Tianeptine sodium salt 12.5 mg for one coated tablet.
Excipients with known effect: sucrose.
Excipients/Inactive Ingredients: D-mannitol, maize starch, talc, magnesium stearate.
Coating: ethylcellulose, glycerol oleate, SEPIFILM SE 700 White (polyvidone, carmellose sodium, anhydrous colloidal silica, talc, sucrose, polysorbate 80, titanium dioxide, sodium bicarbonate), white beeswax.
Pharmacotherapeutic class: OTHER ANTIDEPRESSANTS. ATC code: N06AX14.
Pharmacology: Pharmacodynamics: Mechanism of action: Tianeptine is an antidepressant: Tianeptine has the following characteristics in animals: tianeptine increases the spontaneous activity of pyramidal cells in the hippocampus and accelerates their recovery after functional inhibition, tianeptine increases the rate of serotonin re-uptake by neurons in the cortex and hippocampus.
In vitro, tianeptine has no affinity for monoaminergic receptors and does not inhibit serotonin (5-HT), noradrenaline (NA) or dopamine (DA) re-uptake. Tianeptine can modulate synaptic glutamatergic neuro-transmission.
The specific contribution of each effect to the antidepressant activity is unknown.
Clinical efficacy and safety: Four double-blind, placebo-controlled trials were performed to evaluate the short-term efficacy of tianeptine in the treatment of major depressive episodes in adults: one at fixed doses (37.5 mg, 75 mg) and two with possibility to adjust the dosage to a higher or lower dose (initial dose 37.5 mg, then 25, 37.5 or 50 mg) and one in elderly patients (311 patients aged 65 years and above; ~100 patients by treatment arm, including ~20 patients above 75 years in each arm) with a potential dose increase according to patient improvement after 2 weeks of treatment (25 mg then 25mg or 50 mg). In the adult studies, primary endpoint was change in MADRS total score from baseline for the fixed and flexible dose trials.
At the end of treatment (6 weeks), the efficacy of tianeptine was significant in the two flexible dose trials but not in the fixed dose trial. In a trial, imipramine, used as an active comparator, demonstrated the sensitivity of the trial. In the elderly study (potential dose increase trial), after 8 weeks of treatment, significant efficacy of tianeptine was demonstrated on the primary endpoint (HAMD total score change from baseline). The active control, escitalopram, used in this trial showed assay sensitivity.
The maintenance of the antidepressant efficacy was evaluated in a relapse and recurrence prevention trial. Patients considered as responding to treatment by the investigator (6 weeks of "open" treatment with tianeptine at a daily dosage of 2 to 4 tablets, i.e. 25 to 50 mg daily) were randomised to tianeptine or placebo for an additional duration of 16.5 months. Tianeptine showed a statistically significant efficacy superiority with respect to placebo (p < 0.001) on the main criterion of the trial: prevention of relapse or recurrence measured by the time to their onset. The incidence of relapse after 6 months of double-blind follow-up was 6% for tianeptine and 22% for placebo. The incidence of relapse or recurrence after 18 months of double-blind follow-up was 16% for tianeptine and 36% for placebo.
Pharmacokinetics: Absorption: Gastrointestinal absorption is rapid and complete.
Distribution: Distribution is rapid and is associated with protein binding of nearly 94 %, primarily to albumin.
Biotransformation: Tianeptine is extensively metabolised by the liver, primarily by beta-oxidation, without CYP450 involvement. Its main metabolite, pentanoic acid (MC5), is active and less potent than tianeptine.
Elimination: The elimination of tianeptine is characterised by a short terminal half-life of 3 h, most of the metabolites are excreted in the urine.
Elderly, very elderly and fragile patients: In elderly patients, tianeptine plasma concentrations increased by 30% and those of MC5 were nearly doubled after single or repeated administration, compared to that of younger patients (see Dosage & Administration).
In very elderly (87 ± 5 years) or fragile (45 ± 9 kg), a significant increase of Cmax and exposure (area under the curve, AUC) to tianeptine and MC5 were observed after a single administration (see Dosage & Administration).
Patients with severe renal failure (ClCr < 19 ml/min): The pharmacokinetics of tianeptine remain unchanged but the exposure to MC5 is nearly doubled after single and repeated administration (see Dosage & Administration).
Patients with severe liver cirrhosis (Class C, Child-Pugh Score): Exposure to tianeptine and MC5, after the administration of a 12.5 mg dose, are increased compared to that of adult depressive patients (see Dosage & Administration).
In case of milder cirrhosis, such as chronic alcoholics, the effects on the pharmacokinetic parameters are insignificant (see Dosage & Administration).
Toxicology: Preclinical safety data: Non-clinical data from conventional genotoxicity and carcinogenesis studies have not revealed any specific risk for humans.
In the fertility study, an increase in pre-implantation losses was observed at the maternotoxic dose of 45 mg/kg/day (i.e. 12 times the human dose determined with respect to the body surface).
Tianeptine is not teratogenic in rats and rabbits.
In the peri- and post-natal study, a lactic secretion dysfunction and an increase in post-implantation and post-natal losses have been observed in rats at the maternotoxic dose of 45 mg/kg/day (i.e. 12 times the human dose determined with respect to the body surface).
Neurotic and reactive depression.
Anxio-depressive states with psychosomatic manifestations, especially gastrointestinal.
Anxio-depressive states in alcoholic during withdrawal stage.
Posology: The recommended dosage is one tablet containing 12.5 mg, three times a day (morning, midday and evening) at the beginning of the main meals.
Special populations: Elderly subjects: The efficacy and safety of tianeptine have been established in elderly depressed patients (≥ 65 years) (see Pharmacology: Pharmacodynamics under Actions). No dose adjustment is required in relation to age.
In frail elderly patients (< 55 kg), the dosage should be restricted to 2 tablets per day (see Pharmacology: Pharmacokinetics under Actions).
Renal failure: In patients with severe renal failure (ClCr < 19 ml/min), the posology should be restricted to 2 tablets per day (see Pharmacology: Pharmacokinetics under Actions).
Hepatic impairment: In patients with severe cirrhosis (Class C, Child Pugh Score), the posology should be restricted to 2 tablets per day (see Pharmacology: Pharmacokinetics under Actions).
In chronic alcoholic patients, irrespective of whether they have mild or moderate cirrhosis or no cirrhosis, the posology does not need to be adjusted (see Pharmacology: Pharmacokinetics under Actions).
Paediatric population: The safety and efficacy of tianeptine in children and adolescents under 18 years of age have not been determined. There is no data available (see Precautions).
Tianeptine is contraindicated in children and adolescents under 15 years old (see Contraindications).
Discontinuation of treatment: Abrupt discontinuation of the treatment should be avoided. The dosage should be gradually reduced over a period of 7 to 14 days in order to reduce the risk of withdrawal reactions (see Precautions).
Method of administration: Oral route.
Symptoms: The experience concerning cases of acute tianeptine intoxication (maximum quantity: 2250 mg, ingested in a single dose) primarily reveals alertness disorders which can lead to coma, especially in case of multiple intoxications.
Recommended procedure: Tianeptine has no known specific antidote. In case of acute intoxication, a symptomatic treatment and routine monitoring must be started. Medical monitoring in a specialised setting is recommended.
Hypersensitivity to the drug substance or to any of the excipients mentioned in Description.
Children and adolescents under 15 years old.
Suicide/suicidal thoughts or clinical worsening: Depression is associated with an increased risk of suicidal thoughts, self-harming and suicide (suicidal behaviour). This risk persists until a significant remission has been obtained. C
Patients with a history of suicidal type behaviour or those expressing significant suicidal thoughts before starting the treatment face a higher risk of the onset of suicidal thoughts or suicidal type behaviour, and must be closely monitored during treatment. A meta-analysis of placebo-controlled clinical trials of the use of antidepressants in adults displaying psychiatric disorders has revealed an increase in the risk of suicidal behaviour in patients under 25 years of age treated with antidepressants compared to those receiving a placebo. Careful monitoring of patients, and particularly of high-risk patients, must accompany the use of this drug treatment, particularly at the beginning of treatment and at times of dose changes.
The patients (and their family and friends) must be warned of the need to monitor the onset of clinical worsening, the appearance of suicidal-thoughts/behaviour and any abnormal change of behaviour, and to seek medical advice immediately if such symptoms arise.
In case of general anaesthesia, the anaesthetist should be informed of the treatment, and the treatment discontinued 24 or 48 hours prior to surgery.
In case of emergency, surgery may still be performed without prior discontinuation; under peroperative monitoring.
As with any psychotropic treatment, the administration of this medicinal product with alcoholic beverages or medicinal products containing alcohol is inadvisable.
Do not exceed the recommended doses.
Abuse/dependence and withdrawal syndrome: In case of a history of drug-dependence or alcohol-dependence, the patients must be very closely monitored in order to avoid any increase in dosage.
After discontinuation of treatment with tianeptine, withdrawal symptoms have been observed in some patients. The following events have been observed: anxiety, muscle pain, abdominal pain, insomnia, joint pain. When the treatment is started, the patient should be informed on the risk of withdrawal syndrome at discontinuation.
If the treatment is to be interrupted, the dosage should be gradually reduced over a period of 7 to 14 days in order to reduce the risk of withdrawal reactions (see Dosage & Administration).
A combination with MAOI is inadvisable (see Interactions). It is necessary to allow a free interval: of two weeks when tianeptine is used as a replacement of MAOI, of 24 hours when a MAOI is used as a replacement of tianeptine.
Hyponatraemia: Hyponatraemia, probably due to a syndrome of inappropriate anti-diuretic hormone secretion (SIADH), has been reported with the use of tianeptine. The majority of cases were reported in the elderly, especially when coupled with a recent history of, or condition pre-disposing to, altered fluid balance. Caution should be exercised in patients at increased risk for hyponatraemia, such as elderly, cirrhotic, or dehydrated patients or those treated with diuretics.
This medicinal product contains sucrose. Its use is inadvisable in patients with fructose intolerance, glucose and galactose malabsorption syndrome or sucrase-isomaltase deficiency (rare hereditary diseases).
Level of sodium: This medicine contains less than 1 mmol sodium (23 mg) per coated-tablet, i.e. essentially 'sodium-free'.
Effects on ability to drive and use machines: Diminished alertness could appear in some patients. Therefore, the attention of drivers and users of machines should be drawn to the risks of drowsiness attached to the use of this medicinal product.
Use in Children: STABLON is contraindicated in children and adolescents under 15 years old (see Contraindications) and should not be used in adolescents aged 15 to 18 years. Suicidal type behaviours (suicide attempts and suicidal thoughts) and hostile type behaviour (mainly aggressiveness, opposition behaviour and anger) have been observed more frequently during clinical studies in children and adolescents treated with antidepressants compared to those treated with placebo. If the decision to treat is nonetheless taken, in case of clinical need, the patient must be closely monitored to detect the appearance of suicidal symptoms. Furthermore, there is no long-term safety data in children and adolescents, concerning growth, sexual maturation and cognitive and behavioural development.
Pregnancy: An increase in post-implantation and post-natal losses were observed in a peri- and post-natal study in rats at maternal toxic doses (see Pharmacology: Toxicology: Preclinical safety data under Actions).
There is no data or limited data (less than 300 pregnancies) on the use of tianeptine in pregnant women.
It is therefore preferable to avoid the use of tianeptine during pregnancy, irrespective of the term.
It is preferable to maintain a balanced maternal psychic equilibrium throughout pregnancy. If a drug treatment with tianeptine is required to maintain this equilibrium, the treatment must be started or continued at the effective dose throughout the pregnancy and if possible in monotherapy and the pharmacological profile of the molecule must be taken into account when monitoring the newborn baby.
Lactation: Lactic secretion dysfunction has been observed in rats at materno-toxic doses (see Pharmacology: Toxicology: Preclinical safety data under Actions).
Tricyclic antidepressants are excreted into breast milk, therefore, breast-feeding is not recommended for the duration of the treatment.
Fertility: In rats, a study showed a decrease in the reproductory performance (increase of pre-implantation losses), at materno-toxic doses. (see Pharmacology: Toxicology: Preclinical safety data under Actions).
The clinical impact is unknown.
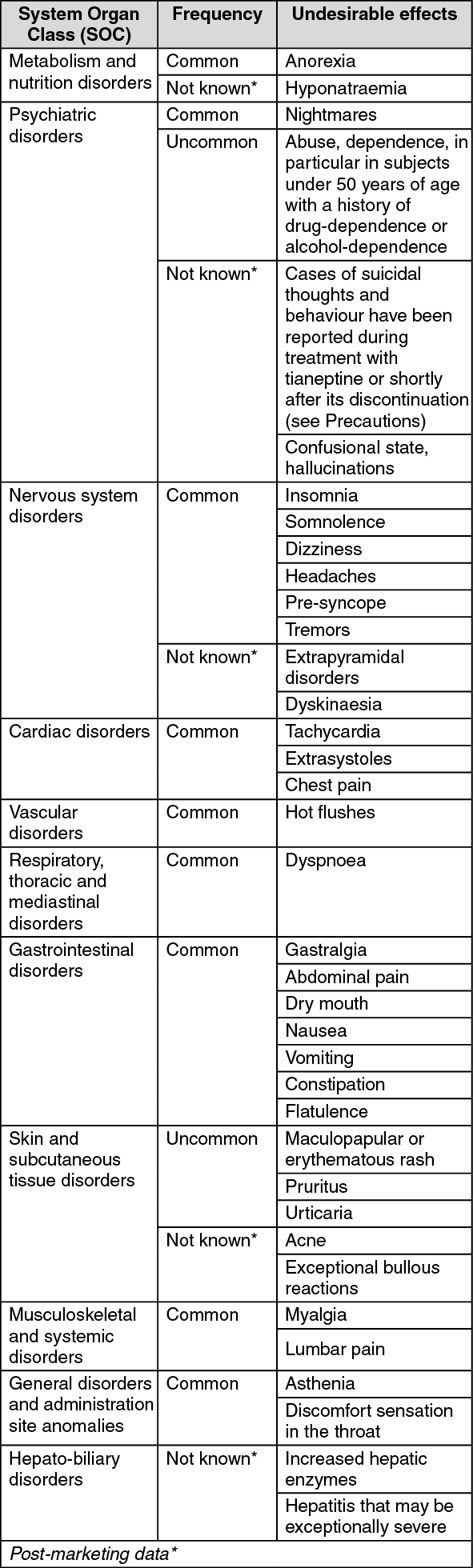
Summary of the safety profile: The undesirable effects observed with tianeptine during clinical trials are moderate in intensity. They consist primarily of nausea, constipation, abdominal pain, drowsiness, headaches, dry mouth and vertigo.
Table of undesirable effects: The following undesirable effects have been observed during clinical trials and/or post-MA use of tianeptine and are classified as a function of their frequency: Very common (≥1/10); common (≥1/100, <1/10); uncommon (≥1/1,000, <1/100); rare (≥1/10,000, <1/1,000); very rare (<1/10,000), and not known (cannot be estimated from the available data). (See table.)
 Click on icon to see table/diagram/image
Reporting of suspected adverse reactions:
Click on icon to see table/diagram/image
Reporting of suspected adverse reactions: Reporting suspected adverse reactions after authorisation of the medicinal product is important. It allows continued monitoring of the benefit/risk balance of the medicinal product. Healthcare professionals are asked to report any suspected adverse reactions via the national reporting system.
Concomitant use not recommended: Irreversible MAOIs (iproniazide): due to risk of cardiovascular collapse or paroxysmal hypertension, hyperthermia, convulsions, death.
Incompatibilities: Not applicable.
Store at a temperature below 30°C.
Shelf life: 36 months.
N06AX14 - tianeptine ; Belongs to the class of other antidepressants.
Stablon coated tab 12.5 mg
30's


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out
