


 Sign Out
Sign Out



Agents that may increase ibrutinib plasma concentrations: Concomitant use of IMBRUVICA and medicinal products that strongly or moderately inhibit CYP3A4 can increase ibrutinib exposure and strong CYP3A4 inhibitors should be avoided.
Strong CYP3A inhibitors: Co-administration of ketoconazole, a strong CYP3A inhibitor, in 18 healthy subjects, increased exposure (Cmax and AUC0-last) of ibrutinib by 29- and 24-fold, respectively. In a dedicated drug-drug interaction study in patients with B-cell malignancies, co-administration of voriconazole increased Cmax and AUC by 6.7-fold and 5.7-fold, respectively. In clinical studies, the maximal observed ibrutinib exposure (AUC) was ≤ 2-fold in 37 patients treated with mild and/or moderate CYP3A inhibitors when compared with the ibrutinib exposure in 76 patients not treated concomitantly with CYP3A inhibitors. Clinical safety data in 66 patients treated with moderate (n=47) or strong CYP3A inhibitors (n=19) did not reveal meaningful increases in toxicities. Voriconazole and posaconazole can be used concomitantly with IMBRUVICA as per dose recommendations in the table as follows. All other strong inhibitors of CYP3A (e.g., ketoconazole, indinavir, nelfinavir, ritonavir, saquinavir, clarithromycin, telithromycin, itraconazole, nefazodone, and cobicistat) should be avoided and an alternative with less CYP3A inhibitory potential should be considered. If the benefit outweighs the risk and a strong CYP3A inhibitor must be used, see recommended dose modifications in the table as follows.
Moderate and mild CYP3A inhibitors: In patients with B-cell malignancies, co-administration of CYP3A inhibitor erythromycin increased Cmax and AUC by 3.4-fold and 3.0-fold, respectively. If a moderate CYP3A inhibitor (e.g., fluconazole, erythromycin, amprenavir, aprepitant, atazanavir, ciprofloxacin, crizotinib, diltiazem, fosamprenavir, imatinib, verapamil, amiodarone, dronedarone) is indicated, reduce IMBRUVICA dose as per recommended dose modifications in the table as follows.
No dose adjustment is required in combination with mild inhibitors. Monitor patient closely for toxicity and follow dose modification guidance as needed. Avoid grapefruit and Seville oranges during IMBRUVICA treatment as these contain moderate inhibitors of CYP3A (see Dosage & Administration and Pharmacology: Pharmacokinetics under Actions).
Recommended dose modifications are described as follows: (See Table 17.)
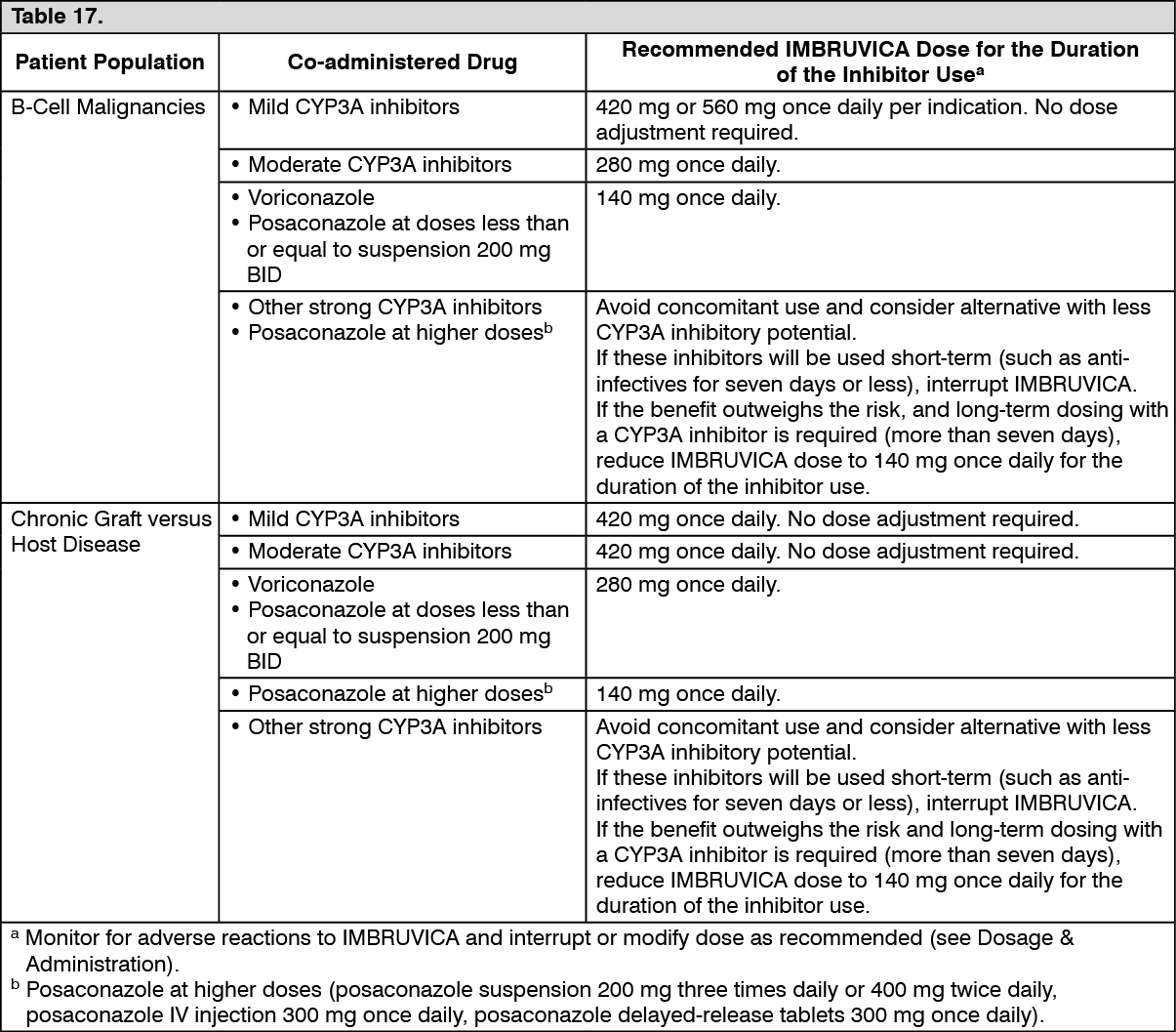 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageAfter discontinuation of a CYP3A inhibitor, resume previous dose of IMBRUVICA (see Dosage & Administration).
Agents that may decrease ibrutinib plasma concentrations: Administration of IMBRUVICA with inducers of CYP3A4 can decrease ibrutinib plasma concentrations.
Co-administration of rifampicin, a strong CYP3A4 inducer, in 18 fasted healthy subjects, decreased exposure (Cmax and AUC) of ibrutinib by 92 and 90%, respectively. Avoid concomitant use of strong or moderate CYP3A4 inducers (e.g., carbamazepine, rifampicin, phenytoin). Preparations containing St. John's Wort are contraindicated during treatment with IMBRUVICA, as efficacy may be reduced. Consider alternative agents with less CYP3A4 induction. If the benefit outweighs the risk and a strong or moderate CYP3A4 inducer must be used, monitor patient closely for lack of efficacy (see Contraindications and Precautions). Mild inducers may be used concomitantly with IMBRUVICA, however, patients should be monitored for potential lack of efficacy.
Ibrutinib has a pH dependent solubility, with lower solubility at higher pH. A lower Cmax was observed in fasted healthy subjects administered a single 560 mg dose of ibrutinib after taking omeprazole at 40 mg once daily for 5 days (see Pharmacology: Pharmacokinetics under Actions). There is no evidence that the lower Cmax would have clinical significance, and medicinal products that increase stomach pH (e.g., proton pump inhibitors) have been used without restrictions in the pivotal clinical studies.
Agents that may have their plasma concentrations altered by ibrutinib: Ibrutinib is a P-gp and breast cancer resistance protein (BCRP) inhibitor in vitro. As no clinical data are available on this interaction, it cannot be excluded that ibrutinib could inhibit intestinal P-gp and BCRP after a therapeutic dose. To minimise the potential for an interaction in the GI tract, oral narrow therapeutic range, P-gp or BCRP substrates such as digoxin or methotrexate should be taken at least 6 hours before or after IMBRUVICA. Ibrutinib may also inhibit BCRP in the liver and increase the exposure of medicinal products that undergo BCRP-mediated hepatic efflux, such as rosuvastatin.
In a drug interaction study in patients with B-cell malignancies, a single 560 mg dose of ibrutinib did not have a clinically meaningful effect on the exposure of the CYP3A4 substrate midazolam. In the same study, 2 weeks of treatment with ibrutinib at 560 mg daily had no clinically relevant effect on the pharmacokinetics of oral contraceptives (ethinylestradiol and levonorgestrel), the CYP3A4 substrate midazolam, nor the CYP2B6 substrate bupropion.