Pharmacology: Pharmacodynamics: Mechanism of action: Esflurbiprofen is an optical isomer (S isomer) of flurbiprofen, racemate.
An
in vitro study demonstrated the inhibitory action of esflurbiprofen on the cyclooxygenase activity, which is probably the main source of anti-inflammatory/analgesic effects.
Pharmacodynamic effects: Analgesic effect: The analgesic effect was demonstrated in all pain models: a dog model of urate-induced knee joint arthritic pain, and rat models of carrageenan-induced inflammatory pain, silver nitrate-induced arthritic pain, and adjuvant-induced arthritic pain.
Anti-inflammatory effect: The anti-inflammatory effect was demonstrated in all acute inflammation models: rat models of carrageenan-induced footpad inflammation, traumatic oedema, and adjuvant-induced arthritis.
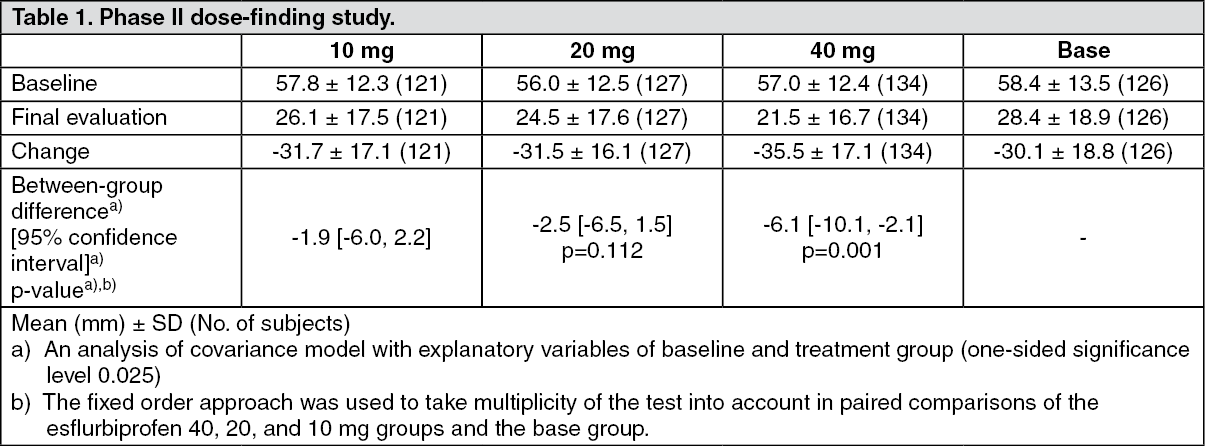
Clinical efficacy and safety: A randomized double-blind, placebo-controlled, parallel-group study (phase II dose-finding study) and a randomized open-label* parallel-group study with flurbiprofen patches as the control (phase III study) were performed in patients with knee osteoarthritis. The following tables show changes from baseline in VAS scores (pain felt on rising from the chair) in patients receiving esflurbiprofen 40mg, base, or flurbiprofen patches for 2 weeks.
*The study was performed with well managed information on treatment groups for study subjects and investigators.
(See Tables 1 and 2.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Pharmacokinetics: Plasma Levels:
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Pharmacokinetics: Plasma Levels: Single dose: The pharmacokinetic parameters and changes in plasma concentrations in healthy adults (Japanese) receiving a single 24-hour application of 40mg of esflurbiprofen are shown in Table 3 and figure. Based on the residual drug amount in the patch, the transdermal absorption was calculated to be 48.34 ± 16.70%. (See Table 3 and figure.)
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Multiple doses: The pharmacokinetic parameters in healthy adults (Japanese) receiving multiple 23-hour applications of once daily doses of 80 mg of esflurbiprofen for 7 days are shown in Table 4. Based on the residual drug amount in the patch, the transdermal absorption was calculated to be 73.24 ± 11.58%. (See Table 4.)
Click on icon to see table/diagram/image
Distribution: Tissue penetration: In patients (Japanese) with knee osteoarthritis scheduled to undergo knee replacement arthroplasty, the levels of esflurbiprofen in the synovia, synovial fluid, and plasma after a single 12-hour application of 20 mg of esflurbiprofen were 14.8, 32.7, and 34.5 times higher, respectively, than those after the use of 40 mg flurbiprofen patch.
Protein binding: An
in vitro study showed that 99.95% of esflurbiprofen was bound to human plasma protein, probably to albumin as the main binding protein.
Metabolism: Esflurbiprofen mainly undergoes oxidative metabolism by CYP2C9. A study investigating the effect of CYP2C9 polymorphism using human liver microsomes showed the 4'-hydroxylation activity (CL
int) in poor metabolizers (PMs) (with genotype CYP2C9*3/*3) was 1/69 of that in extensive metabolizers (EMs) (with genotype CYP2C9*1/*1).
Excretion: In healthy adults (Japanese) receiving a single 24-hour application of 80 mg of esflurbiprofen, little of the dose (0.253%) was excreted as unchanged compound in the urine through 72 hours after the start of application.
Major metabolites were glucuronate or sulfate conjugates of the 4'-hydroxy compound. Other metabolites were free glucuronate conjugates, 4'-hydroxy compounds, and glucuronate conjugates of the 3'-hydroxy-4'-methoxy compound.
Toxicology: Preclinical safety data: Non-clinical data reveal no special hazard for humans based on conventional studies of safety pharmacology, repeated dose toxicity, genotoxicity, carcinogenic potential, fertility and early development, and embryo-fetal development.
In the pre- and postnatal development study using rats in late pregnancy, maternal animal death at ≥ 0.1 mg/kg, a tendency of an increased number and percentage of stillborn pups at 0.1, 0.3, and 3 mg/kg, delayed delivery at 0.3 mg/kg, reduced live birth index at ≥ 0.3 mg/kg, and incomplete delivery and prolonged delivery at ≥ 1 mg/kg were indicated. Since the AUC
0-24h value of esflurbiprofen on Day 17 of gestation at 1 mg/kg was comparable or less than the exposure after 40 or 80 mg of esflurbiprofen was administered to humans, the AUC
0-24h values at 0.1 and 0.3 mg/kg appeared to be lower than that in humans.
After esflurbiprofen was administered to rats in the lactation period, suppression of postnatal body weight gain and delayed onset of early behavior were seen at 3 mg/kg. The AUC
0-24h value of esflurbiprofen on Day 17 of gestation at 3 mg/kg were 5.77 and 2.55 times higher than the exposure after 40 or 80 mg of esflurbiprofen was administered to humans.





 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image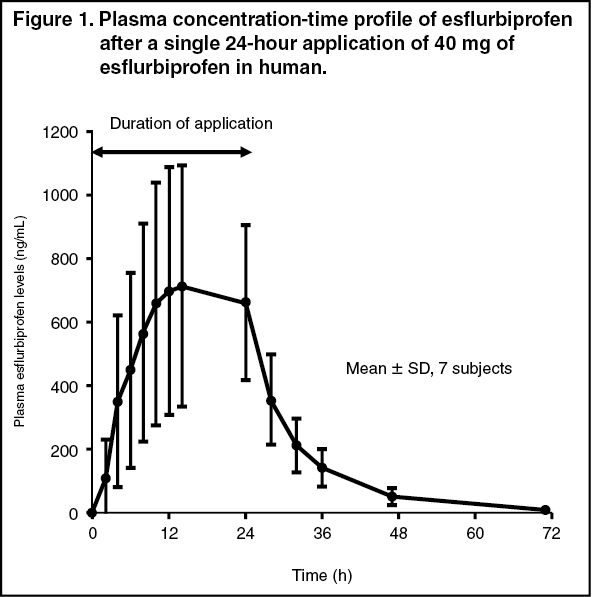 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out
