


 Sign Out
Sign Out




Clinically Significant Adverse Reactions: Hypoglycemia (1.0%*): Hypoglycemia may occur in combined use with other antidiabetic drugs (in particular, sulfonylureas or insulin preparations). In addition, hypoglycemia was reported without combined use of other antidiabetic drugs. When hypoglycemic symptoms are observed, appropriate measures such as eating food containing carbohydrates should be taken. However, when hypoglycemic symptoms are observed in combined use with α-glucosidase inhibitors, glucose should be administered. (See Special Precautions for Use, Important Precautions under Precautions, Interactions and Pharmacology: Clinical Studies under Actions).
*: The Incidence calculated from the results of clinical studies (monotherapy), at the time of approval in Japan.
Pyelonephritis (0.1%), sepsis (incidence unknown): Since pyelonephritis may occur and result in sepsis (including septic shock), patients should be closely monitored. If any abnormality is noted, administration should be discontinued and appropriate treatment should be provided. (See Important Precautions under Precautions).
Necrotising fasciitis of the perineum (Fournier's gangrene) (incidence unknown): Post-marketing cases of necrotising fasciitis of the perineum, (also known as Fournier's gangrene), have been reported in female and male patients taking SGLT2 inhibitors. This is a rare but serious and potentially life-threatening event that requires urgent surgical intervention and antibiotic treatment. Patients should be advised to seek medical attention if they experience a combination of symptoms of pain, tenderness, erythema, or swelling in the genital or perineal area, with fever or malaise. Be aware that either urogenital infection or perineal abscess may precede necrotizing fasciitis. If Fournier's gangrene is suspected, Lusefi should be discontinued and prompt treatment (including antibiotics and surgical debridement) should be instituted. (See Important Precautions under Precautions).
Dehydration (0.1%): Dehydration may occur. Patients should be instructed to drink fluid appropriately and be monitored sufficiently. When symptoms including thirst, polyuria, pollakiuria and blood pressure decreased appear and dehydration is suspected, appropriate measures including interruption of administration and fluid replacement should be taken. Since onset of thromboembolism such as cerebral infarction following dehydration has been reported, sufficient attention should be paid. (See Special Precautions for Use and Important Precautions under Precautions.)
Ketoacidosis (incidence unknown): Since ketoacidosis (including diabetic ketoacidosis) may occur, patients should be closely monitored. If any abnormality is noted, administration should be discontinued and appropriate treatment should be provided. (See Important Precautions under Precautions.)
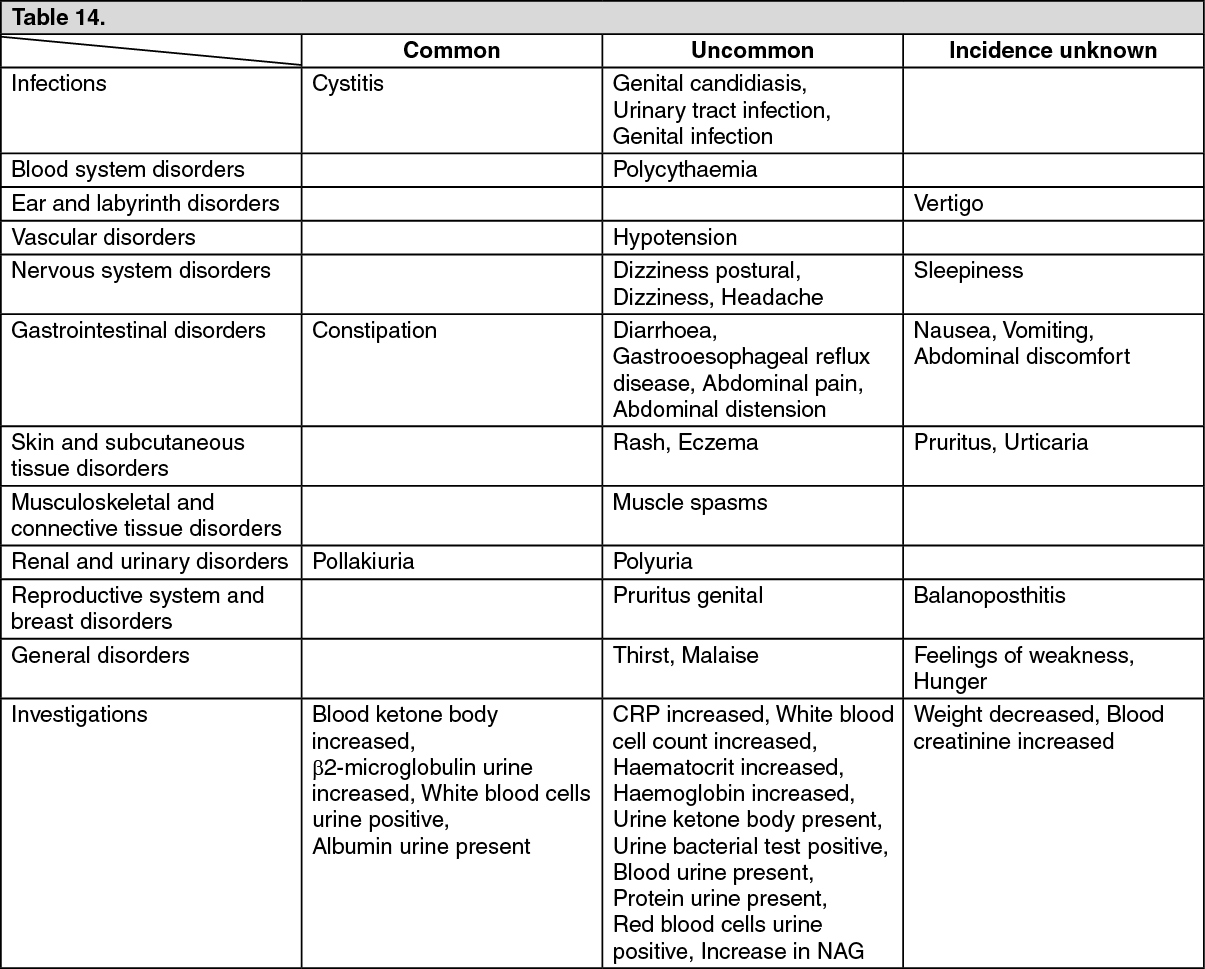
Other Adverse Reactions: The following adverse reactions have been reported in all the clinical trials and from post-marketing experience with luseogliflozin. Adverse reactions listed as follows are classified according to frequency and system organ class (SOC). Frequency categories are defined according to the following convention: very common (≥ 1/10), common (≥ 1/100 to < 1/10), uncommon (≥ 1/1,000 to < 1/100), rare (≥1/10,000 to < 1/1,000), very rare (< 1/10,000) and not known (cannot be estimated from the available data). (See Table 14.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
View ADR Monitoring Form