Pharmacotherapeutic group: Platelet aggregation inhibitors excluding heparin.
ATC code: B01AC22.
Pharmacology: Pharmacodynamics: Mechanism of action/Pharmacodynamic effects: Prasugrel is an inhibitor of platelet activation and aggregation through the irreversible binding of its active metabolite to the P2Y
12 class of ADP receptors on platelets. Since platelets participate in the initiation and/or evolution of thrombotic complications of atherosclerotic disease, inhibition of platelet function can result in the reduction of the rate of cardiovascular events eg, death, myocardial infarction, or stroke.
Following a 60 mg loading dose of prasugrel, inhibition of ADP-induced platelet aggregation occurs at 15 minutes with 5 μM ADP and 30 minutes with 20 μM ADP. The maximum inhibition by prasugrel of ADP-induced platelet aggregation is 83% with 5 μM ADP and 79% with 20 μM ADP, in both cases with 89% of healthy subjects and patients with stable atherosclerosis achieving at least 50% inhibition of platelet aggregation by 1 hour. Prasugrel-mediated inhibition of platelet aggregation exhibits low between-subject (9%) and within-subject (12%) variability with both 5 μM and 20 μM ADP. Mean steady-state inhibition of platelet aggregation was 74% and 69% respectively for 5 μM ADP and 20 μM ADP, and was achieved following 3 to 5 days of administration of the 10 mg prasugrel maintenance dose preceded by a 60 mg loading dose. More than 98% of subjects had ≥20% inhibition of platelet aggregation during maintenance dosing.
Platelet aggregation gradually returned to baseline values after treatment in 7 to 9 days after administration of a single 60 mg loading dose of prasugrel and in 5 days following discontinuation of maintenance dosing at steady-state.
Switching data: Following administration of 75 mg clopidogrel once daily for 10 days, 40 healthy subjects were switched to prasugrel 10 mg once daily with or without a loading dose of 60 mg. Similar or higher inhibition of platelet aggregation was observed with prasugrel. Switching directly to prasugrel 60 mg loading dose resulted in the most rapid onset of higher platelet inhibition. Following administration of a 900-mg loading dose of clopidogrel (with ASA), 56 subjects with ACS were treated for 14 days with either prasugrel 10 mg once daily or clopidogrel 150 mg once daily, and then switched to either clopidogrel 150 mg or prasugrel 10 mg for another 14 days. Higher inhibition of platelet aggregation was observed in patients switched to prasugrel 10 mg compared with those treated with clopidogrel 150 mg. In a study of 276 ACS patients managed with PCI, switching from an initial loading dose of 600 mg clopidogrel or placebo administered upon presentation to the hospital prior to coronary angiography to a 60 mg loading dose of prasugrel administered at the time of percutaneous coronary intervention, resulted in a similar increased inhibition of platelet aggregation for the 72 hour duration of the study. Although this trial was too small to evaluate bleeding definitively, there was no signal suggesting increased bleeding when prasugrel 60 mg was added to clopidogrel 600 mg compared with that of prasugrel 60 mg alone.
Clinical efficacy and safety: Acute Coronary Syndrome (ACS): The phase 3 TRITON study compared Effient with clopidogrel, both co-administered with ASA and other standard therapy. TRITON was a 13,608 patient, multicenter international, randomised, double-blind, parallel group study. Patients had ACS with moderate to high risk UA, NSTEMI, or STEMI and were managed with PCI.
Patients with UA/NSTEMI within 72 hours of symptoms or STEMI between 12 hours to 14 days of symptoms were randomised after knowledge of coronary anatomy. Patients with STEMI within 12 hours of symptoms and planned for primary PCI could be randomised without knowledge of coronary anatomy. For all patients, the loading dose could be administered anytime between randomisation and 1 hour after the patient left the catheterisation lab.
Patients randomised to receive prasugrel (60 mg loading dose followed by 10 mg once daily) or clopidogrel (300 mg loading dose followed by 75 mg once daily) were treated for a median of 14.5 months (maximum of 15 months with a minimum of 6 months follow-up). Patients also received ASA (75 mg to 325 mg once daily). Use of any thienopyridine within 5 days before enrolment was an exclusion criterion. Other therapies, such as heparin and GPIIb/IIIa inhibitors, were administered at the discretion of the physician. Approximately 40% of patients (in each of the treatment groups) received GPIIb/IIIa inhibitors in support of PCI (no information available regarding the type of GP IIb/IIIa inhibitor used). Approximately 98% of patients (in each of the treatment groups) received antithrombins (heparin, low molecular weight heparin, bivalirudin, or other agent) directly in support of PCI.
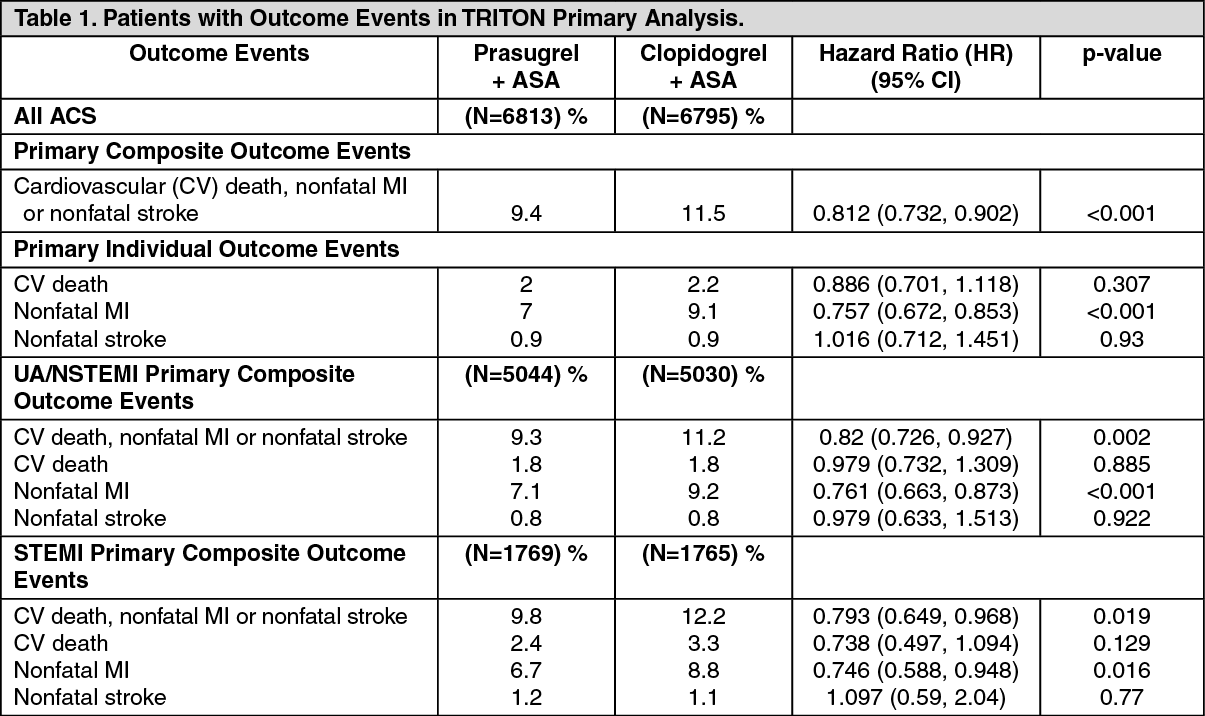
The trial's primary outcome measure was the time to first occurrence of cardiovascular (CV) death, non-fatal myocardial infarction (MI), or non-fatal stroke. Analysis of the composite endpoint in the All ACS population (combined UA/NSTEMI and STEMI cohorts) was contingent on showing statistical superiority of prasugrel versus clopidogrel in the UA/NSTEMI cohort (p<0.05).
All ACS Population: Effient showed superior efficacy compared to clopidogrel in reducing the primary composite outcome events, as well as the prespecified secondary outcome events, including stent thrombosis (see Table 1). The benefit of prasugrel was apparent within the first 3 days and it persisted to the end of study. The superior efficacy was accompanied by an increase in major bleeding (see Precautions and Adverse Reactions). The patient population was 92% Caucasian, 26% female, and 39% ≥65 years of age. The benefits associated with prasugrel were independent of the use of other acute and long-term cardiovascular therapies, including heparin/low molecular weight heparin, bivalirudin, intravenous GPIIb/IIIa inhibitors, lipid-lowering medicinal products, beta-blockers, and angiotensin converting enzyme inhibitors. The efficacy of prasugrel was independent of the ASA dose (75 mg to 325 mg once daily). The use of oral anticoagulants, non-study antiplatelet medicinal products and chronic NSAIDs was not allowed in TRITON. In the All ACS population, prasugrel was associated with a lower incidence of CV death, non-fatal MI, or non-fatal stroke compared to clopidogrel, regardless of baseline characteristics such as age, sex, body weight, geographical region, use of GPIIb/IIIa inhibitors, and stent type. The benefit was primarily due to a significant decrease in non-fatal MI (see Table 1). Subjects with diabetes had significant reductions in the primary and all secondary composite endpoints.
The observed benefit of prasugrel in patients ≥75 years was less than that observed in patients <75 years. Patients ≥75 years were at increased risk of bleeding, including fatal (see Dosage & Administration, Precautions and Adverse Reactions). Patients ≥75 years in whom the benefit with prasugrel was more evident included those with diabetes, STEMI, higher risk of stent thrombosis, or recurrent events.
Patients with a history of TIA or a history of ischaemic stroke more than 3 months prior to prasugrel therapy had no reduction in the primary composite endpoint. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
In the All ACS population, analysis of each of the secondary endpoints showed a significant benefit (p<0.001) for prasugrel versus clopidogrel. These included definite or probable stent thrombosis at study end (0.9% vs 1.8%; HR 0.498; CI 0.364, 0.683); CV death, nonfatal MI, or urgent target vessel revascularization through 30 days (5.9% vs 7.4%; HR 0.784; CI 0.688, 0.894); all cause death, nonfatal MI, or nonfatal stroke through study end (10.2% vs 12.1%; HR 0.831; CI 0.751, 0.919); CV death, nonfatal MI, nonfatal stroke or rehospitalisation for cardiac ischaemic event through study end (11.7% vs 13.8%; HR 0.838; CI 0.762, 0.921). Analysis of all cause death did not show any significant difference between prasugrel and clopidogrel in the All ACS population (2.76% vs 2.90%), in the UA/NSTEMI population (2.58% vs 2.41%), and in the STEMI population (3.28% vs 4.31%).
Prasugrel was associated with a 50% reduction in stent thrombosis through the 15 month follow-up period. The reduction in stent thrombosis with Effient was observed both early and beyond 30 days for both bare metal and drug eluting stents.
In an analysis of patients who survived an ischaemic event, prasugrel was associated with a reduction in the incidence of subsequent primary endpoint events (7.8% for prasugrel vs 11.9% for clopidogrel).
Although bleeding was increased with prasugrel, an analysis of the composite endpoint of death from any cause, nonfatal myocardial infarction, nonfatal stroke, and non-CABG-related TIMI major haemorrhage favoured Effient compared to clopidogrel (Hazard ratio, 0.87; 95% CI, 0.79 to 0.95; p=0.004). In TRITON, for every 1000 patients treated with Effient, there were 22 fewer patients with myocardial infarction, and 5 more with non–CABG-related TIMI major haemorrhages, compared with patients treated with clopidogrel.
In TRITON-TIMI 38, prasugrel reduced ischemic events (mainly nonfatal MIs) and increased bleeding events [see Adverse Reactions] relative to clopidogrel. The findings are consistent with the intended greater inhibition of platelet aggregation by prasugrel at the doses used in the study. There is, however, an alternative explanation: both prasugrel and clopidogrel are pro-drugs that must be metabolized to their active moieties. Whereas the pharmacokinetics of prasugrel's active metabolite are not known to be affected by genetic variations in CYP2B6, CYP2C9, CYP2C19, or CYP3A5, the pharmacokinetics of clopidogrel's active metabolite are affected by CYP2C19 genotype, and approximately 30% of Caucasians are reduced-metabolizers. Moreover, certain proton pump inhibitors, widely used in the ACS patient population and used in TRITON-TIMI 38, inhibit CYP2C19, thereby decreasing formation of clopidogrel's active metabolite. Thus, reduced metabolizer status and use of proton pump inhibitors may diminish clopidogrel's activity in a fraction of the population, and may have contributed to prasugrel's greater treatment effect and greater bleeding rate in TRITON-TIMI 38. The extent to which these factors were operational, however, is unknown.
Results of a pharmacodynamic/pharmacogenomic study in 720 Asian ACS PCI patients demonstrated that higher levels of platelet inhibition are achieved with prasugrel compared to clopidogrel, and that prasugrel 60-mg loading dose/10-mg maintenance dose is an appropriate dose regimen in Asian subjects who weigh at least 60 kg and are less than 75 years of age (see Dosage & Administration).
In a 30 month study (TRILOGY–ACS) in 9326 patients with UA/NSTEMI ACS medically managed without revascularisation (non-licensed indication), prasugrel did not significantly reduce the frequency of the composite endpoint of CV death, MI or stroke compared to clopidogrel. Rates of TIMI major bleeding (including life threatening, fatal and ICH) were similar in prasugrel and clopidogrel treated patients. Patients ≥75 years old or those below 60 kg (N=3022) were randomized to 5 mg prasugrel. As in the < 75 years old and ≥60 kg patients treated with 10 mg prasugrel, there was no difference between 5 mg prasugrel and 75 mg clopidogrel in CV outcomes. Rates of major bleeding were similar in patients treated with 5 mg prasugrel and those treated with 75 mg clopidogrel. Prasugrel 5 mg provided greater antiplatelet effect than clopidogrel 75 mg. Prasugrel should be used with caution in patients ≥ 75 years old and in patients weighing <60 kg (see Dosage & Administration, Precautions and Adverse Reactions).
In a 30-day study (ACCOAST) in 4033 patients with NSTEMI with elevated troponin who were scheduled for coronary angiography followed by PCI within 2 to 48 hours after randomization, subjects who received prasugrel 30 mg loading dose on average 4 hours prior to coronary angiography followed by a 30 mg loading dose at the time of PCI (n=2037) had an increased risk of non-CABG peri-procedural bleeding and no additional benefit compared to patients receiving a 60 mg loading dose at the time of PCI (n=1996). Specifically, prasugrel did not significantly reduce the frequency of the composite endpoint of cardiovascular (CV) death, myocardial infarction (MI), stroke, urgent revascularization (UR), or glycoprotein (GP) IIb/IIIa inhibitor bailout through 7 days from randomization in subjects receiving prasugrel prior to coronary angiography compared to patients receiving the full loading dose of prasugrel at the time of PCI, and the rate of the key safety objective for all TIMI major bleeding (CABG and non-CABG events) through 7 days from randomization in all treated subjects was significantly higher in subjects receiving prasugrel prior to coronary angiography versus patients receiving the full loading dose of prasugrel at the time of PCI. Therefore, in UA/NSTEMI patients, where coronary angiography is performed within 48 hours after admission, the loading dose should be given at the time of PCI. (See Dosage & Administration, Precautions and Adverse Reactions.)
Paediatric population: Study TADO tested the use of prasugrel (n=171) vs placebo (n=170) in patients, ages 2 to less than 18 years of age, with sickle cell anaemia for reduction of vaso occlusive crisis in a phase III study. The study failed to meet any of the primary or secondary endpoints. Overall, no new safety findings were identified for prasugrel as monotherapy in this patient population.
Pharmacokinetics: Prasugrel is a prodrug and is rapidly metabolised
in vivo to an active and inactive metabolites. The active metabolite's exposure AUC has moderate to low between-subject (27%) and within-subject (19%) variability. Prasugrel's pharmacokinetics are similar in healthy subjects, patients with stable atherosclerosis, and patients undergoing percutaneous coronary intervention.
Absorption: The absorption and metabolism of prasugrel are rapid, with peak plasma concentration (C
max) of the active metabolite occurring in approximately 30 minutes. The active metabolite's exposure (AUC) increases proportionally over the therapeutic dose range. In a study of healthy subjects, AUC of the active metabolite was unaffected by a high fat, high calorie meal, but C
max was decreased by 49% and the time to reach C
max (T
max) was increased from 0.5 to 1.5 hours. Effient was administered without regard to food in TRITON. Therefore, Effient can be administered without regard to food; however, the administration of prasugrel loading dose in the fasted state may provide most rapid onset of action (see Dosage & Administration).
Distribution: Active metabolite binding to human serum albumin (4% buffered solution) was 98%.
Biotransformation: Prasugrel is not detected in plasma following oral administration. It is rapidly hydrolysed in the intestine to a thiolactone, which is then converted to the active metabolite by a single step of cytochrome P450 metabolism, primarily by CYP3A4 and CYP2B6 and to a lesser extent by CYP2C9 and CYP2C19. The active metabolite is further metabolised to two inactive compounds by S-methylation or conjugation with cysteine.
In healthy subjects, patients with stable atherosclerosis, and patients with ACS receiving Effient, there was no relevant effect of genetic variation in CYP3A5, CYP2B6, CYP2C9 or CYP2C19 on the pharmacokinetics of prasugrel or its inhibition of platelet aggregation.
Elimination: Approximately 68% of the prasugrel dose is excreted in the urine and 27% in the feces, as inactive metabolites. The active metabolite has an elimination half-life of about 7.4 hours (range 2 to 15 hrs).
Pharmacokinetics in special populations: Elderly: In a study of healthy subjects between the ages of 20 and 80 years, age had no significant effect on pharmacokinetics of prasugrel or its inhibition of platelet aggregation. In the large phase 3 clinical trial, the mean estimated exposure (AUC) of the active metabolite was 19% higher in very elderly patients (≥75 years) compared to subjects <75 years of age. Prasugrel should be used with caution in patients ≥75 years due to the potential risk of bleeding in this population (see Dosage & Administration and Precautions). In a study in subjects with stable atherosclerosis, the mean AUC of the active metabolite in patients ≥75 years old taking 5 mg prasugrel was approximately half that in patients < 65 years old taking 10 mg prasugrel, and the antiplatelet effect of 5 mg was reduced but was non-inferior compared to 10 mg.
Hepatic Impairment: No dose adjustment is necessary for patients with mild to moderate impaired hepatic function (Child-Pugh Class A and B). Pharmacokinetics of prasugrel and its inhibition of platelet aggregation were similar in subjects with mild to moderate hepatic impairment compared to healthy subjects. Pharmacokinetics and pharmacodynamics of prasugrel in patients with severe hepatic impairment have not been studied. Prasugrel must not be used in patients with severe hepatic impairment (see Contraindications).
Renal Impairment: No dosage adjustment is necessary for patients with renal impairment, including patients with end-stage renal disease (ESRD). Pharmacokinetics of prasugrel and its inhibition of platelet aggregation are similar in patients with moderate renal impairment (GFR 30-<50 ml/min/1.73 m
2) and healthy subjects. Prasugrel-mediated inhibition of platelet aggregation was also similar in patients with ESRD who required haemodialysis compared to healthy subjects, although C
max and AUC of the active metabolite decreased 51% and 42%, respectively, in ESRD patients.
Body Weight: The mean exposure (AUC) of the active metabolite of prasugrel is approximately 30 to 40% higher in healthy subjects and patients with a body weight of <60 kg compared to those weighing ≥60 kg. Prasugrel should be used with caution in patients with a body weight of <60 kg due to the potential risk of bleeding in this population (see Precautions). In a study in subjects with stable atherosclerosis, the mean AUC of the active metabolite in patients <60 kg taking 5 mg prasugrel was 38% lower than in patients ≥60 kg taking 10 mg prasugrel, and the antiplatelet effect of 5 mg was similar to 10 mg.
Ethnicity: In clinical pharmacology studies, after adjusting for body weight, the AUC of the active metabolite was approximately 19% higher in Chinese, Japanese, and Korean subjects compared to that of Caucasians, predominantly related to higher exposure in Asian subjects <60 kg. There is no difference in exposure among Chinese, Japanese and Korean subjects. Exposure in subjects of African and Hispanic descent is comparable to that of Caucasians. No dose adjustment is recommended based on ethnicity alone.
Gender: In healthy subjects and patients, the pharmacokinetics of prasugrel are similar in men and women.
Paediatric population:
Pharmacokinetics and pharmacodynamics of prasugrel have not been evaluated in a pediatric population (see Dosage & Administration).
Toxicology: Preclinical safety data: Non-clinical data reveal no special hazard for humans based on conventional studies of safety pharmacology, repeat-dose toxicity, genotoxicity, carcinogenic potential, or toxicity to reproduction. Effects in nonclinical studies were observed only at exposures considered sufficiently in excess of the maximum human exposure indicating little relevance to clinical use.
Embryo-foetal developmental toxicology studies in rats and rabbits showed no evidence of malformations due to prasugrel. At a very high dose (>240 times the recommended daily human maintenance dose on a mg/m
2 basis) that caused effects on maternal body weight and/or food consumption, there was a slight decrease in offspring body weight (relative to controls). In pre- and post-natal rat studies, maternal treatment had no effect on the behavioural or reproductive development of the offspring at doses up to an exposure 240 times the recommended daily human maintenance dose (based on mg/m
2).
No compound-related tumours were observed in a 2-year rat study with prasugrel exposures ranging to greater than 75 times the recommended therapeutic exposures in humans (based on plasma exposures to the active and major circulating human metabolites). There was an increased incidence of tumours (hepatocellular adenomas) in mice exposed for 2 years to high doses (>75 times human exposure), but this was considered secondary to prasugrel-induced enzyme-induction. The rodent-specific association of liver tumours and drug-induced enzyme induction is well documented in the literature. The increase in liver tumours with prasugrel administration in mice is not considered a relevant human risk.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image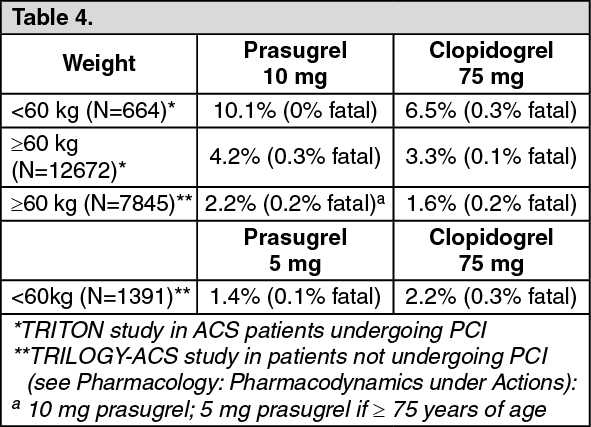 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image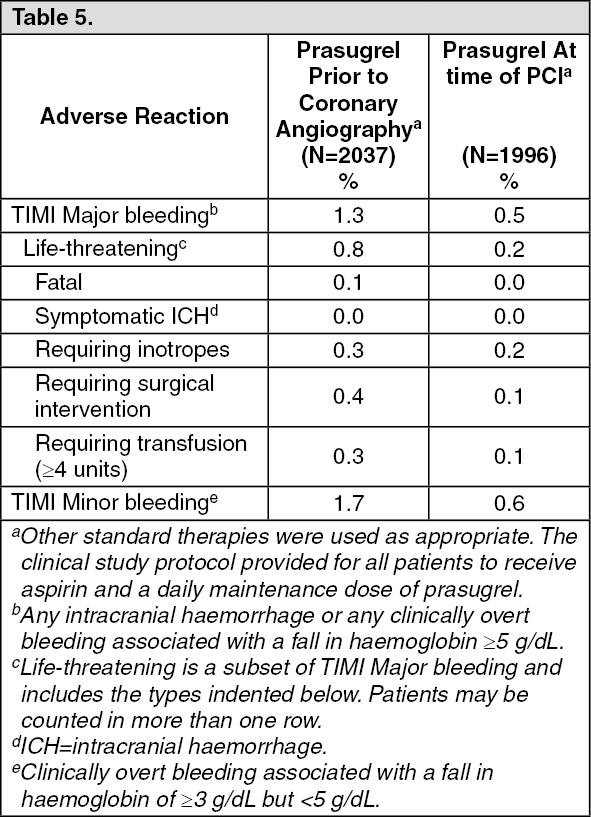 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image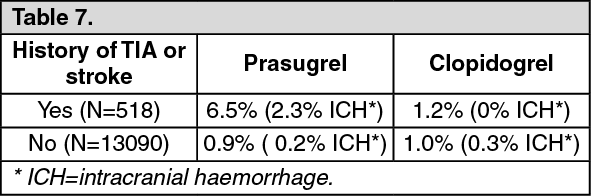 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image


 Sign Out
Sign Out
