Pharmacology: Pharmacodynamics: General Properties: Linezolid is a synthetic antibacterial agent that belongs to a new class of antimicrobials, the oxazolidinones. It has
in vitro activity against aerobic Gram-positive bacteria, some Gram-negative bacteria and anaerobic microorganisms. Linezolid selectively inhibits bacterial protein synthesis via a unique mechanism of action. Specifically, it binds to a site on the bacterial ribosome (23S of the 50S subunit) and prevents the formation of a functional 70S initiation complex which is an essential component of the translation process.
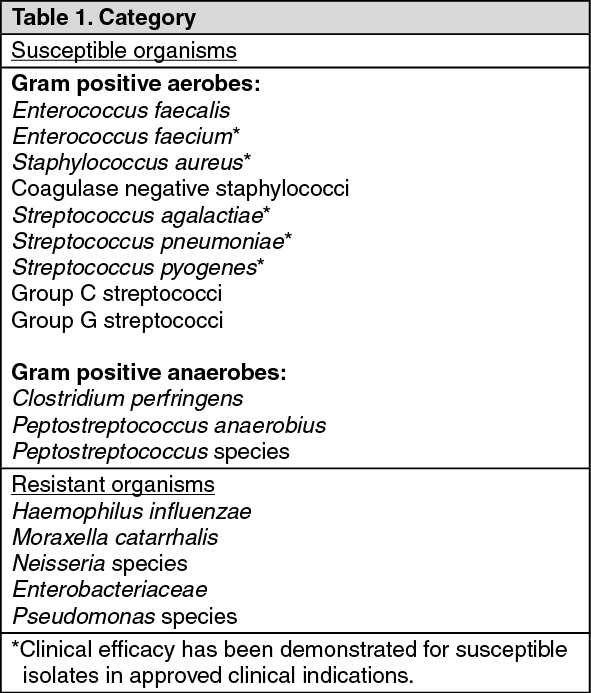
Susceptibility: Only microorganisms relevant to the given clinical indications are presented as follows. (See Table 1.)
 Click on icon to see table/diagram/image
Pharmacokinetics: Absorption:
Click on icon to see table/diagram/image
Pharmacokinetics: Absorption: Linezolid is rapidly and extensively absorbed following oral dosing. Maximum plasma concentrations are reached within 2 hours of dosing. Absolute oral bioavailability of linezolid (oral and intravenous dosing in a crossover study) is complete (approximately 100%).
Plasma linezolid C
max and C
min (mean and [SD]) at steady-state following twice daily intravenous dosing of 600 mg have been determined to be 15.1 [2.5] mg/l and 3.68 [2.68] mg/l, respectively.
In another study following oral dosing of 600 mg twice daily to steady-state, C
max and C
min were determined to be 21.2 [5.8] mg/l and 6.15 [2.94] mg/l, respectively. Steady-state conditions are achieved by the second day of dosing.
Distribution: Volume of distribution at steady-state averages at about 40-50 litres in healthy adults and approximates to total body water. Plasma protein binding is about 31% and is not concentration dependent.
Linezolid concentrations have been determined in various fluids from a limited number of subjects in volunteer studies following multiple dosing. The ratio of linezolid in saliva and sweat relative to plasma was 1.2:1.0 and 0.55:1.0, respectively. The ratio for epithelial lining fluid and alveolar cells of the lung was 4.5:1.0 and 0.15:1.0, when measured at steady-state C
max, respectively.
Pharmacokinetic information generated in pediatric patients with ventriculoperitoneal shunts showed variable cerebrospinal fluid (CSF) linezolid concentrations following single and multiple dosing of linezolid; therapeutic concentrations were not consistently achieved or maintained in the CSF. Therefore, the use of linezolid for the empiric treatment of pediatric patients with central nervous system infections is not recommended.
Metabolism: Linezolid is primarily metabolized by oxidation of the morpholine ring resulting mainly in the formation of two inactive open-ring carboxylic acid derivatives: the aminoethoxyacetic acid metabolite (PNU-142300) and the hydroxyethyl glycine metabolite (PNU-142586). The hydroxyethyl glycine metabolite (PNU-142586) is the predominant human metabolite and is believed to be formed by a non-enzymatic process. The aminoethoxyacetic acid metabolite (PNU-142300) is less abundant. Other minor, inactive metabolites have been characterised.
Elimination: In patients with normal renal function or mild to moderate renal insufficiency, linezolid is primarily excreted under steady-state conditions in the urine as PNU-142586 (40%), parent drug (30%) and PNU-142300 (10%). Virtually no parent drug is found in the feces while approximately 6% and 3% of each dose appears as PNU-142586 and PNU-142300, respectively. The elimination half-life of linezolid averages at about 5-7 hours.
Non-renal clearance accounts for approximately 65% of the total clearance of linezolid. A small degree of non-linearity in clearance is observed with increasing doses of linezolid. This appears to be due to lower renal and non-renal clearance at higher linezolid concentrations. However, the difference in clearance is small and is not reflected in the apparent elimination half-life.
Special Populations: Patients with renal insufficiency: After single doses of 600 mg, there was a 7-8 fold increase in exposure to the two primary metabolites of linezolid in the plasma of patients with severe renal insufficiency (i.e. creatinine clearance <30 mL/min). However, there was no increase in AUC of parent drug. Although there is some removal of the major metabolites of linezolid by hemodialysis, metabolite plasma levels after single 600 mg doses were still considerably higher following dialysis than those observed in patients with normal renal function or mild to moderate renal insufficiency.
In 24 patients with severe renal insufficiency, 21 of whom were on regular hemodialysis, peak plasma concentrations of the two major metabolites after several days dosing were about 10 fold those seen in patients with normal renal function. Peak plasma levels of linezolid were not affected.
The clinical significance of these observations has not been established as limited safety data are currently available (see Dosage & Administration).
Patients with hepatic insufficiency: Limited data indicate that the pharmacokinetics of linezolid, PNU-142300 and PNU-142586 are not altered in patients with mild to moderate hepatic insufficiency (i.e. Child-Pugh class A or B). The pharmacokinetics of linezolid in patients with severe hepatic insufficiency (i.e. Child-Pugh class C) have not been evaluated. However, as linezolid is metabolized by a non-enzymatic process, impairment of hepatic function would not be expected to significantly alter its metabolism (see Dosage & Administration).
Children and adolescents (<18 years old): In adolescents (12 to 17 years old), linezolid pharmacokinetics were similar to that in adults following a 600 mg dose. Therefore, adolescents administered 600 mg every 12 hours daily will have similar exposure to that observed in adults receiving the same dosage.
In children 1 week to 12 years old, administration of 10 mg/kg every 8 hours daily gave exposure approximating to that achieved with 600 mg twice daily in adults.
In neonates up to 1 week of age, the systemic clearance of linezolid (based on kg body weight) increases rapidly in the first week of life. Therefore, neonates given 10 mg/kg every 8 hours daily will have the greatest systemic exposure on the first day after delivery. However, excessive accumulation is not expected with this dosage regimen during the first week of life as clearance increases rapidly over that period.
Elderly patients: The pharmacokinetics of linezolid are not significantly altered in elderly patients (aged 65 and over).
Female patients: Females have a slightly lower volume of distribution than males and the mean clearance is reduced by approximately 20% when corrected for body weight. Plasma concentrations are higher in females and this can partly be attributed to body weight differences. However, because the mean half-life of linezolid is not significantly different in males and females, plasma concentrations in females are not expected to substantially rise above those known to be well tolerated and, therefore, dose adjustments are not required.
Toxicology: Preclinical safety data: Linezolid decreased fertility and reproductive performance of male rats at exposure levels approximately equal to those expected in humans. In sexually mature animals these effects were reversible. The reversible effects on fertility were mediated by altered spermatogenesis. Affected spermatids contained abnormally formed and oriented mitochondria and were non-viable. The presence of abnormal sperm in the epididymis was accompanied by epithelial cell hypertrophy and hyperplasia. Epididymal hypertrophy was not observed in dogs treated for 1 month, although changes in the weights of prostate, testes and epididymis were apparent.
Sexually mature male rats showed slightly decreased fertility following oral treatment as juveniles throughout most of their period of sexual development (50 mg/kg/day from postnatal days 7 to 36, and 100 mg/kg/day from days 37 to 55), at exposures up to 1.7 times the mean AUC in pediatric patients aged 3 months to 11 years. Decreased fertility was not observed following shorter treatment periods
in utero through the early neonatal period (gestation day 6 through postnatal day 5), neonatal exposure (postnatal days 5 to 21), or juvenile exposure (postnatal days 22 to 35). Reversible reductions in sperm motility and altered sperm morphology were observed in rats following treatment on postnatal days 22 to 35.
Reproductive toxicity studies in mice and rats showed no evidence of a teratogenic effect at exposure levels 4 times or equivalent, respectively, to those expected in humans. The same linezolid concentrations caused maternal toxicity in mice and were related to increased embryo death including total litter loss, decreased fetal body weight and an exacerbation of the normal genetic predisposition to sternal variations in the strain of mice. In rats, slight maternal toxicity was noted at exposures lower than expected clinical exposures. Mild fetal toxicity, manifested as decreased fetal body weights, reduced ossification of sternebrae, reduced pup survival and mild maturational delays were noted. When mated, these same pups showed evidence of a reversible dose-related increase in pre-implantation loss with a corresponding decrease in fertility.
Linezolid was also not teratogenic in rabbits when administered twice daily at total oral doses up to 15 mg/kg/day (0.06 times the clinical exposure, based on AUC). Maternal toxicity (clinical signs, reduced body weight gain and food consumption) occurred at 5 and 15 mg/kg/day, and reduced fetal body weight occurred at 15 mg/kg/day. Linezolid exposures were low due to the characteristic sensitivity of rabbits to antibiotics.
Linezolid and its metabolites are excreted into the milk of lactating rats and the concentrations observed were higher than those in maternal plasma.
Linezolid produced reversible myelosuppression in adult and juvenile rats and dogs.
In rats administered linezolid orally for 6 months, non-reversible, minimal to mild axonal degeneration of sciatic nerves was observed at 80 mg/kg/day; minimal degeneration of the sciatic nerve was also observed in 1 male at this dose level at a 3-month interim necropsy. Sensitive morphologic evaluation of perfusion-fixed tissues was conducted to investigate evidence of optic nerve degeneration. Minimal to moderate optic nerve degeneration was evident in 2 male rats administered linezolid at 80 mg/kg/day for 6 months, but the direct relationship to drug was equivocal because of the acute nature of the finding and its asymmetrical distribution. The nerve degeneration observed was microscopically comparable to a spontaneous unilateral optic nerve degeneration reported in aging rats and may be an exacerbation of a common background change.





 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image


 Sign Out
Sign Out
