The information highlighted (if any) are the most recent updates for this brand.
The tablets contain amlodipine besilate equivalent to 5 mg and 10 mg amlodipine.
The 5 mg tablet can be divided into equal halves.
Excipients/Inactive Ingredients: Microcrystalline cellulose, anhydrous dibasic calcium phosphate, sodium starch glycolate, magnesium stearate.
Pharmacology: Pharmacodynamics: Amlodipine is a calcium ion influx inhibitor (slow channel blocker or calcium ion antagonist) and inhibits the transmembrane influx of calcium ions into cardiac and vascular smooth muscle.
The mechanism of the antihypertensive action of amlodipine is due to a direct relaxant effect on vascular smooth muscle. The precise mechanism by which amlodipine relieves angina has not been fully determined, but amlodipine reduces total ischemic burden by the following two actions: 1) Amlodipine dilates peripheral arterioles and thus reduces the total peripheral resistance (afterload) against which the heart works. Since the heart rate remains stable, this unloading of the heart reduces myocardial energy consumption and oxygen requirements.
2) The mechanism of action of amlodipine also probably involves dilatation of the main coronary arteries and coronary arterioles, both in normal and ischemic regions. This dilatation increases myocardial oxygen delivery in patients with coronary artery spasm (Prinzmetal's or variant angina) and blunts smoking-induced coronary vasoconstriction.
In patients with hypertension, once-daily dosing provides clinically significant reductions in blood pressure in both the supine and standing positions throughout the 24-hour interval. Due to the slow onset of action, acute hypotension is not a feature of amlodipine administration.
In patients with angina, once-daily administration of amlodipine increases total exercise time, time to angina onset, and time to 1 mm ST segment depression, and decreases both angina attack frequency and nitroglycerine tablet consumption.
Amlodipine has not been associated with any adverse metabolic effects or changes in plasma lipids and is suitable for use in patients with asthma, diabetes, and gout.
Treatment to Prevent Heart Attack Trial (ALLHAT): A randomized, double-blind, morbidity-mortality study called the Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT) was performed to compare newer drug therapies: amlodipine 2.5 mg/day to 10 mg/day (calcium channel blocker) or lisinopril 10 mg/day to 40 mg/day (ACE inhibitor) as first-line therapies to that of the thiazide-diuretic chlorthalidone 12.5 mg/day to 25 mg/day in mild to moderate hypertension.
A total of 33,357 hypertensive patients aged 55 or older were randomized and followed up for a mean of 4.9 years. The patients had at least one additional CHD risk factor, including MI or stroke for >6 months or documentation of other atherosclerotic CVD (overall 51.5%), type 2 diabetes (36.1%), high-density lipoprotein-C (HDL-C) <35 mg/dL (11.6%), left ventricular hypertrophy diagnosed by electrocardiogram or echocardiography (20.9%), or current cigarette smoking (21.9%).
The primary endpoint was a composite of fatal CHD or non-fatal MI. There was no significant difference in the primary endpoint between amlodipine-based therapy and chlorthalidone-based therapy: RR 0.98 95% CI [0.90-1.07], p = 0.65. In addition, there was no significant difference in all-cause mortality between amlodipine-based therapy and chlorthalidone-based therapy: RR 0.96 95% CI [0.89-1.02], p = 0.20.
Use in Patients with Heart Failure: Hemodynamic studies and exercise-based controlled clinical trials in NYHA Class II-IV heart failure patients have shown that amlodipine did not lead to clinical deterioration, as measured by exercise tolerance, left ventricular ejection fraction, and clinical symptomatology.
A placebo-controlled study (PRAISE) designed to evaluate patients in NYHA Class III-IV heart failure receiving digoxin, diuretics, and ACE inhibitors has shown that amlodipine did not lead to an increase in risk of mortality or combined mortality and morbidity in patients with heart failure.
In a follow-up, long-term, placebo-controlled study (PRAISE-2) of amlodipine in patients with NYHA class III and IV heart failure without clinical symptoms or objective findings suggestive of underlying ischemic disease, on stable doses of ACE inhibitors, digitalis, and diuretics, amlodipine had no effect on total or cardiovascular mortality. In this same population, amlodipine was associated with increased reports of pulmonary edema despite no significant difference in the incidence of worsening heart failure compared to placebo.
Use in Pediatric Patients (Aged 6 to 17 years): The efficacy of amlodipine in hypertensive pediatric patients aged 6 to 17 years of age was demonstrated in one 8-week, double-blind, placebo-controlled, randomized withdrawal trial in 268 patients with hypertension. All patients were randomized to the 2.5 mg or 5 mg treatment arms and followed up for 4 weeks after which they were randomized to continue 2.5 mg or 5 mg amlodipine or placebo for an additional 4 weeks.
Compared to baseline, once-daily treatment with amlodipine 5 mg resulted in statistically significant reductions in systolic and diastolic blood pressures. Placebo-adjusted mean reduction in seated systolic blood pressure was estimated to be 5.0 mmHg for the 5 mg dose of amlodipine and 3.3 mmHg for the 2.5 mg dose of amlodipine. Subgroup analyses indicated that younger pediatric patients aged 6 to 13 years had efficacy results comparable to those of the older pediatric patients aged 14 to 17 years.
Pharmacokinetics: Absorption: After oral administration of therapeutic doses, amlodipine is well absorbed with peak blood levels between 6 and 12 hours post-dose. Absolute bioavailability has been estimated to be between 64% and 80%. The volume of distribution is approximately 21 L/kg. Absorption of amlodipine is unaffected by consumption of food.
In vitro studies have shown that approximately 97.5% of circulating amlodipine is bound to plasma proteins.
Biotransformation/Elimination: The terminal plasma elimination half-life is about 35 to 50 hours and is consistent with once-daily dosing. Steady-state plasma levels are reached after 7 to 8 days of consecutive dosing. Amlodipine is extensively metabolized by the liver to inactive metabolites, with 10% of the parent compound and 60% of metabolites excreted in the urine.
Use in the Elderly: The time to reach peak plasma concentrations of amlodipine is similar in elderly and younger subjects. Amlodipine clearance tends to be decreased with resulting increases in AUC and elimination half-life in elderly patients. Increases in AUC and elimination half-life in patients with CHF were as expected for the patient age group studied.
Use in Pediatrics: In one clinical chronic exposure study, 73 hypertensive pediatric patients aged 12 months to less than or equal to 17 years received amlodipine at an average daily dose of 0.17 mg/kg. Clearance for subjects with median weight of 45 kg was 23.7 L/h and 17.6 L/h for males and females, respectively. This is in a similar range to the published estimates of 24.8 L/h in a 70 kg adult. The average estimate for volume of distribution for a 45 kg patient was 1130 L (25.11 L/kg). Maintenance of the blood pressure effect over the 24-hour dosing interval was observed with little difference in peak and trough variation effect. When compared to historical adult pharmacokinetics, the parameters observed in this study indicate that once-daily dosing is appropriate.
Toxicology: Preclinical Safety Data: Carcinogenesis, Mutagenesis, Impairment of Fertility: Rats and mice treated with amlodipine in the diet for 2 years, at concentrations calculated to provide daily dosage levels of 0.5, 1.25, and 2.5 mg/kg/day showed no evidence of carcinogenicity. The highest dose (for mice, similar to, and for rats twice* the maximum recommended clinical dose of 10 mg, on a mg/m2 basis) was close to the maximum tolerated dose for mice but not for rats.
Mutagenicity studies revealed no drug-related effects at either the gene or chromosome levels.
There was no effect on the fertility of rats treated with amlodipine (males for 64 days and females for 14 days prior to mating) at doses up to 10 mg/kg/day (8 times* the maximum recommended human dose of 10 mg, on a mg/m2 basis).
*Based on patient weight of 50 kg.
Hypertension: Amlodipine is indicated for the first-line treatment of hypertension and can be used as the sole agent to control blood pressure in the majority of patients. Patients not adequately controlled on a single antihypertensive agent (other than amlodipine) may benefit from the addition of amlodipine, which has been used in combination with a thiazide diuretic, alpha blockers, beta adrenoceptor blocking agent, or an angiotensin-converting enzyme (ACE) inhibitor.
Chronic Stable Angina: Amlodipine is indicated for the first-line treatment of myocardial ischemia, whether due to fixed obstruction (stable angina) and/or vasospasm/vasoconstriction (Prinzmetal's or variant angina) of coronary vasculature. Amlodipine may be used where the clinical presentation suggests a possible vasospastic/vasoconstrictive component but where vasospasm/vasoconstriction has not been confirmed. Amlodipine may be used alone, as monotherapy, or in combination with other antianginal drugs in patients with angina that is refractory to nitrates and/or adequate doses of beta-blockers.
For both hypertension and angina, the usual initial dose is 5 mg amlodipine once daily, which may be increased to a maximum dose of 10 mg depending on the individual patient's response.
No dose adjustment of amlodipine is required upon concomitant administration of thiazide diuretics, beta-blockers, and ACE inhibitors.
Use in the Elderly: Normal dosage regimens are recommended. Amlodipine, used at similar doses in the elderly or younger patients, is equally well tolerated.
Use in Children: Children and adolescents with hypertension from 6 years to 17 years of age. The recommended antihypertensive oral dose in pediatric patients aged 6-17 years is 2.5 mg once daily as a starting dose, up-titrated to 5 mg once daily if blood pressure goal is not achieved after 4 weeks. Doses in excess of 5 mg daily have not been studied in pediatric patients (see Pharmacology: Pharmacodynamics and Pharmacokinetics under Actions).
Children under 6 years old: No data are available.
Use in Patients with Impaired Hepatic Function: See Precautions.
Use in Patients with Renal Failure: Amlodipine may be used at normal doses in patients with renal failure. Changes in amlodipine plasma concentrations are not correlated with the degree of renal impairment. Amlodipine is not dialyzable.
Available data suggest that gross overdose could result in excessive peripheral vasodilatation and possibly reflex tachycardia. Marked and probably prolonged systemic hypotension, up to and including shock with fatal outcome, have been reported.
Administration of activated charcoal to healthy volunteers immediately after or up to 2 hours after amlodipine 10 mg ingestion has been shown to significantly decrease amlodipine absorption. Gastric lavage may be worthwhile in some cases. Clinically significant hypotension due to amlodipine overdose calls for active cardiovascular support, including frequent monitoring of cardiac and respiratory function, elevation of extremities, and attention to circulating fluid volume and urine output. A vasoconstrictor may be helpful in restoring vascular tone and blood pressure, provided there is no contraindication to its use. Intravenous calcium gluconate may be beneficial in reversing the effects of calcium channel blockade. Since amlodipine is highly protein-bound, dialysis is not likely to be of benefit.
Amlodipine is contraindicated in patients with a known hypersensitivity to dihydropyridines* or any of the inert ingredients.
*Amlodipine is a dihydropyridine calcium channel blocker.
Use in Patients with Heart Failure: In a long-term placebo-controlled study (PRAISE-2) of amlodipine in patients with New York Heart Association (NYHA) class III and IV heart failure of non-ischemic etiology, amlodipine was associated with increased reports of pulmonary edema despite no significant differences in the incidence of worsening heart failure compared to placebo (see Pharmacology: Pharmacodynamics under Actions).
Effects on Ability to Drive and Use Machines: Clinical experience with amlodipine indicates that it is unlikely to impair a patient's ability to drive or use machinery.
Use in Patients with Impaired Hepatic Function: As with all calcium antagonists, amlodipine's half-life is prolonged in patients with impaired liver function and dosage recommendations have not been established in these patients. The drug should therefore be administered with caution in these patients.
The safety of amlodipine in human pregnancy or lactation has not been established. Amlodipine does not demonstrate toxicity in animal reproductive studies other than delay in parturition and prolongation of labor in rats at a dose level 50 times the maximum recommended dose in humans. Accordingly, use in pregnancy is only recommended when there is no safer alternative and when the disease itself carries greater risk for the mother and fetus. There was no effect on the fertility of rats treated with amlodipine (see Pharmacology: Toxicology: Preclinical Safety Data under Actions).
Experience in humans indicates that amlodipine is transferred into human breast milk. The median amlodipine concentration ratio of milk/plasma in 31 lactating women with pregnancy-induced hypertension was 0.85 following amlodipine administration at an initial dose of 5 mg once daily which was adjusted as needed (mean daily dose and body weight adjusted daily dose: 6 mg and 98.7 mcg/kg, respectively). The estimated daily dose of amlodipine in the infant via breast milk was 4.17 mcg/kg.
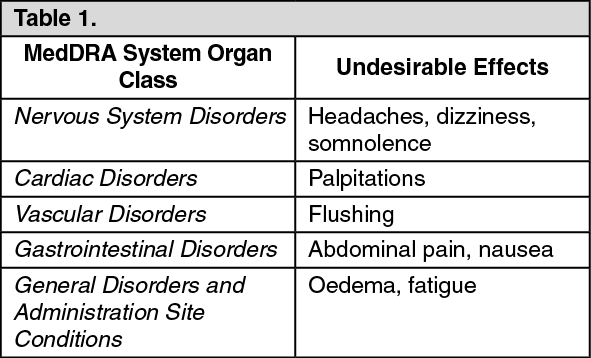
Amlodipine is well tolerated. In placebo-controlled clinical trials involving patients with hypertension or angina, the most commonly observed side effects were: (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
In these clinical trials, no pattern of clinically significant laboratory test abnormalities related to amlodipine has been observed.
Less commonly observed side effects in marketing experience include: (See Table 2.)
Click on icon to see table/diagram/image
Rarely reported events were allergic reactions including pruritus, rash, angioedema, and erythema multiforme.
Hepatitis, jaundice and hepatic enzyme elevations have also been reported very infrequently (mostly consistent with cholestasis). Some cases severe enough to require hospitalization have been reported in association with use of amlodipine. In many instances, causal association is uncertain.
As with other calcium channel blockers, the following adverse events have been rarely reported and cannot be distinguished from the natural history of the underlying disease: myocardial infarction, arrhythmia (including bradycardia, ventricular tachycardia and atrial fibrillation) and chest pain.
Pediatric Patients (ages 6-17 years): Amlodipine is well tolerated in children. Adverse events were similar to those seen in adults. In a study of 268 children, the most frequently reported adverse events were: (see Table 3).
Click on icon to see table/diagram/image
The majority of adverse events were mild or moderate. Severe adverse events (predominantly headache) were experienced by 7.2% with amlodipine 2.5 mg, 4.5% with amlodipine 5 mg, and 4.6% with placebo. The most common cause of discontinuation from the study was uncontrolled hypertension. There were no discontinuations due to laboratory abnormalities. There was no significant change in heart rate.
Amlodipine has been safely administered with thiazide diuretics, alpha blockers, beta-blockers, ACE inhibitors, long-acting nitrates, sublingual nitroglycerine, non-steroidal anti-inflammatory drugs, antibiotics, and oral hypoglycemic drugs.
In vitro data from studies with human plasma indicate that amlodipine has no effect on protein binding of the drugs tested (digoxin, phenytoin, warfarin, or indomethacin).
Simvastatin: Co-administration of multiple doses of 10 mg amlodipine with 80 mg simvastatin resulted in a 77% increase in exposure to simvastatin compared to simvastatin alone. Limit the dose of simvastatin in patients on amlodipine to 20 mg daily.
Grapefruit Juice: Co-administration of 240 mL grapefruit juice with a single oral dose of 10 mg amlodipine in 20 healthy volunteers had no significant effect on the pharmacokinetics of amlodipine. The study did not allow examination of the effect of genetic polymorphism in CYP3A4, the primary enzyme responsible for metabolism of amlodipine; therefore, administration of amlodipine with grapefruit or grapefruit juice is not recommended as bioavailability may be increased in some patients, resulting in increased blood pressure lowering effects.
CYP3A4 Inhibitors: Co-administration of a 180 mg daily dose of diltiazem with 5 mg amlodipine in elderly hypertensive patients (69 to 87 years of age) resulted in a 57% increase in amlodipine systemic exposure. Co-administration of erythromycin in healthy volunteers (18 to 43 years of age) did not significantly change amlodipine systemic exposure (22% increase in area under the concentration versus time curve [AUC]). Although the clinical relevance of these findings is uncertain, pharmacokinetic variations may be more pronounced in the elderly.
Strong inhibitors of CYP3A4 (e.g., ketoconazole, itraconazole, ritonavir) may increase the plasma concentrations of amlodipine to a greater extent than diltiazem. Amlodipine should be used with caution when administered with CYP3A4 inhibitors.
Clarithromycin: Clarithromycin is an inhibitor of CYP3A4. There is an increased risk of hypotension in patients receiving clarithromycin with amlodipine. Close observation of patients is recommended when amlodipine is co-administered with clarithromycin.
CYP3A4 Inducers: There is no data available regarding the effect of CYP3A4 inducers on amlodipine. Concomitant use of CYP3A4 inducers (e.g., rifampicin, Hypericum perforatum) may decrease the plasma concentrations of amlodipine. Amlodipine should be used with caution when administered with CYP3A4 inducers.
In the following studies, there were no significant changes in the pharmacokinetics of either amlodipine or another drug within the study, when co-administered.
Special Studies: Effect of Other Agents on Amlodipine: Cimetidine: Co-administration of amlodipine with cimetidine did not alter the pharmacokinetics of amlodipine.
Aluminum/Magnesium (Antacid): Co-administration of aluminum/magnesium (antacid) with a single dose of amlodipine had no significant effect on the pharmacokinetics of amlodipine.
Sildenafil: A single 100 mg dose of sildenafil in subjects with essential hypertension had no effect on the pharmacokinetic parameters of amlodipine. When amlodipine and sildenafil were used in combination, each agent independently exerted its own blood pressure lowering effect.
Special Studies: Effect of Amlodipine on Other Agents: Atorvastatin: Co-administration of multiple 10 mg doses of amlodipine with 80 mg atorvastatin resulted in no significant change in the steady-state pharmacokinetic parameters of atorvastatin.
Digoxin: Co-administration of amlodipine with digoxin did not change serum digoxin levels or digoxin renal clearance in healthy volunteers.
Ethanol (Alcohol): Single and multiple 10 mg doses of amlodipine had no significant effect on the pharmacokinetics of ethanol.
Warfarin: Co-administration of amlodipine with warfarin did not change the warfarin prothrombin response time.
Cyclosporin: No drug interaction studies have been conducted with cyclosporin and amlodipine in healthy volunteers or other populations, with the exception of renal transplant patients. Various studies in renal transplant patients report that co-administration of amlodipine with cyclosporin affects the trough concentrations of cyclosporin, from no change up to an average increase of 40%. Consideration should be given for monitoring cyclosporin levels in renal transplant patients on amlodipine.
Tacrolimus: There is a risk of increased tacrolimus blood levels when co-administered with amlodipine. In order to avoid toxicity of tacrolimus, administration of amlodipine in a patient treated with tacrolimus requires monitoring of tacrolimus blood levels and dose adjustment of tacrolimus when appropriate.
Mechanistic Target of Rapamycin (mTOR) Inhibitors: mTOR inhibitors such as sirolimus, temsirolimus, and everolimus are CYP3A substrates. Amlodipine is a weak CYP3A inhibitor. With concomitant use of mTOR inhibitors, amlodipine may increase exposure of mTOR inhibitors.
Drug/Laboratory Test Interactions: None known.
Incompatibilities: Not relevant.
Special Precautions for Disposal and Other Handling: Not relevant.
C08CA01 - amlodipine ; Belongs to the class of dihydropyridine derivative selective calcium-channel blockers with mainly vascular effects. Used in the treatment of cardiovascular diseases.
Norvasc tab 10 mg
100's;30's
Norvasc tab 5 mg
100's;30's





 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image


 Sign Out
Sign Out
