Pharmacology: Pharmacodynamics: Mechanism of action: Paracetamol: Although the exact site and mechanism of analgesic action is not clearly defined, paracetamol appears to produce analgesia by elevation of the pain threshold.
Ibuprofen: Ibuprofen possesses analgesic, antipyretic and anti-inflammatory properties, similar to other non-steroidal anti-inflammatory drugs (NSAIDs). Its mechanism of action is unknown, but is thought to be through peripheral inhibition of cyclooxygenases and subsequent prostaglandin synthesis inhibition.
Clinical Trials: A prospective, Parallel Group, Double-Blind Comparison of the Analgesic Effect of Maxigesic, Paracetamol alone, or Ibuprofen alone in 135 Patients with Post-Operative dental pain for 48 hours following oral surgery was conducted. The oral surgery was conducted under local or general anaesthetic with one dose of oral analgesic (2 tablets of paracetamol 500mg or ibuprofen 300mg or Maxigesic ) given pre-operatively. Total dose in the 24 hours were paracetamol 4000mg, ibuprofen 1200mg and Maxigesic. Analgesia, the primary efficacy end point was a time-corrected AUC (Area under the Curve) calculated from 100mm VAS (Visual Analogue Scale) pain scores over 48 hours at both rest and on activity.
The primary end points, assessed on the Intent to Treat (ITT) population, showed the mean time-adjusted AUCs over 48 hours calculated from the VAS pain scores for Maxigesic were significantly lower than for paracetamol at rest (22.344 [SE 3.2] and 33.016 [3.005] respectively (p=0.007), and on activity 28.377 [SE 3.396] and 40.364 [SE 3.271] respectively (p=0.006).
A similar outcome is seen for the Maxigesic comparison where the AUCs over 48 hours showed the VAS for the combination drug were significantly lower than for ibuprofen at rest, 22.344 [SE 3.2] and 34.78 [SE 3.22] respectively (p=0.003) and during activity, 28.377 [SE 3.396] and 40.217 [SE 3.418] respectively (p=0.007). (See Figure 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
A presentation of the pain records during the 48 hours also shows the Maxigesic analgesic effect showed lower mean pain scores than either of its two active ingredients at almost all time points at both rest and during activity (see Figure 2).
Click on icon to see table/diagram/image
Pharmacokinetics: Absorption: Paracetamol is absorbed from the gastrointestinal tract with peak plasma concentration occurring about 10 to 60 minutes after oral administration.
Ibuprofen is absorbed following oral administration with maximum plasma concentrations usually achieved in 60 to 120 minutes.
Distribution: Paracetamol is distributed into most body tissues. Ibuprofen is highly protein bound.
Metabolism: Paracetamol is metabolised extensively in the liver and excreted in the urine, mainly as inactive glucuronide and sulphate conjugates. Less that 5% is excreted unchanged. The metabolites of paracetamol include a minor hydroxylated intermediate which has hepatotoxic activity. This active intermediate is detoxified by conjugation with glutathione, however, it can accumulate following paracetamol overdosage and if left untreated has the potential to cause severe and even irreversible liver damage.
Paracetamol is metabolised differently by premature infants, newborns, and young children compared with adults, the sulphate conjugate being most predominant.
Ibuprofen is highly bound (90-99%) to plasma proteins and is extensively metabolised to inactive compounds in the liver, mainly by glucuronidation.
The metabolic pathways of paracetamol and ibuprofen are distinct and there should be no drug interactions where the metabolism of one affects the metabolism of the other. A formal study using human liver enzymes to investigate such a possibility failed to find any potential drug interaction on the metabolic pathways.
In another study, the effect of ibuprofen on the oxidative metabolism of paracetamol was evaluated in healthy volunteers under fasting conditions. The study results indicated that ibuprofen did not alter the amount of paracetamol undergoing oxidative metabolism, as the amount of paracetamol and its metabolites (glutathione-, mercapturate-, cysteine-, glucuronide- and sulfate-paracetamol) were similar when administered alone, as paracetamol, or with the concomitant administration of ibuprofen (as a fixed combination Maxigesic).
Elimination: Paracetamol elimination half-life varies from about 1 to 3 hours.
Both the inactive metabolites and a small amount of unchanged ibuprofen are excreted rapidly and completely by the kidney, with 95% of the administered dose eliminated in the urine within four hours of ingestion. The elimination half-life if ibuprofen is in the range of 1.9 to 2.2 hours.
Pharmacokinetic/pharmacodynamic relationship(s): A specific study to investigate possible effects of paracetamol on the plasma clearance of ibuprofen and vice versa did not identify any drug interactions.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image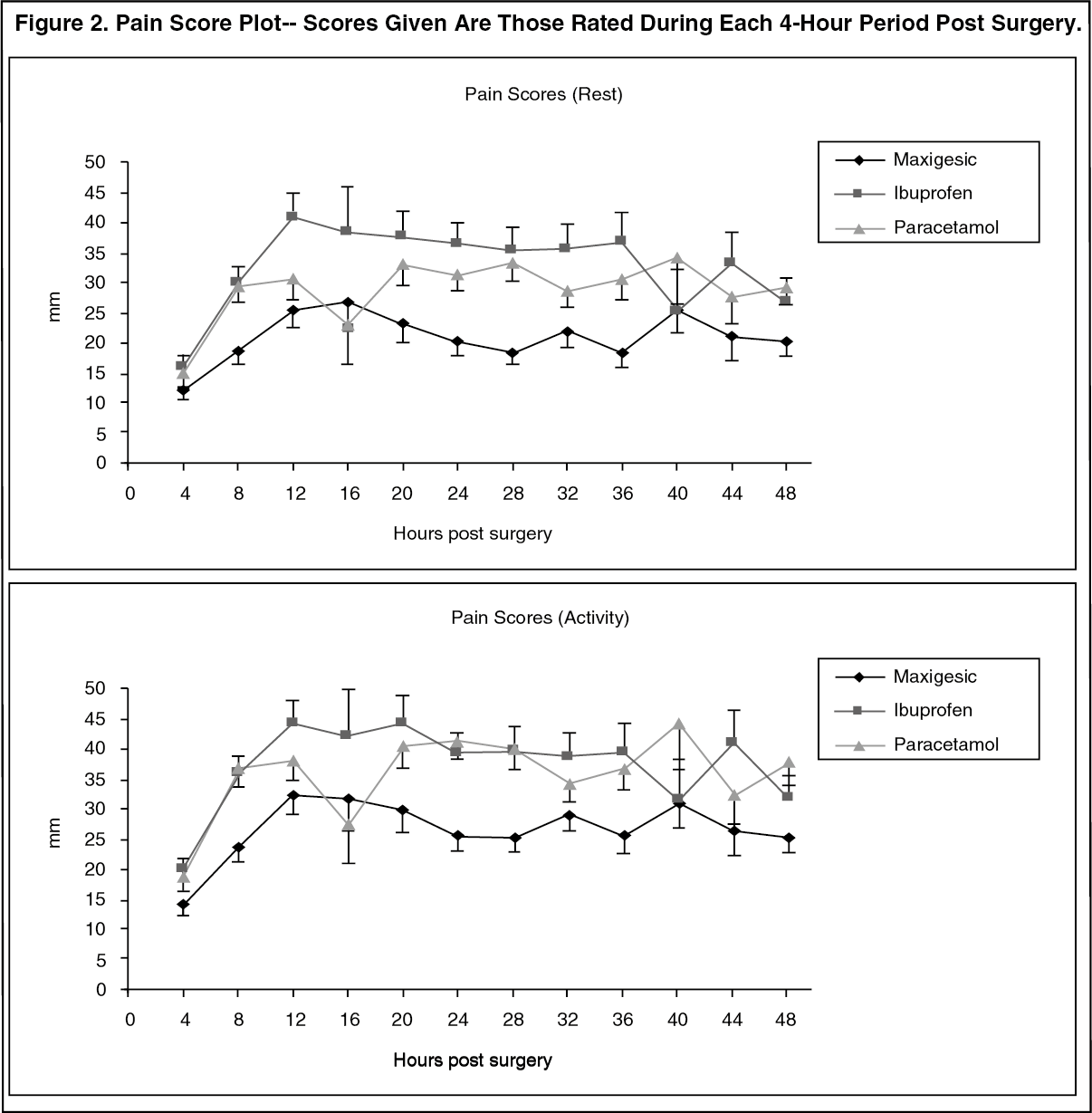 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out
