


 Sign Out
Sign Out

Bleeding: Non-Coronary Artery Bypass Graft (CABG) related bleeding: In TRITON, the frequency of patients experiencing a non-CABG related bleeding event is shown in Table 2. The incidence of Non-CABG-related TIMI major bleeding, including life-threatening and fatal, as well as TIMI minor bleeding, was statistically significantly higher in subjects treated with prasugrel compared to clopidogrel in the UA/NSTEMI and All ACS populations. No significant difference was seen in the STEMI population. The most common site of spontaneous bleeding was the gastrointestinal tract (1.7% rate with prasugrel and 1.3% rate with clopidogrel); the most frequent site of provoked bleeding was the arterial puncture site (1.3% rate with prasugrel and 1.2% with clopidogrel). (See Table 2.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imagePatients ≥75 years old: Non-CABG-related TIMI major or minor bleeding rates: See Table 3.
 Click on icon to see table/diagram/image
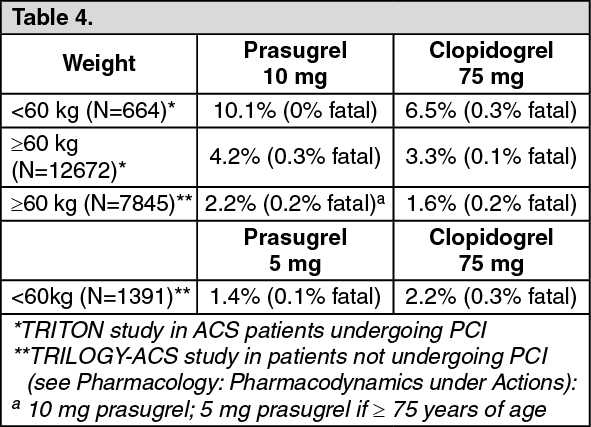
Click on icon to see table/diagram/imagePatients <60 kg: Non-CABG-related TIMI major or minor bleeding rates: See Table 4.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imagePatients ≥60 kg and age <75 years: In patients ≥60 kg and age <75 years, non-CABG-related TIMI major or minor bleeding rates were 3.6% for prasugrel and 2.8% for clopidogrel; rates for fatal bleeding were 0.2% for prasugrel and 0.1% for clopidogrel.
CABG-related bleeding: In the phase 3 clinical trial, 437 patients underwent CABG during the course of the study. Of those patients, the rate of CABG-related TIMI major or minor bleeding was 14.1% for the prasugrel group and 4.5% in the clopidogrel group. The higher risk for bleeding events in subjects treated with prasugrel persisted up to 7 days from the most recent dose of study drug. For patients who received their thienopyridine within 3 days prior to CABG, the frequencies of TIMI major or minor bleeding were 26.7% (12 of 45 patients) in the prasugrel group, compared with 5.0% (3 of 60 patients) in the clopidogrel group. For patients who received their last dose of thienopyridine within 4 to 7 days prior to CABG, the frequencies decreased to 11.3% (9 of 80 patients) in the prasugrel group and 3.4% (3 of 89 patients) in the prasugrel group. Beyond 7 days after drug discontinuation, the observed rates of CABG-related bleeding were similar between treatment groups (see Precautions).
Bleeding Risk Associated with Timing of Loading Dose in NSTEMI: In a clinical study of NSTEMI patients (the ACCOAST study), where patients were scheduled to undergo coronary angiography within 2 to 48 hours after randomization, patients given a 30 mg loading dose on average 4 hours prior to coronary angiography followed by a 30 mg loading dose at the time of PCI had an increased risk of non-CABG peri-procedural bleeding and no additional benefit compared to patients receiving a 60 mg loading dose at the time of PCI (see Dosage & Administration and Precautions).
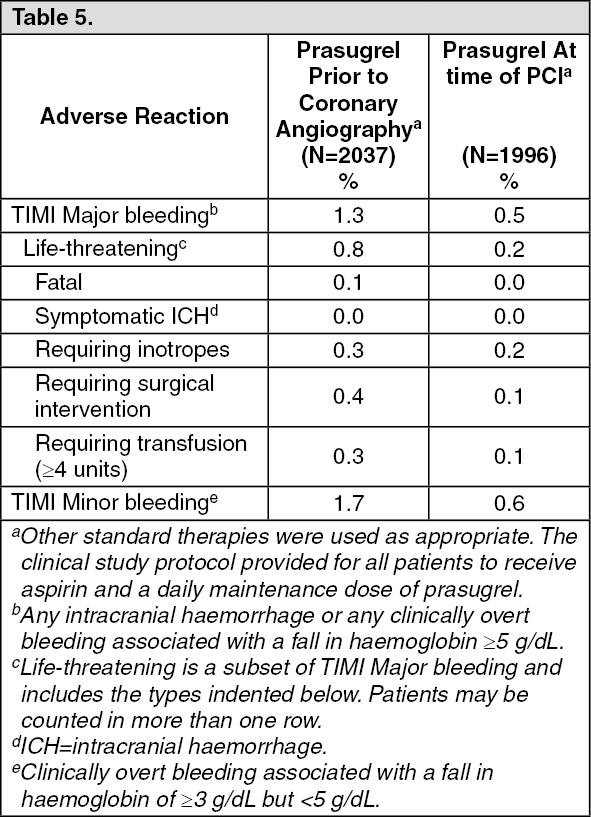
Non-CABG- related TIMI bleeding rates through 7 days for patients were as follows: See Table 5.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageTabulated summary of adverse reactions: Table 6 summarizes haemorrhagic and non-haemorrhagic adverse reactions in TRITON, or that were spontaneously reported classified by frequency and system organ class. Frequencies are defined as follows: Very common (≥1/10); common (≥1/100 to <1/10); uncommon (≥1/1000 to <1/100); rare (≥1/10,000 to <1/1000); very rare (<1/10,000); not known (cannot be estimated from the available data). (See Table 6.)
 Click on icon to see table/diagram/image
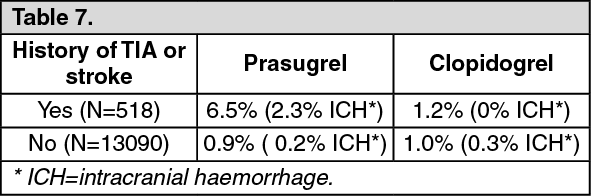
Click on icon to see table/diagram/imageIn patients with or without a history of TIA or stroke, the incidence of stroke in the phase 3 clinical trial was as follows (see Precautions): See Table 7.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
View ADR Monitoring Form