


 Sign Out
Sign Out

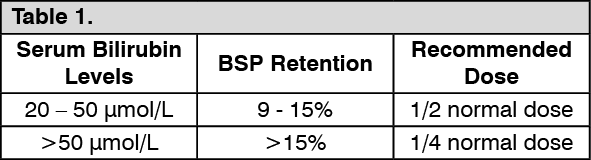
Use in Hepatic Impairment: Doxorubicin dosage must be reduced if hepatic function is impaired according to the following table: (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageMethod of Administration: ROBOL Injection is supplied as 10 mg doxorubicin hydrochloride in 5 mL vials, 50 mg doxorubicin hydrochloride in 25 mL vials and 200 mg doxorubicin hydrochloride in 100 mL vials respectively (doxorubicin concentration 2 mg/mL).
Doxorubicin Injection must be handled with care. If contact with the skin occurs, wash thoroughly with soap and water. The product contains no antimicrobial preservative. The single dose vials should be used in one patient on one occasion only. Discard any residue. The solution is to be stored under refrigeration (2°C to 8°C) and should be protected from sunlight and retained in the carton until time of use.
Storage of doxorubicin at refrigerated conditions can result in the formation of a gelled product. This gelled product will return to a slightly viscous to mobile solution after two to a maximum of four hours equilibration at room temperature (20°C to 25°C).
It is recommended that doxorubicin be slowly administered into the tubing of a freely running intravenous infusion of Sodium Chloride Injection or 5% Glucose Injection. The tubing should be attached to a butterfly needle inserted preferably into a large vein. The rate of administration is dependent on the size of the vein and the dosage. However, the dose should be administered in not less than 3-5 minutes. A direct push injection is not recommended due to the risk of extravasation, which may occur even in the presence of adequate blood return upon needle aspiration.
Local erythematous streaking along the vein as well as facial flushing may be indicative of too rapid administration. A burning or stinging sensation may be indicative of perivenous infiltration and the infusion should be immediately terminated and restarted in another vein.
Until specific compatibility data are available, it is not recommended that doxorubicin be mixed with other drugs. Contact with alkaline solutions should be avoided since this can lead to hydrolysis of doxorubicin. Doxorubicin should not be mixed with heparin due to chemical incompatibility that may lead to precipitation.
Doxorubicin should not be mixed with fluorouracil (e.g., in the same IV infusion bag or at the Y-site of an IV infusion line) since it has been reported that these drugs are incompatible to the extent that a precipitate might form. If concomitant therapy with doxorubicin and fluorouracil is required, it is recommended that the IV line be flushed between the administrations of these drugs.
Doxorubicin has been used in combination with other approved chemotherapeutic agents.
Though evidence is available that at least in some types of neoplastic disease combination chemotherapy is superior to single agents the benefits and risks of such therapy have not yet been fully elucidated.
Doxorubicin must not be given intrathecally or intramuscularly or by long-term infusion. Direct intravenous infusion is not advised due to the tissue damage that may occur if the infusion infiltrates the tissues. If a central vein catheter is used then infusion of doxorubicin in sodium chloride 0.9 % injection is advised.
Protective Measures: The following protective recommendations are given due to the toxic nature of this substance: Personnel should be trained in good technique for reconstitution and handling.
Pregnant staff should be excluded from working with this drug.
Personnel handling doxorubicin should wear protective clothing: goggles, gowns and disposable gloves and masks.
A designated area should be defined for reconstitution (preferably under a laminar flow system). The work surface should be protected by disposable, plastic-backed, absorbent paper.
All items used for reconstitution, administration or cleaning, including gloves, should be placed in high-risk waste-disposal bags for high-temperature incineration.
Spillage or leakage should be treated with dilute sodium hypochlorite (1% available chlorine) solution, preferably by soaking, and then water.
All cleaning materials should be disposed of as indicated previously.
In case of skin contact thoroughly wash the affected area with soap and water or sodium bicarbonate solution. However, do not abrade the skin by using a scrub brush.
In case of contact with the eye(s), hold back the eyelid(s) and flush the affected eye(s) with copious amounts of water for at least 15 minutes. Then seek medical evaluation by a physician.
Always wash hands after removing gloves.
Method of Administration: Intravesical Administration: The following procedure is recommended: 1. The bladder should be catheterised and emptied.
2. Dilute ROBOL to a final concentration of 80 mg in 100 mL of normal saline and instill via the catheter into the bladder.
3. The catheter should be removed and the patient instructed to be on one side. At 15 minute intervals the patient should alternate to the opposite side over a 1-hour period.
4. The patient should be requested not to urinate for 1 hour, after which the bladder should be emptied of solution.
5. The procedure should be repeated at monthly intervals.
Route of Administration: Intravenous and Intravesical.