


 Sign Out
Sign Out

Summary of the safety profile: The safety profile of NINLARO is based on available clinical trial data and post-marketing experience to date. Frequencies of adverse reactions described as follows and in Table 6 have been determined based on data generated from clinical studies.
Unless otherwise noted, the data presented as follows is the pooled safety data from the pivotal, Phase 3, global C16010 study (n=720) and the double-blind, placebo-controlled C16010 China Continuation Study (n=115). The most frequently reported adverse reactions (≥ 20%) across 418 patients treated within the ixazomib regimen and 417 patients within the placebo regimen were diarrhoea (47% vs. 38%), thrombocytopenia (41% vs. 24%), neutropenia (37% vs. 36%), constipation (31% vs. 24%), upper respiratory tract infection (28% vs. 24%), peripheral neuropathy (28% vs. 22%), nausea (28% vs. 20%), back pain (25% vs. 21%), rash (25% vs. 15%), peripheral oedema (24% vs. 19%), vomiting (23% vs. 12%) and bronchitis (20% vs. 15%). Serious adverse reactions reported in ≥ 2% of patients included diarrhoea (3%), thrombocytopenia (2%) and bronchitis (2%).
Tabulated list of adverse reactions: The following convention is used for the classification of the frequency of an adverse drug reaction (ADR): very common (≥ 1/10); common (≥ 1/100 to < 1/10); uncommon (≥ 1/1,000 to < 1/100); rare (≥ 1/10,000 to < 1/1,000); very rare (< 1/10,000); not known (cannot be estimated from the available data). Within each system organ class, the ADRs are ranked by frequency, with the most frequent reactions first. Within each frequency grouping, adverse reactions are presented in order of decreasing seriousness. (See Table 6.)
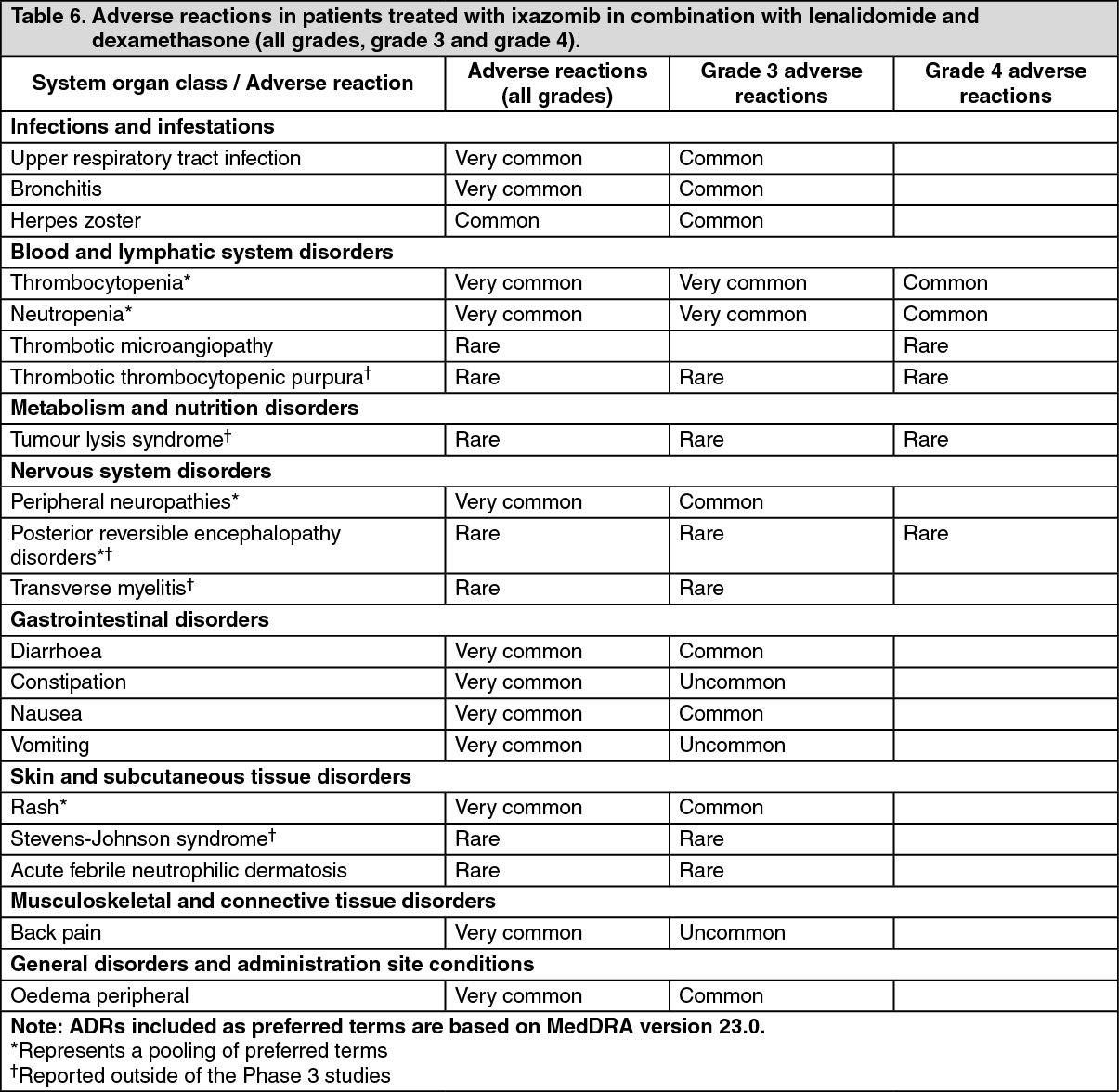 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageDescription of selected adverse reactions: Discontinuations: For each adverse reaction, one or more of the three medicinal products was discontinued in ≤ 3% of patients in the ixazomib regimen.
Thrombocytopenia: Two percent of patients in both the ixazomib regimen and the placebo regimen had a platelet count ≤ 10,000/mm3 during treatment. Less than 1% of patients in both regimens had a platelet count ≤ 5,000/mm3 during treatment. Thrombocytopenia resulted in discontinuation of one or more of the three medicinal products in 2% of patients in the ixazomib regimen and 3% of patients in the placebo regimen. Thrombocytopenia did not result in an increase in haemorrhagic events or platelet transfusions.
Gastrointestinal toxicities: Diarrhoea resulted in discontinuation of one or more of the three medicinal products in 2% of patients in the ixazomib regimen and 1% of patients in the placebo regimen.
Rash: Rash occurred in 25% of patients in the ixazomib regimen compared to 15% of patients in the placebo regimen. The most common type of rash reported in both regimens was maculo-papular and macular rash. Grade 3 rash was reported in 3% of patients in the ixazomib regimen compared to 2% of patients in the placebo regimen. Rash resulted in discontinuation of one or more of the three medicinal products in < 1% of patients in both regimens.
Peripheral neuropathy: Peripheral neuropathy occurred in 28% of patients in the ixazomib regimen compared to 22% of patients in the placebo regimen. Grade 3 adverse reactions of peripheral neuropathy were reported in 2% of patients in the ixazomib regimen compared to 1% in the placebo regimen. The most commonly reported reaction was peripheral sensory neuropathy (21% and 15% in the ixazomib and placebo regimen, respectively). Peripheral motor neuropathy was not commonly reported in either regimen (< 1%). Peripheral neuropathy resulted in discontinuation of one or more of the three medicinal products in 3% of patients in the ixazomib regimen compared to < 1% of patients in the placebo regimen.
Eye disorders: Eye disorders were reported with many different preferred terms but in aggregate, the frequency was 34% in patients in the ixazomib regimen and 28% of patients in the placebo regimen. The most common adverse reactions were blurred vision (6% in the ixazomib regimen and 5% in the placebo regimen), dry eye (6% in the ixazomib regimen and 1% in the placebo regimen), conjunctivitis (8% in the ixazomib regimen and 2% in the placebo regimen) and cataract (13% in the ixazomib regimen and 17% in the placebo regimen). Grade 3 adverse reactions were reported in 6% of patients in the ixazomib regimen and 8% of patients in the placebo regimen.
Other adverse reactions: In the pooled dataset from the pivotal, Phase 3, global C16010 study (n=720) and the double-blind, placebo-controlled, C16010 China Continuation Study (n=115), the following adverse reactions occurred with a similar rate between the ixazomib and placebo regimens: fatigue (28% vs. 26%), decreased appetite (13% vs. 11%), hypotension (5% vs. 4%), heart failure† (5% each), arrhythmia† (17% vs. 16%), and liver impairment including enzyme changes† (11% vs. 9%).
The frequency of severe (Grade 3-4) events of hypokalaemia was higher in the ixazomib regimen (7%) than the placebo regimen (2%).
Fungal and viral pneumonia resulting in fatal outcome were rarely reported in patients given the ixazomib, lenalidomide and dexamethasone combination.
† Standardised MedDRA Queries (SMQs)
Reporting of suspected adverse reactions: Reporting suspected adverse reactions after authorisation of the medicinal product is important. It allows continued monitoring of the benefit/risk balance of the medicinal product. Healthcare professionals are asked to report any suspected adverse reactions.
View ADR Monitoring Form