Dexketoprofen trometamol.
Each tablet contains dexketoprofen 25 mg as dexketoprofen trometamol.
The tablets can be divided into equal halves.
Excipients/Inactive Ingredients: Tablet core: maize starch, microcrystalline cellulose, sodium starch glycolate, glycerol distearate.
Film-Coating: 1. Dry lacquer composed of: hypromellose, titanium dioxide, macrogol 6000.
2. Propylene glycol.
Pharmacotherapeutic group: Propionic acid derivatives. ATC code: M01AE17.
Pharmacology: Pharmacodynamics: Dexketoprofen trometamol is the tromethamine salt of S-(+)-2-(3-benzoylphenyl) propionic acid, an analgesic, anti-inflammatory and antipyretic drug, which belongs to the non-steroidal anti-inflammatory group of drugs (M01AE).
Mechanism of action: The mechanism of action of non-steroidal anti-inflammatory drugs is related to the reduction of prostaglandin synthesis by the inhibition of cyclooxygenase pathway. Specifically, there is an inhibition of the transformation of arachidonic acid into cyclic endoperoxides, PGG2 and PGH2, which produce prostaglandins PGE1, PGE2, PGF2α and PGD2 and also prostacyclin PGI2 and thromboxanes (TxA2 and TxB2). Furthermore, the inhibition of the synthesis of prostaglandins could affect other inflammation mediators such as kinins, causing an indirect action which would be additional to the direct action.
Pharmacodynamic effects: Dexketoprofen has been demonstrated to be an inhibitor for COX-1 and COX-2 activities in experimental animals and humans.
Clinical efficacy and safety: Clinical studies performed on several pain models demonstrated effective analgesic activity of dexketoprofen. The onset of the analgesic activity was obtained in some studies at 30 minutes post-administration. The analgesic effect persists for 4 to 6 hours.
Pharmacokinetics: Absorption: After oral administration of dexketoprofen trometamol to humans, the Cmax is reached at 30 min (range 15 to 60 min).
When administered concomitantly with food, the AUC does not change, however the Cmax of dexketoprofen decreases and its absorption rate is delayed (increased tmax).
Distribution: The distribution half-life and elimination half-life values of dexketoprofen are 0.35 and 1.65 hours, respectively. As with other drugs with a high plasma protein binding (99%), its volume of distribution has a mean value below 0.25 l/kg.
In multiple-dose pharmacokinetic studies, it was observed that the AUC after the last administration is not different from that obtained following a single dose, indicating that no drug accumulation occurs.
Biotransformation and elimination: After administration of dexketoprofen trometamol only the S-(+) enantiomer is obtained in urine, demonstrating that no conversion to the R-(-) enantiomer occurs in humans.
The main elimination route for dexketoprofen is glucuronide conjugation followed by renal excretion.
Toxicology: Preclinical safety data: Non-clinical data revealed no special hazard for humans based on conventional studies of safety pharmacology, genotoxicity, and immunopharmacology. The chronic toxicity studies carried out in mice and monkeys gave a No Observed Adverse Effect Level (NOAEL) at doses 2 fold higher than maximum recommended human dose. In monkey, at higher doses, the main adverse effect observed were blood in faeces, decreased body weight gain and, at the highest dose, erosive gastrointestinal lesions. These effects appeared at doses determining a drug exposure 14-18 fold higher than that at the maximum recommended human dose.
There are no studies on the carcinogenic potential in animals.
As it has been recognised for the whole pharmacological class of NSAIDs, dexketoprofen trometamol may cause changes of embryo-foetal survival in animal models, both indirectly, through the gastrointestinal toxicity on the pregnant mothers, and directly upon the development of the foetus.
Symptomatic treatment of pain of mild to moderate intensity, such as musculo-skeletal pain, dysmenorrhoea, dental pain.
Adults: According to the nature and severity of pain, the recommended dosage is generally 12.5 mg every 4-6 hours or 25 mg every 8 hours. The total daily dose should not exceed 75 mg.
Undesirable effects may be minimised by using the lowest effective dose for the shortest duration necessary to control symptoms (see Precautions).
Ketesse tablets are not intended for long term use and the treatment must be limited to the symptomatic period.
Elderly: In elderly patients it is recommended to start the therapy at the lower end of the dosage range (50 mg total daily dose). The dosage may be increased to that recommended for the general population only after good general tolerance has been ascertained.
Hepatic impairment: Patients with mild to moderate hepatic impairment should start therapy at reduced doses (50 mg total daily dose) and be closely monitored. Ketesse tablets should not be used in patients with severe hepatic impairment.
Renal impairment: The initial dosage should be reduced to 50 mg total daily dose in patients with mildly impaired renal function (creatinine clearance 60 - 89 ml/min) (see Precautions). Ketesse tablets should not be used in patients with moderate to severe renal impairment (creatinine clearance ≤ 59 ml/min) (see Contraindications).
Paediatric Population: Ketesse tablets has not been studied in children and adolescent. Therefore, the safety and efficacy in children and adolescents have not been established and the product should not be used in children and adolescent.
Method of administration: The tablet should be swallowed with a sufficient amount of fluid (e.g. one glass of water).
Concomitant administration with food delays the absorption rate of the drug (see Pharmacology: Pharmacokinetics under Actions), thus in case of acute pain it is recommended that administration is at least 30 minutes before meals.
The symptomatology following overdose is not known. Similar medicinal products have produced gastrointestinal (vomiting, anorexia, abdominal pain) and neurological (somnolence, vertigo, disorientation, headache) disorders.
In case of accidental or excessive intake, immediately institute symptomatic therapy according to the patient's clinical condition. Activated charcoal should be administered if more than 5 mg/kg has been ingested by an adult or a child within an hour.
Dexketoprofen trometamol may be removed by dialysis.
Ketesse tablets must not be administered in the following cases: patients hypersensitive to the active substance, to any other NSAIDs, or to any of the excipients of the product; patients in whom substances with a similar action (e.g. acetylsalicylic acid, or other NSAIDs) precipitate attacks of asthma, bronchospasm, acute rhinitis, or cause nasal polyps, urticaria or angioneurotic oedema; known photoallergic or phototoxic reactions during treatment with ketoprofen or fibrates; patients with history of gastrointestinal bleeding or perforation, related to previous NSAIDs therapy; patients with active peptic ulcer/gastrointestinal haemorrhage or any history of gastrointestinal bleeding, ulceration or perforation; patients with chronic dyspepsia; patients who have other active bleedings or bleeding disorders; patients with Crohn's disease or ulcerative colitis; patients with severe heart failure; patients with moderate to severe renal impairment (creatinine clearance ≤59 ml/min); patients with severely impaired hepatic function (Child-Pugh score 10-15); patients with haemorrhagic diathesis and other coagulation disorders; patients with severe dehydration (caused by vomiting, diarrhoea or insufficient fluid intake); during the third trimester of pregnancy and lactation period (see Use in Pregnancy & Lactation).
Warning or precautions (according to Ministry of Public Health announcement): 1. Do not use if allergic with the ingredients in this product or any of the following conditions such as asthma, urticaria or acute sinusitis that occurs from an aspirin or NSAIDs allergy.
2. Avoid taking this medication if pregnant at the last trimester unless prescribed by a doctor.
3. Do not take this medication if the patient has an active gastrointestinal bleeding or ulcers.
4. Do not take this medication if the patient has severe liver or kidney disease.
5. Do not take this medication if the patient has dengue fever.
6. This medication may increase risk of gastrointestinal bleeding or ulcer.
7. Long term use at higher doses of this medication may increase risk of ischemic stroke, and coronary heart diseases.
8. Caution in taking this medication in an abnormal function of cardiovascular or kidney conditions, it may be associated with water retention and edema.
9. Caution when using this medication in people with high blood pressure or elderly.
10. Avoid taking this medicine if suspected with dengue fever or platelets level abnormalities from other causes as it affects platelet aggregation.
Administer with caution in patients with a history of allergic conditions.
The use of Ketesse with concomitant other NSAIDs including cyclooxygenase-2 selective inhibitors should be avoided.
Undesirable effects may be minimised by using the lowest effective dose for the shortest duration necessary to control symptoms (see Dosage & Administration, and Gastrointestinal safety and Cardiovascular and cerebrovascular safety as follows).
Gastrointestinal safety: Gastrointestinal bleeding, ulceration or perforation which can be fatal, have been reported with all NSAIDs at anytime during treatment, with or without warning symptoms or a previous history of serious gastrointestinal events. When gastrointestinal bleeding or ulceration occurs in patients receiving Ketesse, the treatment should be withdrawn.
The risk of gastrointestinal bleeding, ulceration or perforation is higher with increasing NSAIDs doses, in patients with a history of ulcer, particularly if complicated with haemorrhage or perforation (see Contraindications), and in the elderly.
Renal Safety: Caution should be exercised in patients with impairment of renal functions. In these patients, the use of NSAIDs may result in deterioration of renal function, fluid retention and oedema. Caution is also required in patients receiving diuretic therapy or those who could develop hypovolaemia as there is an increased risk of nephrotoxicity.
Adequate fluid intake should be ensured during treatment to prevent dehydration and possibly associated increased renal toxicity.
As with all NSAIDs, it can increase plasma urea nitrogen and creatinine. As with other inhibitors of prostaglandin synthesis, it can be associated with adverse effects on the renal system which can lead to glomerular nephritis, interstitial nephritis, renal papillary necrosis, nephrotic syndrome and acute renal failure.
Elderly patients are more likely to be suffering from impaired renal function (see Dosage & Administration).
Liver Safety: Caution should be exercised in patients with impairment of hepatic functions.
As with other NSAIDs, it can cause transient small increases in some liver parameters, and also significant increases in SGOT and SGPT. In case of a relevant increase in such parameters, therapy must be discontinued.
Elderly patients are more likely to be suffering from impaired hepatic function (see Dosage & Administration).
Cardiovascular and cerebrovascular safety: Appropriate monitoring and advice are required for patients with history of hypertension and/or mild to moderate heart failure. Special caution should be exercised in patients with a history of cardiac disease, in particular those with previous episodes of heart failure as there is an increased risk of triggering heart failure, since fluid retention and oedema have been reported in association with NSAIDs therapy.
Clinical trial and epidemiological data suggest that use of some NSAIDs (particularly at high doses and in long term treatment) may be associated with a small increased risk of arterial thrombotic events (for example myocardial infarction or stroke). There are insufficient data to exclude such a risk for dexketoprofen.
Consequently, patients with uncontrolled hypertension, congestive heart failure, established ischaemic heart disease, peripheral arterial disease, and/or cerebrovascular disease should only be treated with dexketoprofen after careful consideration. Similar consideration should be made before initiating longer-term treatment of the patients with risk factors for cardiovascular disease (e.g. hypertension, hyperlipidaemia, diabetes mellitus, smoking).
All non-selective NSAIDs can inhibit platelet aggregation and prolong bleeding time via inhibition of prostaglandin synthesis. Therefore, the use of dexketoprofen in patients who are receiving other therapy that interferes with haemostasis, such as warfarin or other coumarins or heparins is not recommended (see Interactions).
Elderly patients are more likely to be suffering from impaired cardiovascular function (see Dosage & Administration).
Skin reactions: Serious skin reactions, some of them fatal, including exfoliative dermatitis, Stevens-Johnson syndrome, and toxic epidermal necrolysis, have been reported very rarely in association with the use of NSAIDs. Patients appear to be at highest risk of these reactions early in the course of therapy, the onset of the reaction occurring in the majority of cases within the first month of treatment. Ketesse should be discontinued at the first appearance of skin rash, mucosal lesions, or any other sign of hypersensitivity.
Masking of symptoms of underlying infections: Dexketoprofen can mask symptoms of infection, which may lead to delayed initiation of appropriate treatment and thereby worsening the outcome of the infection. This has been observed in bacterial community acquired pneumonia and bacterial complications to varicella. When this medicine is administered for pain relief in relation to infection, monitoring of infection is advised. In non-hospital settings, the patient should consult a doctor if symptoms persist or worsen.
Exceptionally, varicella can be at the origin of serious cutaneous and soft tissues infectious complications. To date, the contributing role of NSAIDs in the worsening of these infections cannot be ruled out. Thus, it is advisable to avoid use of Ketesse in case of varicella.
Other information: Particular caution is required in patients with: congenital disorder of porphyrin metabolism (e.g. acute intermittent porphyria); dehydration; directly after major surgery.
If the physician considers long-term dexketoprofen therapy to be necessary, hepatic and renal function and the blood count should be regularly checked.
Severe acute hypersensitivity reactions (anaphylactic shock, for example) have been observed on very rare occasions. Treatment must be discontinued at the first signs of severe hypersensitivity reactions following intake of Ketesse. Depending on the symptoms, any medically required procedures must be initiated by specialist healthcare professionals.
Patients with asthma combined with chronic rhinitis, chronic sinusitis, and/or nasal polyposis have a higher risk of allergy to acetylsalicylic acid and/or NSAIDs than the rest of the population. Administration of this medicinal product can cause asthma attacks or bronchospasm, particularly in subjects allergic to acetylsalicylic acid or NSAIDs (see Contraindications).
Ketesse should be administered with caution to patients suffering from haematopoietic disorders, systemic lupus erythematosus or mixed connective tissue disease.
This medicine contains less than 1 mmol sodium (23 mg) per tablet, that is to say essentially 'sodium-free'.
Effects on ability to drive and use machines: Ketesse tablets may cause undesirable effects such as dizziness, visual disturbances or drowsiness. The ability to react and the ability to take part actively in road traffic and to operate machines may be impaired in these cases.
Use in Children: The safe use in children and adolescents has not been established.
Use in the Elderly: The elderly have an increased frequency of adverse reactions to NSAIDs especially gastrointestinal bleeding and perforation which may be fatal (see Dosage & Administration). These patients should commence treatment on the lowest dose available.
As with all NSAIDs, any history of oesophagitis, gastritis and/or peptic ulcer must be sought in order to ensure their total cure before starting treatment with dexketoprofen. Patients with gastrointestinal symptoms or history of gastrointestinal disease should be monitored for digestive disturbances, especially gastrointestinal bleeding.
NSAIDs should be given with care to patients with a history of gastrointestinal disease (ulcerative colitis, Crohn's disease) as their condition may be exacerbated (see Adverse Reactions).
Combination therapy with protective agents (e.g. misoprostol or proton pump inhibitors) should be considered for these patients, and also for patients requiring concomitant low dose acetylsalicylic acid, or other drugs likely to increase gastrointestinal risk (see following text and Interactions).
Patients with a history of gastrointestinal toxicity, particularly when elderly, should report any unusual abdominal symptoms (especially gastrointestinal bleeding) particularly in the initial stages of treatment.
Caution should be advised in patients receiving concomitant medications which could increase the risk of ulceration or bleeding, such as oral corticosteroids, anticoagulants such as warfarin, selective serotonin-reuptake inhibitors or anti-platelet agents such as acetylsalicylic acid (see Interactions).
Ketesse tablets are contraindicated during third trimester of pregnancy and lactation (see Contraindications).
Pregnancy: Inhibition of prostaglandin synthesis may adversely affect the pregnancy and/or the embryo/foetal development. Data from epidemiological studies raise concern about an increased risk of miscarriage and of cardiac malformation and gastroschisis after use of a prostaglandin synthesis inhibitor in early pregnancy. The absolute risk for cardiovascular malformation was increased from less than 1%, up to approximately 1.5%. The risk is believed to increase with dose and duration of therapy. In animals, administration of a prostaglandin synthesis inhibitor has been shown to result in increased pre- and post-implantation loss and embryo-foetal lethality. In addition, increased incidences of various malformations including cardiovascular, have been reported in animals given a prostaglandin synthesis inhibitor during the organogenetic period. Nevertheless, animal studies with dexketoprofen haven't shown reproductive toxicity (see Pharmacology: Toxicology: Preclinical safety data under Actions). During the first and second trimester of pregnancy, dexketoprofen should not be given unless clearly necessary. If dexketoprofen is used by a woman attempting to conceive, or during the first and second trimester of pregnancy, the dose should be kept as low and duration of treatment as short as possible.
During the third trimester of pregnancy, all prostaglandin synthesis inhibitors may expose the fetus to: cardiopulmonary toxicity (with premature closure of the ductus arteriosus and pulmonary hypertension); renal impairment, which may progress to renal failure with oligohydramnios.
The mother and the neonate, at the end of pregnancy, to: possible prolongation of bleeding time, an anti-aggregating effect which may occur even at very low doses; inhibition of uterine contractions resulting in delayed or prolonged labour.
Breast-feeding: It is not known whether dexketoprofen is excreted in human milk. Ketesse is contraindicated during breast-feeding (see Contraindications).
Fertility: As with other NSAIDs, the use of dexketoprofen trometamol may impair female fertility and is not recommended in women attempting to conceive. In women who have difficulties conceiving or who are undergoing investigation of infertility, withdrawal of dexketoprofen should be considered.
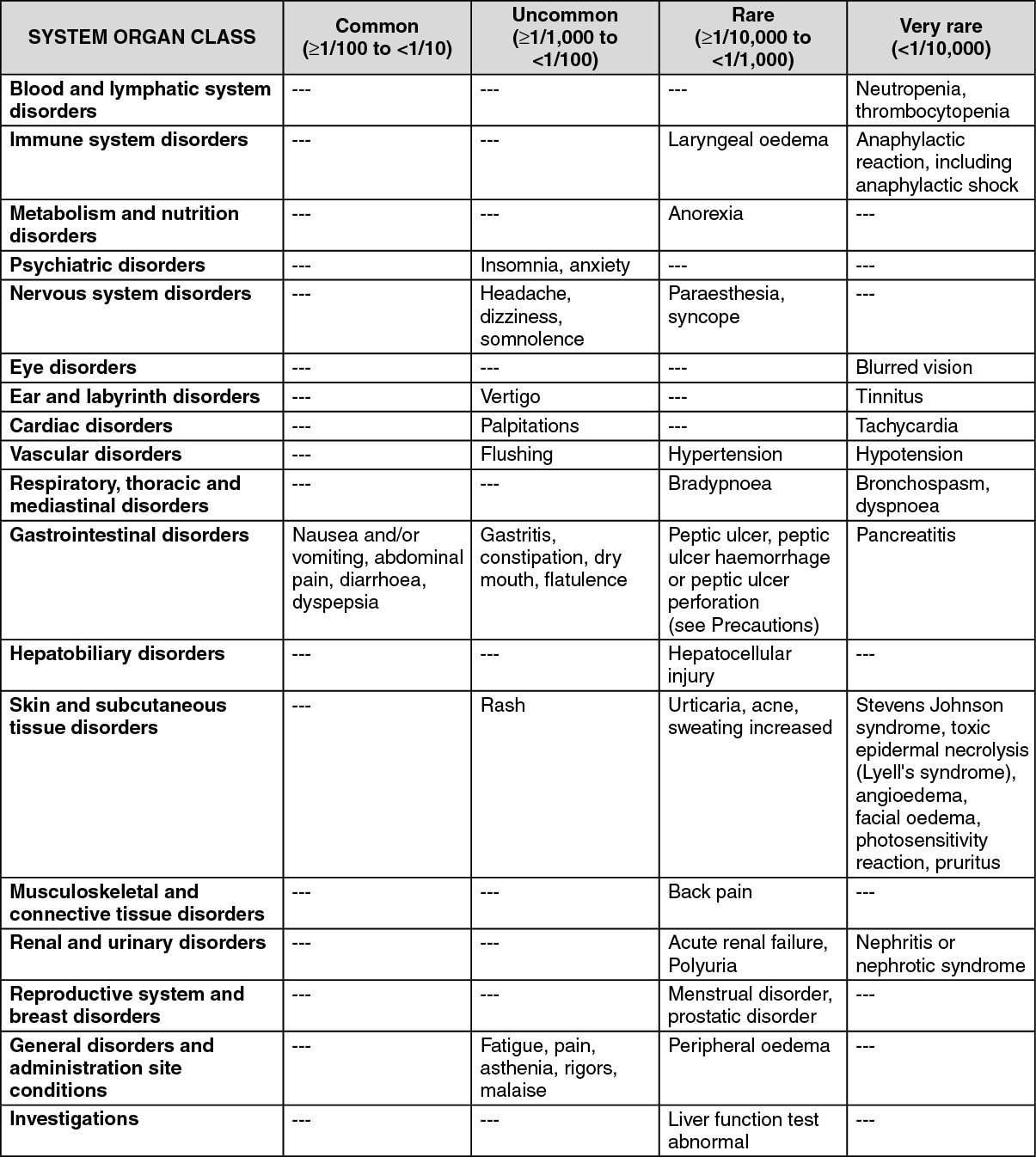
The adverse events reported as at least possibly related with dexketoprofen in clinical trials, as well as the adverse reactions reported after the marketing of Ketesse tablets are tabulated as follows, classified by system organ class and ordered by frequency: See table.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
The most commonly-observed adverse events are gastrointestinal in nature. Peptic ulcers, perforation or gastrointestinal bleeding, sometimes fatal, particularly in the elderly, may occur (see Precautions). Nausea, vomiting, diarrhoea, flatulence, constipation, dyspepsia, abdominal pain, melaena, haematemesis, ulcerative stomatitis, exacerbation of colitis and Crohn's disease (see Precautions) have been reported following administration. Less frequently, gastritis has been observed. Oedema, hypertension and cardiac failure have been reported in association with NSAIDs treatment.
As with other NSAIDs the following undesirable effects may appear aseptic meningitis, which might predominantly occur in patients with systemic lupus erythematosus or mixed connective tissue disease; haematological reactions (purpura, aplastic and haemolytic anaemia, and rarely agranulocytosis and medullar hypoplasia).
Bullous reactions including Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis (very rare).
Clinical trial and epidemiological data suggest that use of some NSAIDs (particularly at high doses and in long term treatment) may be associated with a small increased risk of arterial thrombotic events (for example myocardial infarction or stroke) (see Precautions).
The following interactions apply to non-steroidal anti-inflammatory drugs (NSAIDs) in general: Inadvisable combinations: Other NSAIDs (including cyclooxygenase-2 selective inhibitors) and high doses of salicylates (≥ 3 g/day): administration of several NSAIDs together may increase the risk of gastrointestinal ulcers and bleeding, via a synergistic effect.
Anticoagulants: NSAIDs may enhance the effects of anti-coagulants, such as warfarin (see Precautions), due to the high plasma protein binding of dexketoprofen and the inhibition of platelet function and damage to the gastroduodenal mucosa. If the combination cannot be avoided, close clinical observation and monitoring of laboratory values should be carried out.
Heparins: increased risk of haemorrhage (due to the inhibition of platelet function and damage to the gastroduodenal mucosa). If the combination cannot be avoided, close clinical observation and monitoring of laboratory values should be carried out.
Corticosteroids: there is an increased risk of gastrointestinal ulceration or bleeding (see Precautions).
Lithium (described with several NSAIDs): NSAIDs increase blood lithium levels, which may reach toxic values (decreased renal excretion of lithium). This parameter therefore requires monitoring during the initiation, adjustment and withdrawal of treatment with dexketoprofen.
Methotrexate, used at high doses of 15 mg/week or more: increased haematological toxicity of methotrexate via a decrease in its renal clearance by anti-inflammatory agents in general.
Hydantoines and sulphonamides: the toxic effects of these substances may be increased.
Combinations requiring precautions: Diuretics, ACE inhibitors, antibacterial aminoglycosides and angiotensin II receptor antagonists: Dexketoprofen may reduce the effect of diuretics and antihypertensive drugs. In some patients with compromised renal function (e.g. dehydrated patients or elderly patients with compromised renal function), the coadministration of agents that inhibit cyclo-oxygenase and ACE inhibitors, angiotensin II receptor antagonists or antibacterial aminoglycosides may result in further deterioration of renal function, which is usually reversible. In case of combined prescription of dexketoprofen and a diuretic, it is essential to ensure that the patient is adequately hydrated and to monitor renal function at the start of the treatment (see Precautions).
Methotrexate, used at low doses, less than 15 mg/week: increased haematological toxicity of methotrexate via a decrease in its renal clearance by anti-inflammatory agents in general. Weekly monitoring of blood count during the first weeks of the combination. Increased surveillance in the presence of even mildly impaired renal function, as well as in the elderly.
Pentoxyfilline: increased risk of bleeding. Increase clinical monitoring and check bleeding time more often.
Zidovudine: risk of increased red cell line toxicity via action on reticulocytes, with severe anaemia occurring one week after the NSAIDs is started. Check complete blood count and reticulocyte count one to two weeks after starting treatment with the NSAIDs.
Sulfonylureas: NSAIDs can increase the hypoglycaemic effect of sulfonylureas by displacement from plasma protein binding sites.
Combinations needing to be taken into account: Beta-blockers: treatment with NSAIDs may decrease their antihypertensive effect via inhibition of prostaglandin synthesis.
Cyclosporin and tacrolimus: nephrotoxicity may be enhanced by NSAIDs via renal prostaglandin mediated effects. During combination therapy, renal function has to be measured.
Thrombolytics: increased risk of bleeding.
Anti-platelet agents and selective serotonin reuptake inhibitors (SSRIs): increased risk of gastrointestinal bleeding (see Precautions).
Probenecid: plasma concentrations of dexketoprofen may be increased; this interaction can be due to an inhibitory mechanism at the site of renal tubular secretion and of glucuronoconjugation and requires adjustment of the dose of dexketoprofen.
Cardiac glycosides: NSAIDs may increase plasma glycoside concentration.
Mifepristone: There is a theoretical risk that prostaglandin synthetase inhibitors may alter the efficacy of mifepristone. Limited evidence suggests that co-administration of NSAIDs on the day of prostaglandin administration does not adversely influence the effects of mifepristone or the prostaglandin on cervical ripening or uterine contractility and does not reduce the clinical efficacy of medical termination of pregnancy.
Quinolone Antibiotics: Animal data indicate that high doses of quinolones in combination with NSAIDs can increase the risk of developing convulsions.
Tenofovir: concomitant use with NSAID can increase plasma urea nitrogen and creatinine, renal function should be monitored in order to control a potential synergic influence on renal function.
Deferasirox: concomitant use with NSAIDs can increase the risk of gastrointestinal toxicity. Close clinical monitoring is required when deferasirox is combined with these substances.
Pemetrexed: concomitant use with NSAIDs may decrease pemetrexed elimination, therefore caution should be made when administering higher doses of NSAIDs. In patients with mild to moderate renal insufficiency (creatinine clearance from 45 to 79 ml/min), the concomitant administration of pemetrexed with NSAIDs doses should be avoided for 2 days before and 2 days following pemetrexed administration.
Incompatibilities: Not applicable.
Instructions for use/handling: No special requirements.
Store below 30°C; keep the blister packs in the outer carton in order to protect from light.
Shelf-life: 3 years.
M01AE17 - dexketoprofen ; Belongs to the class of propionic acid derivatives of non-steroidal antiinflammatory and antirheumatic products.
Ketesse FC tab 25 mg
2 × 10's


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out
