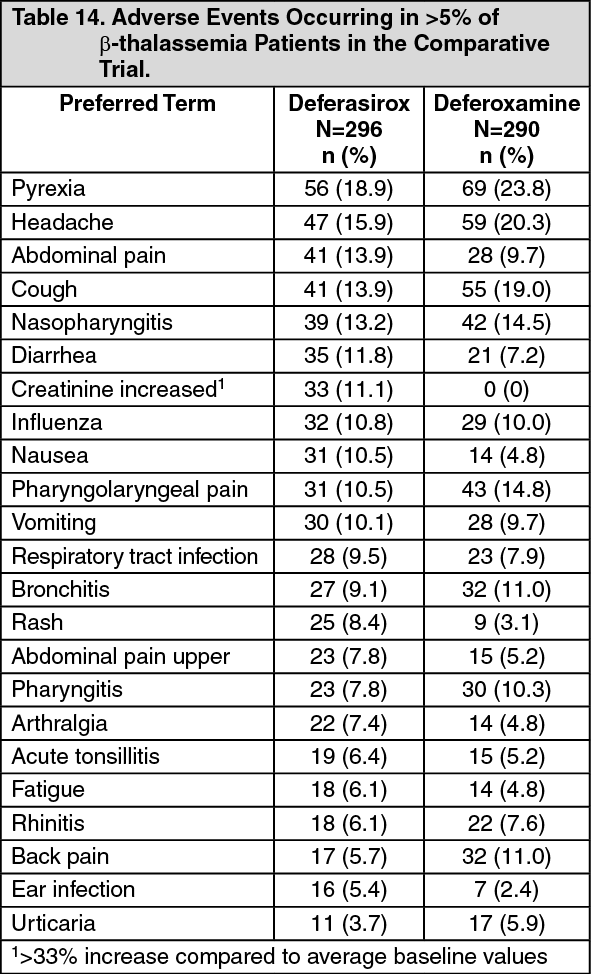
The data in Table 14 displays the adverse events, regardless of causality, occurring in >5% of patients in either treatment group in the primary efficacy study 0107 in which 296 β-thalassemia patients were treated with deferasirox and 290 patients received deferoxamine as an active comparator. Adverse events which most frequently led to dose interruption, dose adjustment, or discontinuation of therapy were skin rash, gastrointestinal disorders, infections, increased creatinine, and increased transaminases (see Abnormal Hematologic and Clinical Chemistry Findings as follows). Discontinuations due to adverse events with a suspected relationship to deferasirox occurred in 7 patients. (See Table 14.)
 Click on icon to see table/diagram/image
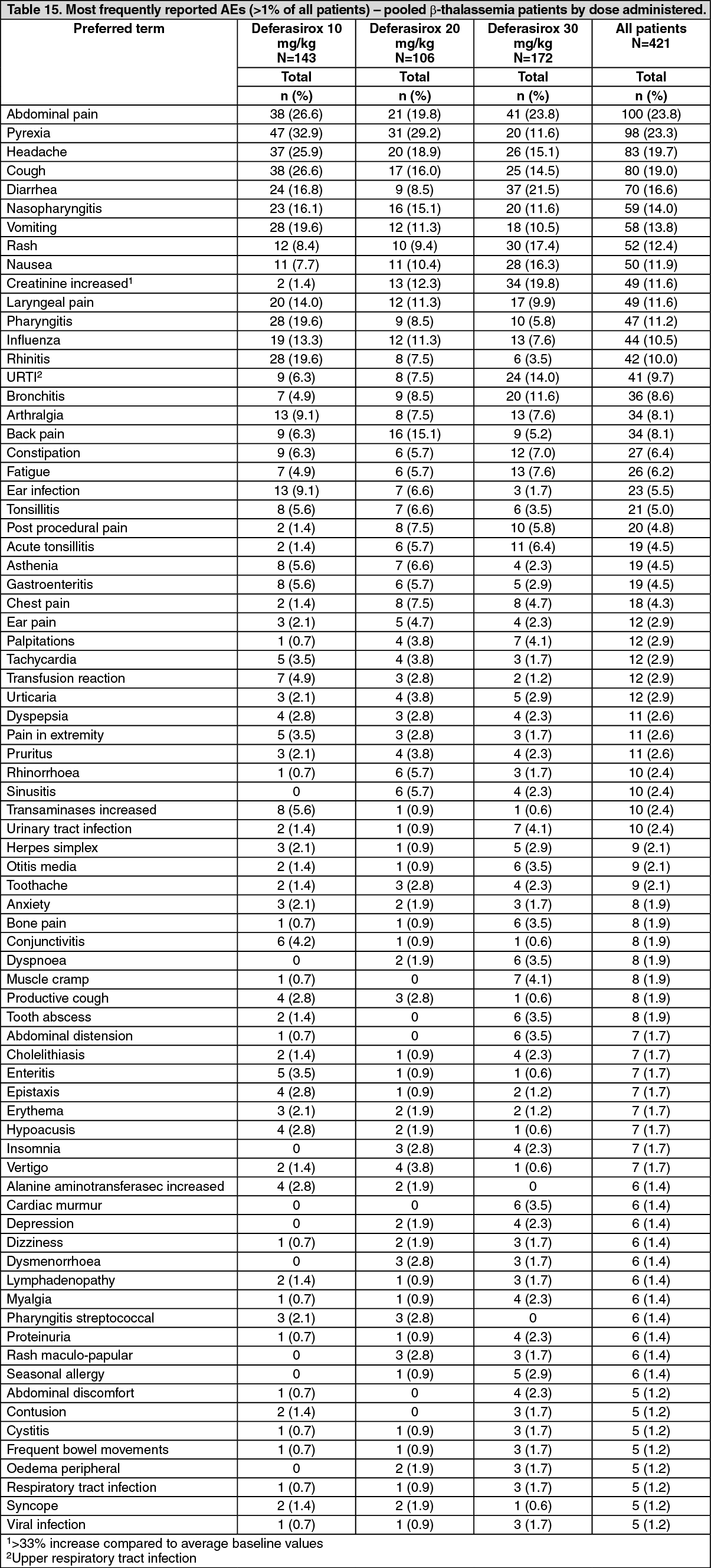
Click on icon to see table/diagram/imageThe data in Table 15 displays the adverse events, regardless of causality, occurring in >1% in the pooled β-thalassemia patients by dose administered. The most frequently reported adverse events were abdominal pain, pyrexia and headache. In the 30 mg/kg dose group, the most frequently reported adverse events were abdominal pain, diarrhea and increased serum creatinine. Skin rash and ALT increase were the only adverse events that resulted in discontinuation. (See Table 15.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageLess Common Clinical Trial Adverse Drug Reactions (<1%): The less common adverse events which occurred in clinical trials and considered to be related to deferasirox are listed as follows: Cardiovascular: QT prolongation1.
General disorders: Pyrexia, oedema, fatigue.
Ear and labyrinth disorders: Deafness.
Eye disorders: Cataract, maculopathy, optic neuritis.
Gastrointestinal: Duodenal ulcer, gastric ulcer (including multiple ulcers) gastritis, gastrointestinal haemorrhage, oesophagitis.
Hepatic/Biliary/Pancreatic: Cholelithiasis, hepatitis, acute pancreatitis2.
Nervous system: Dizziness.
Psychiatric disorders: Anxiety, sleep disorder.
Renal and urinary disorders: Renal disorder (Fanconi syndrome).
Respiratory, thoracic and mediastinal disorders: Pharyngolaryngeal pain.
Skin and subcutaneous tissue disorders: Pigmentation disorder, erythema multiforme.
1. Three cases of QT interval prolongation were reported in the clinical trials, however, a causal relationship to study drug was not established.
2. Cases of serious acute pancreatitis were observed with and without documented underlying biliary conditions.
Abnormal Hematologic and Clinical Chemistry Findings: In the comparative study 0107, 113 patients treated with deferasirox had non-progressive increases in serum creatinine > 33% above baseline (Table 16). Twenty-five (25) patients required dose reductions. Increases in serum creatinine appeared to be dose-related. Of the 17 patients with elevations in SGPT/ALT levels > 5 times the ULN at consecutive visits, one discontinued deferasirox therapy. One patient experienced increases in transaminases to >10x ULN which normalized upon drug discontinuation but then increased sharply upon rechallenge. Increases in transaminases did not appear to be dose-related and most of these patients had elevated transaminases prior to receiving deferasirox therapy. (See Table 16.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageA total of 652 patients were treated with deferasirox in clinical studies 107, 108, and 109. Of these patients, 237 (36%) had an increase in serum creatinine >33% on at least 2 consecutive visits, 68 (11%) of whom underwent dose reduction. The remainder returned to serum creatinine <33% above baseline without dose reduction. Of the 68 patients who underwent dose reduction, 17 (25%) returned to normal, 41 (60%) remained elevated at >33% without progression and the remaining 10 (15%) fluctuated between baseline and 33%.
Based on limited data in patients with sickle cell disease (N=132) and other rare anemias (N=99), the type and frequency of adverse events observed were similar to those observed in patients with β-thalassemia. The adverse event profile in patients <16 years of age was similar to that seen in adults, regardless of disease state.
In 49 adult β-thalassemia patients treated for greater than 1 year and up to 3 years, the type and frequency of adverse events was similar to that seen in patients treated for up to 1 year.
Post-Market Adverse Drug Reactions: Cases of acute renal failure (some with fatal outcome) have been reported following the post-marketing use of deferasirox. Rarely biopsy proven interstitial nephritis has also been reported.
Hypocalcemia has been reported to occur during deferasirox therapy.
Spontaneously reported adverse reactions, presented below, are reported voluntarily and it is not always possible to reliably establish frequency or a causal relationship to drug exposure.
Post-Market Information: Since the International Birth Date (November 2, 2005), the cumulative exposure to marketed deferasirox is 123,619 patient-years as of October 31, 2011.
Paediatric population: Renal tubulopathy has been reported in patients treated with deferasirox. The majority of these patients were children and adolescents with beta-thalassemia and serum ferritin levels <1,500 μg/L.
Renal and urinary disorders: Acute renal failure (mostly serum creatinine increases ≥ 2x upper limit of normal, and usually reversible after treatment interruption), hematuria, renal tubular necrosis.
Skin and subcutaneous tissue disorders: Stevens-Johnson syndrome, hypersensitivity vasculitis, urticaria, erythema multiforme, alopecia, toxic epidermal necrolysis (TEN).
Immune system disorders: Hypersensitivity reactions (including anaphylaxis and angioedema).
Gastrointestinal disorders: Duodenal ulcer, gastric ulcer, gastrointestinal bleeding, gastrointestinal perforation.
Blood and lymphatic system disorders: Agranulocytosis, neutropenia, thrombocytopenia and aggravated anemia.
Hepatic/Biliary/Pancreatic: Hepatic failure.
View ADR Monitoring Form