Aceclofenac sustained-release, rabeprazole sodium enteric coated.
Each capsule contains aceclofenac 200 mg as a sustained release pellets, rabeprazole sodium 20 mg as enteric coated pellets. It also contains the following excipients: Nonpareil seeds, purified talc, sodium hydroxide, hypromellose, light magnesium carbonate, methacrylic acid copolymer dispersion, glyceryl monostearate, polysorbate 80, titanium dioxide, ferric oxide (red), povidone, ethyl cellulose, triacetin.
Aceclofenac is a [[[2-[(2,6-Dichlorophenyl)amino]phenyl]acetyl]oxy] acetic acid. Its empirical formula is C16H13Cl2NO17 with a molecular weight of 354.2.
Rabeprazole is a (RS)-2-([4-(3-methoxypropoxy)-3-methylpyridin-2-yl]methylsulfinyl)-1H-benzo[d]imidazole. Its empirical formula is C18H21N3O3S, with a molecular weight of 359.444.
Pharmacology: Pharmacodynamics: Aceclofenac: Aceclofenac is a nonsteroidal agent with marked anti-inflammatory and analgesic properties. The mode of action of aceclofenac is largely based on the inhibition of prostaglandin synthesis. Aceclofenac is a potent inhibition of the enzyme cyclooxygenase, which is involved in the production of prostaglandins.
Rabeprazole: Rabeprazole sodium belongs to the class of antisecretory compounds, the substituted benzimidazoles, that do not exhibit anticholinergic or H2-histamine antagonist properties, but suppress gastric acid secretion by the specific inhibition of the H+/K+-ATPase enzyme (the acid or proton pump). The effect is dose-related and leads to inhibition of both basal and stimulated acid secretion, irrespective of the stimulus. Animal studies indicate that after administration, rabeprazole sodium rapidly disappears from both the plasma and gastric mucosa. As a weak base, rabeprazole is rapidly absorbed following all doses and is concentrated in the acid environment of the parietal cells. Rabeprazole is converted to the active sulphenamide form through protonation and it subsequently reacts with the available cysteines on the proton pump.
After oral administration of rabeprazole sodium 20 mg, the onset of the antisecretory effect occurs within 1 hr, with the maximum effect occurring within 2-4 hrs. Inhibition of basal and food stimulated acid secretion 23 hrs after the first dose of rabeprazole sodium are 69% and 82%, respectively, and the duration of inhibition lasts up to 48 hrs. The inhibition effect of rabeprazole sodium on acid secretion increases slightly with repeated once-daily dosing, achieving steady state inhibition after 3 days. When the drug is discontinued, secretory activity normalizes over 2-3 days.
Pharmacokinetics: Aceclofenac: After oral administration, aceclofenac is rapidly and completely absorbed as unchanged drug. Peak plasma concentrations are reached approximately 1.25-3 hrs following ingestion. Aceclofenac penetrates into the synovial fluid, where the concentrations reach approximately 57% of those in plasma. The volume of distribution is approximately 25 L. The mean plasma elimination half-life (t½) is around 4 hrs. Aceclofenac is highly protein-bound (>99%). Aceclofenac circulates mainly as unchanged drug. 4'-Hydroxyaceclofenac dose is excreted via urine, mainly as hydroxymetabolites. No changes in the pharmacokinetics of aceclofenac have been detected in the elderly.
Rabeprazole: Rabeprazole is an enteric-coated (gastro-resistant) formulation of rabeprazole sodium. This presentation is necessary because rabeprazole is acid-labile. Absorption of rabeprazole therefore begins only after it leaves the stomach. Absorption is rapid, with peak plasma levels of rabeprazole occurring approximately 3.5 hrs after a 20 mg dose. Peak plasma concentrations (Cmax) of rabeprazole and AUC are linear over the dose range of 10-40 mg. Absolute bioavailability of an oral 20-mg dose (compared to IV administration) is about 52% due in large part to presystem metabolism. Additionally, the bioavailability does not appear to increase with repeat administration. In healthy subjects, the plasma t½ is approximately 1 hr (range 0.7-1.5 hrs), and the total body clearance is estimated to be 283±98 mL/min. There was no clinically relevant interaction with food. Neither food nor the time of the day of administration of the treatment affect the absorption of rabeprazole sodium.
Rabeprazole is approximately 97% bound to human plasma proteins.
Rabeprazole sodium, as is the case with other members of the proton-pump inhibitor (PPI) class of compounds, is metabolized though the cytochrome P450 (CVP45q) hepatic drug metabolising system. In vitro studies with human liver microsomes indicated that rabeprazole sodium is metabolised by isoenzymes of CYP450 (CYP2C19 and CYP3A4). In these studies, at expected human plasma concentrations, rabeprazole neither induces nor inhibits CYP3A4; and although in vitro studies may not always be predictive of in vivo status these findings indicate that no interaction is expected between rabeprazole and cyclosporin. In humans, the thioether (M1) and carboxylic acid (M6) are the main plasma metabolites with the sulphone (M2), desmethyl-thioether (M4) and mercapturic acid conjugates (M5) minor metabolites observed at lower levels. Only the desmethyl metabolite (M3) has a small amount of antisecretory activity, butitis not present in plasma.
Following a single 20 mg 14C labelled oral dose of rabeprazole sodium, no unchanged drugs was excreted in the urine. Approximately, 90% of the dose was eliminated in urine mainly as the 2 metabolites: A mercapturic acid conjugate (M5) and a carboxylic acid (M6), plus 2 unknown metabolites. The remainder of the dose was recovered in faeces.
Special Populations: Geriatrics: Aceclofenac: Maximum plasma concentrations (Cmax) of aceclofenac and times to Cmax (Tmax) are similar after single (100 mg) and multiple (100 mg twice daily for 7 days). Oral doses: In a study in 12 elderly volunteers, mean Cmax values ranged from 8.94-9.86 mg/mL and were achieved in 1.08-1.37 hrs. Areas under plasma drug concentration versus time curves (AUCs) were increased over those seen after single doses in young individuals and decreased in the elderly after multiple doses. No significant differences were observed between young and elderly volunteers in Cmax absorption t½ or V4 values.
Rabeprazole: Elimination of rabeprazole was somewhat decreased in the elderly. Following 7 days of daily dosing with rabeprazole sodium 20 mg, the AUC approximately doubled, the Cmax increased by 60% and t½ increased by approximately 30% as compared to young healthy volunteers. However, there was no evidence of rabeprazole accumulation.
Gender: Rabeprazole: Adjusted for body mass and height, there are no significant gender differences in pharmacokinetic parameters following a single dose of rabeprazole 20 mg.
Renal Dysfunction: Rabeprazole: In as reported study, patients with stable, end-stage, renal failure requiring maintenance haemodialysis [creatinine clearance (CrCl) 5 mL/min/1.73m2], the disposition of rabeprazole was very similar to that in healthy volunteers. The AUC and the Cmax in these patients was about 35% lower than the corresponding parameters in healthy volunteers. The mean t½ of rabeprazole was 0.82 hrs in healthy volunteers, 0.95 hrs in patients during haemodialysis and 3.6 hrs post-dialysis. The clearance of the drug in patients was approximately twice that in healthy volunteers.
Hepatic Dysfunction: Rabeprazole: Following a single dose of rabeprazole 20 mg to patients with chronic mild to moderate hepatic impairment the AUC doubled and there was a 2- to 3-fold increase in t½ of rabeprazole compared to the healthy volunteers. However, following a 20-mg dose daily for 7 days the AUC had increased to only 1.5-fold and the Cmax to only 1.2-fold. The t½ of rabeprazole in patients with hepatic impairment was 12.3 hrs compared to 2.1 hrs in healthy volunteers. The pharmacodynamic response (gastric pH control) in the 2 groups was clinically comparable.
Rabeprazole: Following a dose of rabeprazole 20 mg for 7 days, CYP2C19 slow metabolizes, had AUC and t½ which were approximately 1.9 and 1.6 times the corresponding parameters in extensive metabolizes whilst Cmax had increased only 40%.
Relief of pain and inflammation in osteoarthritis, rheumatoid arthritis and ankylosing spondylitis.
Adults: Recommended Dose: 1 cap once daily, preferably at bedtime or as directed by the physician.
Carefully consider the potential benefits and risks of Naclo-R capsules and other treatment options before deciding to use Naclo-R capsules.
Administration: The route of administration is oral.
Naclo-R capsules are supplied for oral administration and should be swallowed whole with a sufficient quantity of liquid. Naclo-R capsules should be taken with or after food.
Aceclofenac: Management of acute poisoning with nonsteroidal anti-inflammatory drugs (NSAIDs) essentially consists of supportive and symptomatic measures. There is no human data available on the consequences of aceclofenac overdosage. The therapeutic measures to be taken are: Absorption should be prevented as soon as possible after overdosage by means of gastric lavage and treatment with activated charcoal; supportive and symptomatic treatment should be given for complications eg, hypotension, renal failure, convulsions, gastrointestinal irritation, an respiratory depression; specific therapies eg, forced diuresis, dialysis or haemoperfusion are probably of no help in eliminating NSAIDs due to their high rate of protein binding and extensive metabolism.
Rabeprazole: Experience to date with deliberate or accidental overdose is limited. The maximum established exposure has not exceeded 60 mg twice daily or 160 mg once daily. Effects are generally minimal, representative of the known adverse event profile and reversible without further medical intervention. No specific antidote is known. Rabeprazole sodium is extensively protein-bound and is therefore, not dialysable. As in any case of overdose, treatment should be symptomatic and general supportive measures should be utilized.
Hypersensitivity to aceclofenac, rabeprazole, and substituted benzimidazole or to any constituents of Naclo-R; asthma, urticaria, or allergic-type reactions after taking aspirin or other NSAIDs. Severe, rarely fatal, anaphylactic-like reactions to NSAIDs have been reported in such patients (see Warnings and Precautions); history of active or suspected peptic ulcer or gastrointestinal bleeding (see Warnings); moderate to severe renal impairment (see Warnings); treatment of peri-operative pain in the setting of coronary artery bypass graft (CABG) surgery.
Use in pregnancy & lactation: Pregnancy and lactation, unless there are compelling reasons for doing so. The lowest effective dosage of NSAIDs should be used.
Aceclofenac: In late pregnancy, as with other NSAIDs, aceclofenac should be avoided because it may cause premature closure of the ductus arteriosus.
Rabeprazole: Teratology studies have been performed in rats at IV doses up to 50 mg/kg/day (plasma AUC of 11.8 mcg·hr/mL, about 13 times the human exposure at the recommended dose of GERD) and rabbits at IV doses up to 30 mg/kg/day (plasma AUC of 7.3 mcg·hr/mL, about 8 times the human exposure at the recommended dose for GERD) and have revealed no evidence of impaired fertility or harm to the fetus due to rabeprazole. There are, however, no adequate and well-controlled studies in pregnant women. Because animal reproduction studies are not always predictive of human response, Naclo-R should be used during pregnancy only if clearly needed.
Aceclofenac: Cardiovascular Effects: Cardiovascular Thrombotic Events: Clinical trials of several COX-2 selective and nonselective NSAIDs up to 3 years duration have shown an increased risk of serious cardiovascular (CV) thrombotic events, myocardial infarction, and stroke, which can be fatal. All NSAIDs, both COX-2 selective and nonselective, may have a similar risk. Patients with known CV disease or risk factors for CV disease may be at greater risk. To minimize the potential risk for an adverse CV event in patients treated with an NSAID, the lowest effective dose should be used for the shortest duration possible. Physicians and patients should remain alert for the development of such events, even in the absence of previous CV symptoms. Patients should be informed about the signs and/or symptoms of serious CV events and the steps to take if they occur.
There is no consistent evidence that concurrent use of aspirin mitigates the increased risk of serious CV thrombotic events associated with NSAID use. The concurrent use of aspirin and an NSAID does increase the risk of serious gastrointestinal events. (Gastrointestinal Effects-Risk of Ulceration, Bleeding and Perforation as follows).
Hypertension: Nonsteroidal anti-inflammatory drugs including aceclofenac can lead to onset of new hypertension or worsening of preexisting hypertension, either of which may contribute to the incidence of CV events. Patients taking thiazides or loop diuretics may have impaired response to these therapies when taking NSAIDs. Nonsteroidal anti-inflammatory drugs, including aceclofenac, should be used with caution in patients with hypertension. Blood pressure (BP) should be monitored closely during the initiation of NSAID treatment and throughout the course of therapy.
Congestive Heart Failure and Edema: Fluid retention and edema have been observed in some patients taking NSAIDs. Aceclofenac should be used with caution in patients with fluid retention or heart failure.
Gastrointestinal Effects-Risk of Ulceration, Bleeding and Perforation: NSAIDs including aceclofenac can cause serious gastrointestinal adverse events including inflammation, bleeding, ulceration, and perforation of the stomach, small intestine or large intestine, which can be fatal. These serious adverse events can occur at any time, with or without warning symptoms, in patients treated with NSAIDs. Only 1 in 5 patients, who develop a serious upper gastrointestinal adverse event on NSAID therapy, is symptomatic. Upper gastrointestinal ulcers, gross bleeding, or perforation caused by NSAIDs occur in approximately 1% of patients treated for 3-6 months, and in about 2-4% of patients treated for 1 year. These trends continue with longer duration of use, increasing the likelihood of developing a serious gastrointestinal event at some time during the course of therapy. However, even short-term therapy is not without risk.
Nonsteroidal anti-inflammatory drugs should be prescribed with extreme caution in those with a prior history of ulcer disease or gastrointestinal bleeding. Patients with a prior history of peptic ulcer disease and/or gastrointestinal bleeding who use NSAIDs have a greater than 10-fold increased risk for developing a gastrointestinal bleed compared to patients with neither of these risk factors. Other factors that increase the risk for bleeding in patients treated with NSAIDs include concomitant use of oral corticosteroids or anticoagulants, longer duration of NSAID therapy, smoking, use of alcohol, older age, and poor general health status. Most spontaneous reports of fatal gastrointestinal events are in elderly or debilitated patients and therefore, special care should be taken in treating population.
To minimize the potential risk for an adverse gastrointestinal event in patients treated with an NSAID, the lowest effective dose should be used for the shortest possible duration. Patients and physicians should remain alert for signs and symptoms of gastrointestinal ulceration and bleeding during NSAID therapy and promptly initiate additional evaluation and treatment if a serious gastrointestinal adverse event is suspected. This should include discontinuation of the NSAID until a serious gastrointestinal adverse event is ruled out. For high-risk patients, alternate therapies that do not involve NSAIDs should be considered (see Dosage & Administration).
Renal Effects: Long-term administration of NSAIDs has resulted in renal papillary necrosis and other renal injury. Renal toxicity has also seen in patients in whom renal prostaglandins have a compensatory role in the maintenance of renal perfusion. In these patients, administration of NSAIDs may cause a dose-dependent reduction in prostaglandin formation and, secondarily, in renal blood flow, which may precipitate overt renal decompensation. Patients at greatest risk of this reaction are those with impaired renal function, heart failure, liver dysfunction, those taking diuretics and angiotensin-converting enzyme (ACE) inhibitors, and the elderly. Discontinuation of NSAID therapy is usually followed by recovery to the pretreatment state.
Advanced Renal Disease: No information is available from controlled clinical studies regarding the use of aceclofenac in patients with advanced renal disease. Therefore, treatment with aceclofenac is not recommended in these patients with advanced renal disease. If aceclofenac therapy must be initiated, close monitoring of the patient's renal function is advisable.
Hepatic: Close medical surveillance is also imperative in patients suffering from severe impairment of hepatic function.
Anaphylactoid Reactions: As with other NSAIDs, anaphylactoid reactions may occur in patients without known prior exposure to aceclofenac. Aceclofenac should not be given in patients with the aspirin triad. This symptom complex typically occurs in asthmatic patients who experience rhinitis with or without nasal polyps, or who exhibit severe, potentially fatal bronchospasm after taking aspirin or other NSAIDs (see Contraindications and Precautions). Emergency help should be sought in cases where an anaphylactoid reaction occur.
Skin Reactions: Nonsteroidal anti-inflammatory drugs can cause serious skin adverse events eg, exfoliative dermatitis, Stevens-Johnson syndrome (SJS), and toxic epidermal necrolysis (TEN), which can be fatal. These serious events may occur without warning. Patients should be informed about the signs and symptoms of serious skin manifestations and use of the drug should be discontinued at the first appearance of skin rash or any other sign of hypersensitivity.
Rabeprazole: Rabeprazole is not recommended for use in children as there is no experience of its use in this group.
Cardiovascular Risk: Nonsteroidal anti-inflammatory drugs may cause an increased risk of serious cardiovascular thrombotic events, myocardial infarction and stroke, which can be fatal. This risk may increase with duration of use. Patients with cardiovascular disease or risk factors for cardiovascular disease may be at greater risk.
Aceclofenac is contraindicated for the treatment of peri-operative pain in the setting of coronary artery bypass graft (CABG) surgery.
Gastrointestinal Risk: Nonsteroidal anti-inflammatory drugs cause an increased risk of serious gastrointestinal adverse events including bleeding, ulceration and perforation of the stomach or intestines, which can be fatal. These events can occur at any time during use and without warning symptoms. Elderly patients are at greater risk for serious gastrointestinal events.
Hematologic Effects: Rabeprazole: There have been post-marketing reports of blood dyscrasias (thrombocytopenia and neutropenia). In the majority of cases where an alternative aetiology cannot be identified, the events were uncomplicated and resolved on discontinuation of rabeprazole.
Aceclofenac: Anemia is sometimes seen in patients receiving NSAIDs. This may be due to fluid retention, occult or gross gastrointestinal blood loss or an incompletely described effect upon erythropoiesis. Patients on long-term treatment with NSAIDs should have their hemoglobin or hematocrit checked if they exhibit any signs or symptoms of anemia. Nonsteroidal anti-inflammatory drugs inhibit platelet aggregation and have been shown to prolong bleeding time in some patients. Unlike aspirin, their effect on platelet function eg, those with coagulation disorders or patients receiving anticoagulants, should be carefully monitored.
Aceclofenac: General: Aceclofenac cannot be expected to substitute for corticosteroids or to treat corticosteroids insufficiency. Abrupt discontinuation of corticosteroids may lead to disease exacerbation. Patients on prolonged corticosteroid therapy should have their therapy tapered slowly if a decision is made to discontinue corticosteroids.
The pharmacological activity of aceclofenac in reducing inflammation may diminish the utility of these diagnostic signs in detecting complications of presumed noninfectious, painful conditions.
Hepatic Effects: Borderline elevations of ≥1 liver tests may occur in up to 15% of patients taking NSAIDs. These laboratory abnormalities may progress, may remain unchanged, or may be transient with continuing therapy. Notable elevations of alanine aminotransferase (ALT) or aspartate aminotransferase (AST) (approximately ≥3 times the upper limit of normal) have been reported in approximately 1% of patients in clinical trials with NSAIDs. In addition, rare cases of severe hepatic reactions, including jaundice and fatal fulminant hepatitis, liver necrosis and hepatic failure, some of them with fatal outcomes have been reported.
A patient with symptoms and/or signs suggesting liver dysfunction, or in whom an abnormal liver test has occurred, should be evaluated for evidence of the development of a more severe hepatic reaction while on therapy with aceclofenac, if clinical signs and symptoms consistent with liver disease develop, or if systemic manifestations occur (eg, eosinophilia, rash, etc), aceclofenac should be discontinued.
Preexisting Asthma: Patients with asthma may have aspirin-sensitive asthma. The use of aspirin in patients with aspirin-sensitive asthma has been associated with severe bronchospasm which can be fatal. Since cross reactivity, including bronchospasm, between aspirin and other nonsteroidal antiinflammatory drugs has been reported in such aspirin-sensitive patients, aceclofenac should not be administered to patients with this form of aspirin sensitivity and should be used with caution in patients with preexisting asthma.
Laboratory Tests: Because serious gastrointestinal tract ulcerations and bleeding can occur without warning symptoms, physicians should monitor for signs or symptoms of gastrointestinal bleeding. Patients on long-term treatment with NSAIDs should have their complete blood count (CBC) and a chemistry profile checked periodically. If clinical signs and symptoms consistent with liver or renal disease develop, systemic manifestations occur (eg, eosinophilia, rash, etc) or if abnormal liver tests persist or worsen, aceclofenac should be discontinued.
Rabeprazole: General: Symptomatic response to therapy with rabeprazole does not preclude the presence of gastric or esophageal malignancy; therefore, the possibility of malignancy should be excluded prior to commencing treatment with rabeprazole.
Patients on long-term treatment (particularly those treated for more than a year) should be kept under regular surveillance.
A risk of cross-hypersensitivity reactions with other proton-pump inhibitor or substituted benzimidazoles cannot be excluded.
Steady-state interactions of rabeprazole and warfarin have not been adequately evaluated in patients.
There have been reports of increased international normalised ratio (INR) and prothrombin time in patients receiving a PPIs and warfarin concomitantly. Increases in INR and prothrombin time may lead to abnormal bleeding and even death. Patients treated with a PPIs and warfarin concomitantly may need to be monitored for increases in INR and prothrombin time.
Hepatic enzyme abnormalities have been reported in clinical trials and as postmarketing adverse events. In the majority of cases where an alternative aetiology cannot be identified, the events were uncomplicated and resolved on discontinuation of rabeprazole. No evidence of significant drug-related safety problems were seen in a study of patients with mild to moderate hepatic impairment versus normal age and sex matched controls. However, because there are no clinical data on the use of rabeprazole in the treatment of patients with severe hepatic dysfunction, the physician is advised to exercise caution when treatment with rabeprazole is first initiated in such patients. Patients with healed gastroesophageal reflux disease (GERD) were treated for up to 40 months with rabeprazole and monitored with serial gastric biopsies. Patients without H. pylori infection (221 of 326 patients) had no clinically important pathologic changes in the gastric mucosa. Patients with H. pylori infection at baseline (105 of 326 patients) had mild or moderate inflammation in the gastric body or mild inflammation in the gastric antrum. Patients with mild grades of infection or inflammation in the gastric body tended to change to moderate, whereas those moderate at baseline tended to remain stable. Patients with mild grades of infection or inflammation in the gastric antrum tended to remain stable. At baseline, 8% of patients had atrophy of glands in the gastric body and 15% had atrophy in the gastric antrum. At endpoint, 15% of patients had atrophy of glands in the gastric body and 11% had atrophy in the gastric antrum. Approximately, 4% of patients had intestinal metaplasia at some point during follow-up, but no consistent changes were seen.
Co-administration of atazanavir with rabeprazole and its fixed-dose combination (FDCs) is not recommended (see Interactions).
Effects on the Ability to Drive or Operate Machinery: Aceclofenac: Patients suffering from dizziness, vertigo, or other central nervous system disorders whilst taking NSAIDs should refrain from driving or handling dangerous machinery.
Based on the pharmacodynamic properties and the adverse events profile, it is unlikely that rabeprazole would cause an impairment due to somnolence, it is recommended that driving and operating complex machinery be avoided.
Impairment of Fertility: NSAIDs may impair fertility and is not recommended in women trying to conceive. The temporary discontinuation of aceclofenac should be considered in women having difficulties to conceive or undergoing investigations for infertility.
Contraindicated in pregnancy and lactation, unless there are compelling reasons for doing so. The lowest effective dosage of NSAIDs should be used.
Aceclofenac: In late pregnancy, as with other NSAIDs, aceclofenac should be avoided because it may cause premature closure of the ductus arteriosus.
Rabeprazole: Teratology studies have been performed in rats at IV doses up to 50 mg/kg/day (plasma AUC of 11.8 mcg·hr/mL, about 13 times the human exposure at the recommended dose of GERD) and rabbits at IV doses up to 30 mg/kg/day (plasma AUC of 7.3 mcg·hr/mL, about 8 times the human exposure at the recommended dose for GERD) and have revealed no evidence of impaired fertility or harm to the fetus due to rabeprazole. There are, however, no adequate and well-controlled studies in pregnant women. Because animal reproduction studies are not always predictive of human response, Naclo-R should be used during pregnancy only if clearly needed.
Aceclofenac: The majority of adverse reactions reported have been reversible and of a minor nature. The most frequent are gastrointestinal disorders, in particular dyspepsia, abdominal pain, nausea and diarrhoea, and occasional occurrence of dizziness. Dermatological complaints including pruritis and rash and abnormal hepatic enzyme and serum creatinine levels have also been reported. If serious adverse reactions occur, aceclofenac should be withdrawn.
The following is a table of adverse reactions reported during clinical studies and after authorisation, grouped by system-organ class and estimated frequencies (see Table 1).
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Other rare or very rare class effects reported with NSAIDs in general are:
Blood and Lymphatic Disorders: Aplastic anaemia.
Psychiatric Disorders: Hallucination, confusional state.
Nervous System Disorder/s: Optic neuritis, somnolence.
Ear and Labyrinth Disorders: Tinnitus.
Respiratory, Thoracic and Mediastinal Disorders: Aggravated Asthma.
Gastrointestinal System: Duodenal ulcer, gastrointestinal perforation.
Skin and Subcutaneous Tissue Disorders: Toxic epidermal necrolysis, erythema multiforme, exfoliative dermatitis, photosensitivity reaction.
Renal and Urinary Disorders: Interstitial nephritis.
General Disorders and Administration Site Conditions: Malaise.
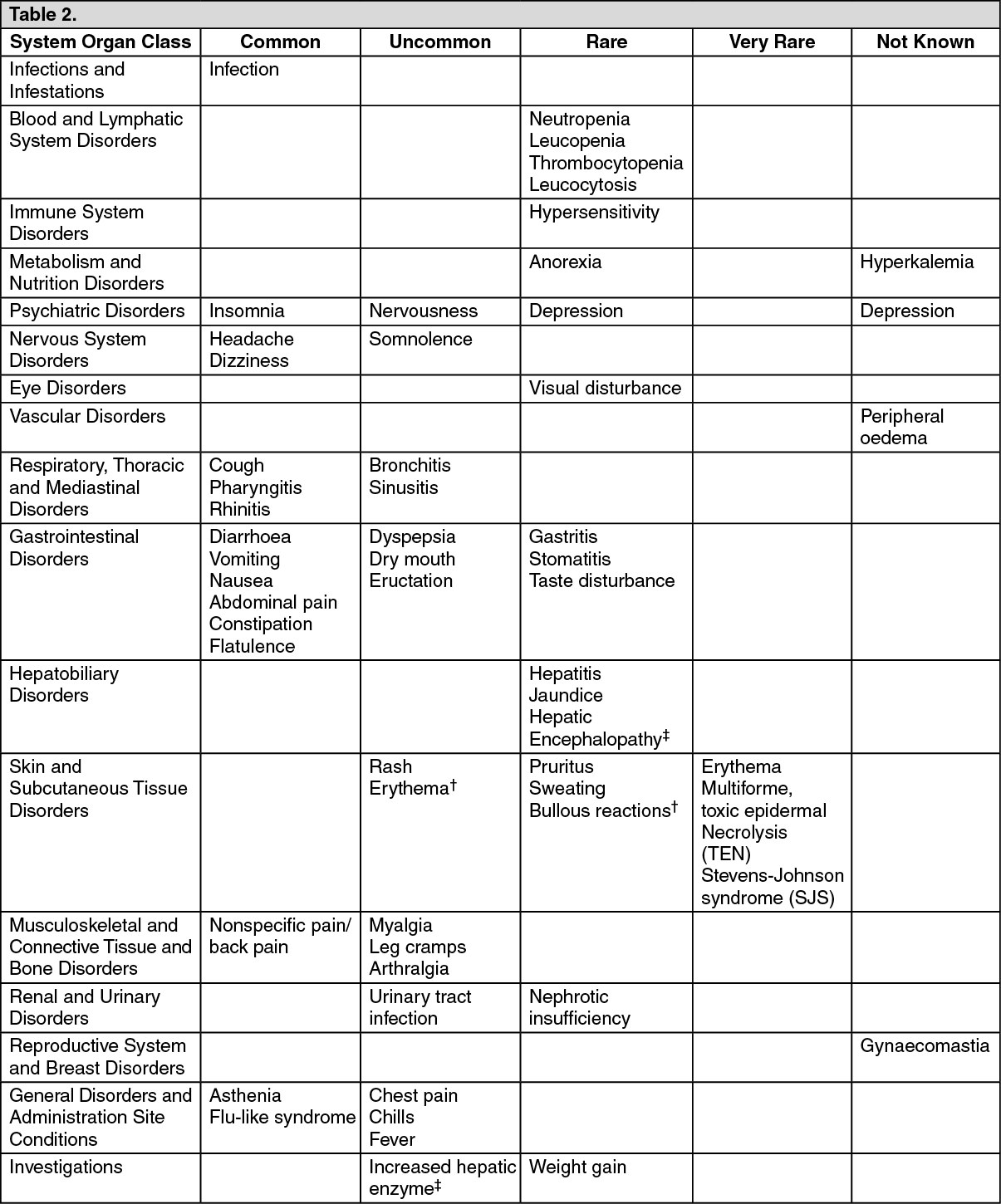
Rabeprazole: Rabeprazole were generally well-tolerated during clinical trials. The observed adverse reactions have been generally mild/moderate and transient in nature. The most common adverse events are headache, diarrhoea and nausea. Adverse reactions reported as more than isolated cases are listed as follows, by system organ class and by frequency.
The following adverse events have been reported from clinical trials and post-marketed experience. However of those adverse reactions reported in company sponsored clinical trials, only headache, diarrhoea, abdominal pain, asthenia, flatulence, rash and dry mouth were associated with the use of rabeprazole.
Frequencies are defined as: Common (>1/100, <1/10); uncommon (>1/1000, <1/100); rare (>1/10,000, <1/1/1000); and very rare (<1/10,000) (see Table 2).
Click on icon to see table/diagram/image
Aceclofenac: Lithium: NSAIDs have produced an elevation of plasma lithium levels and a reduction in renal lithium clearance. The mean minimum lithium concentration increased 15% and the renal clearance was decreased by approximately 20%. These effects have been attributed to inhibition of renal prostaglandin synthesis by the NSAID. Thus, when NSAIDs and lithium are administered concurrently, subjects should be observed carefully for signs of lithium toxicity.
Cardiac Glycoside: Through their renal effects, NSAIDs may increase plasma glycoside (including digoxin) levels, exacerbate cardiac failure and reduce the glomerular filtration rate in patients receiving glycosides.
Diuretics: Aceclofenac, like other NSAIDs, may inhibit the activity of diuretics. Although it was not shown to affect blood pressure control when co-administered with bendrofluazide, interactions with other diuretics cannot be ruled out. When concomitant administration with potassium-sparing diuretics is employed, serum potassium should be monitored. Diuretics can increase the risk of nephrotoxicity of NSAIDs.
Anticoagulants: Like other NSAIDs, aceclofenac may enhance the activity of anticoagulants. Close monitoring of patients on combined anticoagulant and aceclofenac therapy should be undertaken. The effects of warfarin and NSAIDs on gastrointestinal bleeding are synergistic, such that users of both drugs together have a risk of serious gastrointestinal bleeding higher than users of either drug alone.
Antidiabetic Agents: Clinical studies have shown that diclofenac can be given together with oral antidiabetic agents without influencing their clinical effect. However, there have been isolated reports of hypoglycaemic and hyperglycaemic effects. Thus with aceclofenac, consideration should be given to adjustment of the dosage of hypoglycaemic agents.
Methotrexate: Caution should be exercised if NSAIDs and methotrexate are administered within 24 hrs of each other, since NSAIDs may increase plasma levels, resulting in increased toxicity.
Mifepristone: NSAIDs should not be used for 8-12 days after mifepristone administration as NSAIDs can reduce the effect of mifepristone.
Other NSAIDs and Steroids: Concomitant therapy with aspirin, other NSAIDs and steroids may increase the bleeding.
Cyclosporine: Cyclosporine nephrotoxicity may be increased by the effect of NSAIDs on renal prostaglandins.
Quinolone Antimicrobials: Convulsions may occur due to an interaction between quinolones and NSAIDs. This may occur in patients with or without previous history of epilepsy or convulsions. Therefore, caution should be exercised when considering the use of a quinolone in patients who are already receiving NSAIDs.
ACE Inhibitors: Reports suggest that NSAIDs may diminish the antihypertensive effect of ACE inhibitors. This interaction should be given consideration in patients taking NSAIDs concomitantly with ACE inhibitors.
Rabeprazole: Rabeprazole is metabolized by the CYP450 drug metabolizing enzyme system. Studies in healthy subjects have shown that rabeprazole does not have clinically significant interactions with other drugs metabolized by the CYP450 system eg, warfarin and theophylline given as single oral doses, diazepam as a single IV dose, and phenytoin given as a single IV dose (with supplemental oral dosing). Steady-state interactions with rabeprazole and other drugs metabolized by this enzyme system have not been studied in patients; There have been reports of increased INR and prothrombin time may lead to abnormal bleeding and even death.
In vitro incubations employing human liver microsomes indicated that rabeprazole inhibited cyclosporine metabolism with an IC50 of 62 micromolar, a concentration that is over 50 times higher than the Cmax in healthy volunteers following 14 days of dosing with 20 mg of rabeprazole. This degree of inhibition is similar to that by omeprazole at equivalent concentrations.
Rabeprazole sodium produces a profound and long lasting inhibition of gastric acid secretion. An interaction with compounds whose absorption is pH-dependent may occur. Co-administration of rabeprazole sodium with ketoconazole or itraconazole may result in a significant decrease in antifungal plasma levels. Therefore, individual patients may need to be monitored to determine if a dosage adjustment is necessary when ketoconazole or itraconazole are taken concomitantly with rabeprazole. For example, in normal subjects, co-administration of rabeprazole 20 mg 4 times a day. resulted in approximately 30% decrease in the bioavailability of ketoconazole and increase in the AUC and Cmax for digoxin of 19% and 29%, respectively. Therefore, patients may need to be monitored when such drugs are taken concomitantly with rabeprazole. Co-administration of rabeprazole and antacids produced no clinically relevant changes in plasma rabeprazole concentrations.
Concomitant use of atazanavir and PPIs is not recommended. Co-administration of atazanavir with PPIs is expected to substantially decrease atazanavir plasma concentrations and thereby reduce its therapeutic effect.
In a clinical study in Japan evaluating rabeprazole in patients categorized by CYP2C19 genotype (n=6 per genotype category), gastric and suppression was higher in poor metabolizers as compared to extensive metabolizers. This could be due to higher rabeprazole plasma levels in poor metabolizers. Whether or not interactions of rabeprazole sodium with other drugs metabolized by CYP2C19 would be different between extensive metabolizers and poor metabolizers has not been studied. Combined administration consisting of rabeprazole, amoxicillin, and clarithromycin resulted in increases in plasma concentrations of rabeprazole and 14-hydroxyclarithromycin.
Store below 25°C. Protect from light and moisture.
Shelf-Life: 18 months.
M01AB16 - aceclofenac ; Belongs to the class of acetic acid derivatives and related substances of non-steroidal antiinflammatory and antirheumatic products.
Cap 200 mg/20 mg x 3 x 10's.



 Sign Out
Sign Out