Dexmedetomidine hydrochloride.
Each ml contains Dexmedetomidine Hydrochloride USP 118 mcg equivalent to Dexmedetomidine 100 mcg, Water for Injection USP Q.S. to 1 ml.
HYDEX (dexmedetomidine Hydrochloride Injection) is a clear, colourless solution filled in a clear glass vial, when examined under suitable condition visibly; it is free from foreign particles. HYDEX (dexmedetomidine hydrochloride) injection is a sterile, nonpyrogenic ready to use solution suitable for intravenous infusion. Dexmedetomidine hydrochloride is the S-enantiomer of medetomidine and is chemically described as (+)-4-(S)-[1-(2,3-dimethylphenyl)ethyl]-1H-imidazole monohydrochloride. HYDEX has a molecular weight of 236.7 and the empirical formula is C13H16N2·HCl.
Excipients/Inactive Ingredients: Sodium chloride, Water for Injection.
Pharmacology: Pharmacodynamics: HYDEX is a relatively selective alpha2-adrenoceptor agonist with sedative properties. Alpha2 selectivity is observed in animals following slow intravenous infusion of low and medium doses (10-300 mcg/kg). Both alpha1 and alpha2 activity is observed following slow intravenous infusion of high doses (≥1000 mcg/kg) or with rapid intravenous administration.
It has a sympatholytic effect through decrease of the release of noradrenaline (norepinephrine) in sympathetic nerve endings. The sedative effects are mediated through decreased firing of locus coeruleus, the predominant noradrenergic nucleus, situated in the brainstem. Dexmedetomidine has analgesic and anaesthetic/analgesic-sparing effects. The cardiovascular effects depend on the dose; with lower infusion rates the central effects dominate leading to decrease in heart rate and blood pressure. With higher doses, peripheral vasoconstricting effects prevail leading to an increase in systemic vascular resistance and blood pressure, while the bradycardic effect is further emphasised. Dexmedetomidine is relatively free from respiratory depressive effects when given as monotherapy to healthy subjects.
Pharmacokinetics: Dexmedetomidine exhibits a rapid distribution phase with a distribution half-life (T½) of approximately 6 minutes; a terminal elimination half-life (T½) of approximately 2 hours; and steady-state volume of distribution (Vss) of approximately 118 L. Clearance is estimated to be approximately 39 L/hr. The mean body weight associated with this clearance estimate was 72 kg. Dexmedetomidine exhibits linear kinetics in the dosage range of 0.2 to 0.7 mcg/kg/hr when administered by IV infusion for up to 24 hours. Target concentrations are usually in the range of 0.3 to 0.6 ng/mL. Protein binding to both albumin and α1 acid glycoprotein is 94%. Dexmedetomidine undergoes almost complete biotransformation with very little unchanged in urine and feces. Biotransformation involves both direct glucuronidation as well as cytochrome P450 mediated metabolism. There are no active metabolites. Similar kinetic data was noted in pediatric patients. Onset of action with loading infusion is 10 to 20 minutes, and the duration of action after the infusion is stopped is 10 to 30 minutes.
HYDEX is indicated for: Intensive Care Unit Sedation: Sedation of initially intubated and mechanically ventilated patients during treatment in an intensive care setting. Administer HYDEX by continuous infusion not to exceed 24 hours.
Procedural Sedation: Sedation of non-intubated patients prior to and/or during surgical and other procedures.
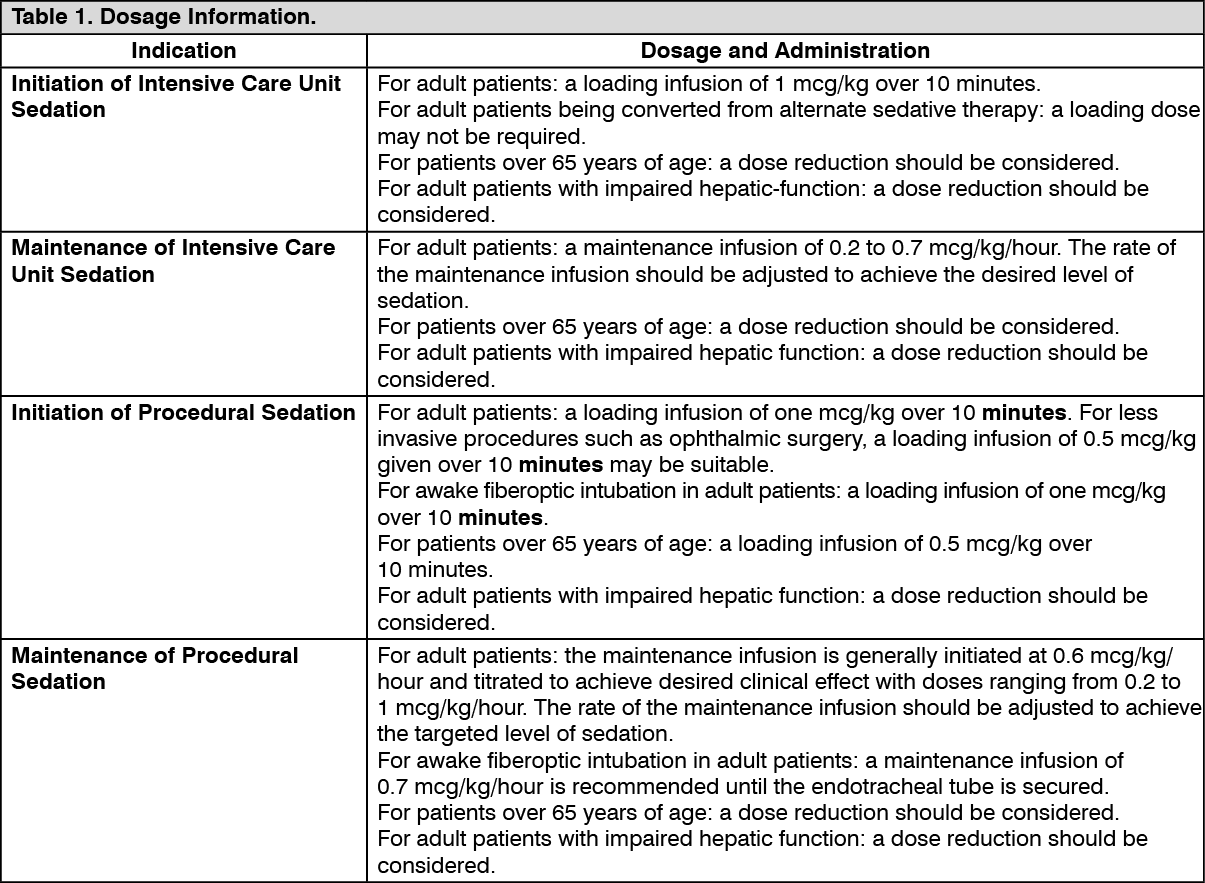
Recommended Dosage: Dosing Guidelines: HYDEX dosing should be individualized and titrated to desired clinical response.
HYDEX is not indicated for infusions lasting longer than 24 hours.
HYDEX should be administered using a controlled infusion device. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Preparation of Solution: Strict aseptic technique must always be maintained during handling of HYDEX. Parenteral drug products should be inspected visually for particulate matter and discoloration prior to administration, whenever solution and container permit.
HYDEX must be diluted with 0.9% sodium chloride solution to achieve required concentration (4 mcg/mL) prior to administration. Preparation of solutions is the same, whether for the loading dose or maintenance infusion. To prepare the infusion, withdraw 2 mL of HYDEX Injection Concentrate, and add to 48 mL of 0.9% sodium chloride injection to a total of 50 mL. Shake gently to mix well.
Route of Administration: Intravenous infusion.
Symptoms: Several cases of dexmedetomidine overdose have been reported both in the clinical trial and the post-marketing data. The reported highest infusion rates of dexmedetomidine in these cases have reached up to 60 µg/kg/h for 36 minutes and 30 µg/kg/h for 15 minutes in a 20-month-old child and in an adult, respectively. The most common adverse reactions reported in conjunction with overdose in these cases included bradycardia, hypotension, oversedation, somnolence and cardiac arrest.
Management: In cases of overdose with clinical symptoms, dexmedetomidine infusion should be reduced or stopped. Expected effects are primarily cardiovascular and should be treated as clinically indicated. At high concentration hypertension may be more prominent than hypotension. In clinical studies, cases of sinus arrest reversed spontaneously or responded to treatment with atropine and glycopyrrolate. Resuscitation was required in isolated cases of severe overdose resulting in cardiac arrest.
Drug Administration: HYDEX should be administered only by persons skilled in the management of patients in the intensive care or operating room setting. Due to the known pharmacological effects of HYDEX, patients should be continuously monitored while receiving HYDEX.
Hypotension, Bradycardia, and Sinus Arrest: Clinically significant episodes of bradycardia and sinus arrest have been reported with dexmedetomidine administration in young, healthy adult volunteers with high vagal tone or with different routes of administration including rapid intravenous or bolus administration. Reports of hypotension and bradycardia have been associated with dexmedetomidine infusion. If medical intervention is required, treatment may include decreasing or stopping the infusion of HYDEX, increasing the rate of intravenous fluid administration, elevation of the lower extremities, and use of pressor agents. Because HYDEX has the potential to augment bradycardia induced by vagal stimuli, clinicians should be prepared to intervene. The intravenous administration of anticholinergic agents (e.g., glycopyrrolate, atropine) should be considered to modify vagal tone. In clinical trials, glycopyrrolate or atropine were effective in the treatment of most episodes of dexmedetomidine-induced bradycardia. However, in some patients with significant cardiovascular dysfunction, more advanced resuscitative measures were required. Caution should be exercised when administering HYDEX to patients with advanced heart block and/or severe ventricular dysfunction. Because dexmedetomidine decreases sympathetic nervous system activity, hypotension and/or bradycardia may be expected to be more pronounced in patients with hypovolemia, diabetes mellitus, or chronic hypertension and in elderly patients. In clinical trials where other vasodilators or negative chronotropic agents were co-administered with dexmedetomidine an additive pharmacodynamic effect was not observed. Nonetheless, caution should be used when such agents are administered concomitantly with HYDEX.
Transient Hypertension: Transient hypertension has been observed primarily during the loading dose in association with the initial peripheral vasoconstrictive effects of dexmedetomidine. Treatment of the transient hypertension has generally not been necessary, although reduction of the loading infusion rate may be desirable.
Arousability: Some patients receiving dexmedetomidine have been observed to be arousable and alert when stimulated. This alone should not be considered as evidence of lack of efficacy in the absence of other clinical signs and symptoms.
Withdrawal: Intensive Care Unit Sedation: The most common withdrawal events after prolonged administration (several days) are nausea, vomiting, and agitation. In adult subjects, tachycardia and hypertension requiring intervention in the 48 hours following study drug discontinuation occurred at frequencies of <5%. If tachycardia and/or hypertension occurs after discontinuation of HYDEX, supportive therapy is indicated.
Procedural Sedation: In adult subjects, withdrawal symptoms were not seen after discontinuation of short term infusions of dexmedetomidine (<6 hours).
Tolerance and Tachyphylaxis: Prolonged exposure to dexmedetomidine beyond 24 hours may be associated with tolerance and tachyphylaxis and a dose-related increase in adverse events.
Effects on Ability to Drive and Use Machines: Not relevant.
Pregnancy: There are no or limited amount of data from the use of dexmedetomidine in pregnant women. Studies in animals have shown reproductive toxicity. HYDEX is not recommended during pregnancy and in women of childbearing potential not using contraception.
Lactation: Available data in the rat have shown excretion of dexmedetomidine or metabolites in milk. A risk to infants cannot be excluded. A decision must be made whether to discontinue breastfeeding or to discontinue dexmedetomidine therapy taking into account the benefit of breastfeeding for the child and the benefit of therapy for the woman.
Summary of the safety profile: The most frequently reported adverse reactions with dexmedetomidine are hypotension, hypertension and bradycardia, occurring in approximately 25%, 15% and 13% of patients respectively.
Hypotension and bradycardia were also the most frequent dexmedetomidine-related serious adverse reactions occurring in 1.7% and 0.9% of randomised Intensive Care Unit (ICU) patients respectively.
Tabulated list of adverse reactions: The adverse reactions listed in Table 2 have been accumulated from pooled data of clinical trials in intensive care.
Adverse reactions are ranked under headings of frequency, the most frequent first, using the following convention: Very common (≥1/10); common (≥1/100 to <1/10); uncommon (≥1/1,000 to <1/100); rare (≥1/10,000 to <1/1,000); very rare (<1/10,000). (See Table 2.)
Click on icon to see table/diagram/image
Interaction studies have only been performed in adults.
Co-administration of dexmedetomidine with anaesthetics, sedatives, hypnotics, and opioids is likely to lead to an enhancement of effects, including sedative, anaesthetic and cardiorespiratory effects. Specific studies have confirmed enhanced effects with isoflurane, propofol, alfentanil, and midazolam.
No pharmacokinetic interactions between dexmedetomidine and isoflurane, propofol, alfentanil and midazolam have been demonstrated. However, due to possible pharmacodynamic interactions, when co-administered with dexmedetomidine, a reduction in dosage of dexmedetomidine or the concomitant anaesthetic, sedative, hypnotic or opioid may be required.
Inhibition of CYP enzymes including CYP2B6 by dexmedetomidine has been studied in human liver microsome incubations. In vitro study suggests that interaction potential in vivo exists between dexmedetomidine and substrates with dominant CYP2B6 metabolism.
Induction of dexmedetomidine in vitro was observed on CYP1A2, CYP2B6, CYP2C8, CYP2C9 and CYP3A4, and induction in vivo cannot be excluded. The clinical significance is unknown.
The possibility of enhanced hypotensive and bradycardic effects should be considered in patients receiving other medicinal products causing these effects, for example beta blockers, although additional effects in an interaction study with esmolol were modest.
Incompatibilities: HYDEX infusion should not be co-administered through the same intravenous catheter with blood or plasma because physical compatibility has not been established.
HYDEX has been shown to be incompatible when administered with the following drugs: amphotericin B, diazepam.
HYDEX has been shown to be compatible when administered with the following intravenous fluids: 0.9% sodium chloride in water, 5% dextrose in water, 20% mannitol, Lactated Ringer's solution, 100 mg/mL magnesium sulfate solution, 0.3% potassium chloride solution.
Compatibility with Natural Rubber: Compatibility studies have demonstrated the potential for absorption of HYDEX to some types of natural rubber. Although HYDEX is dosed to effect, it is advisable to use administration components made with synthetic or coated natural rubber gaskets.
Unopened vials: Do not store above 30°C.
Diluted preparation: For storage conditions after dilution of the medicinal product, see Shelf-Life as follows.
Shelf-Life: Unopened vial: 3 years.
After dilution: Chemical and physical in-use stability has been demonstrated for 24 hours at 15-30°C.
From a microbiological point of view, the product should be used immediately.
N05CM18 - dexmedetomidine ; Belongs to the class of other hypnotics and sedatives.
Hydex infusion 100 mcg/mL
2 mL x 1's


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image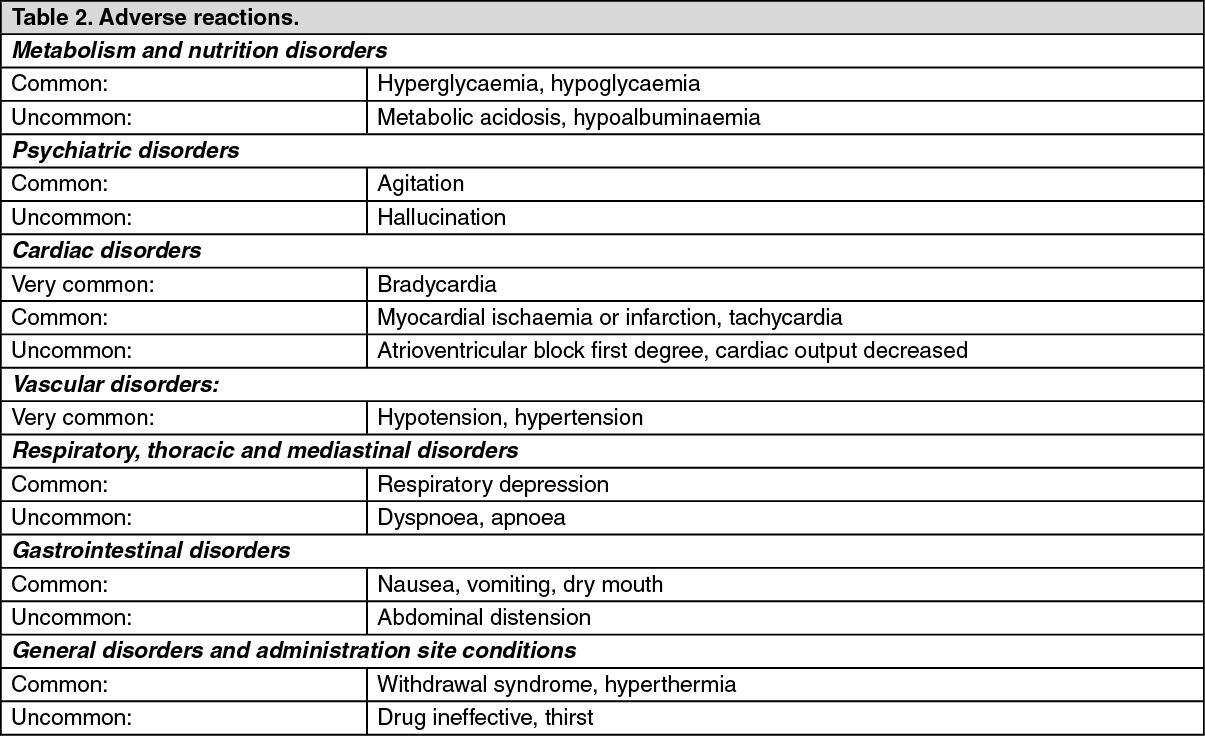 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out
