Metformin hydrochloride, glibenclamide.
Each film-coated tablet contains 500 mg metformin hydrochloride, equivalent to 390 mg metformin, and 2.5 mg glibenclamide.
Each film-coated tablet contains 500 mg metformin hydrochloride, equivalent to 390 mg metformin, and 5 mg glibenclamide.
Excipient: Contains lactose, see Precautions.
Excipients/Inactive Ingredients: Tablet core: Microcrystalline cellulose, Sodium croscarmellose, Povidone K30, Magnesium stearate.
Film-coating: Glucovance 500mg/2.5 mg: Opadry OY-L-24808 (orange) (lactose monohydrate, hypromellose, titanium dioxide (E171), macrogol, yellow iron oxide (E172), red iron oxide (E172), black iron oxide (E172).
Glucovance 500mg/5 mg: Opadry 31-F-22700 (yellow) (lactose monohydrate, hypromellose, titanium dioxide (E171), macrogol, yellow iron oxide (E172), red iron oxide (E172), Quinoline Yellow Lake (E104).
Pharmacotherapeutic group: Biguanides and sulphonamide(s) in combination. ATC code: A10BD02.
Pharmacology: Pharmacodynamics: Metformin is a biguanide with antihyperglycaemic effects, lowering both basal and postprandial plasma glucose. It does not stimulate insulin secretion and therefore does not produce hypoglycaemia.
Metformin may act via 3 mechanisms: (1) by reducing hepatic glucose production by inhibiting gluconeogenesis and glycogenolysis; (2) in muscle, by increasing insulin sensitivity, improving peripheral glucose uptake and utilisation; (3) and by delaying intestinal glucose absorption.
Metformin stimulates intracellular glycogen synthesis by acting on glycogen synthase. Metformin increases the transport capacity of all types of membrane glucose transporters (GLUT).
In humans, independently of its action on glycaemia, metformin has favourable effects on lipid metabolism. This has been shown at therapeutic doses in controlled, medium-term or long-term clinical studies: metformin reduces total cholesterol, LDL-cholesterol and triglyceride levels. In clinical trials conducted so far with combination therapy with metformin and glibenclamide, these favourable effects on lipid metabolism have not been shown.
Glibenclamide is a second generation sulphonylurea with a medium half-life: it causes acute lowering of blood glucose by stimulating the release of insulin by the pancreas, this effect being dependent on the presence of functioning beta cells in the islets of Langerhans.
The stimulation of insulin secretion by glibenclamide in response to a meal is of major importance.
The administration of glibenclamide to diabetics induces an increase in the postprandial insulin-stimulating response. The increased postprandial responses in insulin and C-peptide secretion persist after at least 6 months of treatment.
Metformin and glibenclamide have different mechanisms and sites of action, but their action is complementary. Glibenclamide stimulates the pancreas to secrete insulin, while metformin reduces cell resistance to insulin by acting on peripheral (skeletal muscle) and hepatic sensitivity to insulin.
Results from controlled, double blind clinical trials versus reference products in the treatment of type 2 diabetes inadequately controlled by monotherapy with metformin or glibenclamide combined with diet and exercise, have demonstrated that the combination had an additive effect on glucose regulation.
Paediatric patients: In a 26-week, active controlled, double-blind, clinical study performed in 167 paediatric patients aged 9 to 16 years with type 2 diabetes not adequately controlled with diet and exercise, with or without an oral antidiabetic treatment, a fixed combination of metformin hydrochloride 250 mg and glibenclamide 1.25 mg was not shown more effective to either metformin hydrochloride or glibenclamide in reducing HbA1c from baseline. Therefore, Glucovance should not be used in paediatric patients.
Pharmacokinetics: Related to the combination: The bioavailability of metformin and glibenclamide in the combination is similar to that noted when one tablet of metformin and one tablet of glibenclamide are taken simultaneously. The bioavailability of metformin in the combination is unaffected by the ingestion of food. The bioavailability of glibenclamide in the combination is unaffected by the ingestion of food, but the absorption speed of glibenclamide is increased by eating.
Related to metformin: Absorption: After an oral dose of metformin, maximum plasma concentration (Cmax) is reached in approximately 2.5 hours (tmax). Absolute bioavailability of a 500 mg or 850 mg metformin tablet is approximately 50-60% in healthy subjects. After an oral dose, the non-absorbed fraction recovered in faeces was 20-30%.
After oral administration, metformin absorption is saturable and incomplete. It is assumed that the pharmacokinetics of metformin absorption is non-linear. At the usual metformin doses and dosing schedules, steady state plasma concentrations are reached within 24 to 48 hours and are generally less than 1 μg/ml. In controlled clinical trials, maximum metformin plasma levels (Cmax) did not exceed 4 μg/ml, even at maximum doses.
Distribution: Plasma protein binding is negligible. Metformin partitions into erythrocytes. The blood peak is lower than the plasma peak and appears at approximately the same time. The red blood cells most likely represent a secondary compartment of distribution. The mean volume of distribution Vd ranged from 63 to 276 l.
Metabolism: Metformin is excreted unchanged in the urine. No metabolites have been identified in humans.
Biotransformation: Metformin is excreted unchanged in the urine. No metabolites have been identified in humans.
Elimination: Renal clearance of metformin is > 400 ml/min, indicating that metformin is eliminated by glomerular filtration and tubular secretion. Following an oral dose, the apparent terminal elimination half-life is approximately 6.5 hours.
When renal function is impaired, renal clearance is decreased in proportion to that of creatinine and thus the elimination half-life is prolonged, leading to increased levels of metformin in plasma.
Related to glibenclamide: Absorption: Glibenclamide is very readily absorbed (> 95%) following oral administration. The peak plasma concentration is reached in about 4 hours.
Distribution: Glibenclamide is extensively bound to plasma albumin (99%), which may account for certain drug interactions.
Metabolism: Glibenclamide is completely metabolised in the liver to two metabolites. Hepatocellular failure decreases glibenclamide metabolism and appreciably slows down its excretion.
Elimination: Glibenclamide is excreted in the form of metabolites via biliary route (60%) and urine (40%), elimination being complete within 45 to 72 hours. Its terminal elimination half-life is 4 to 11 hours.
Biliary excretion of the metabolites increases in cases of renal insufficiency, according to the severity of renal impairment until a creatinine clearance at 30 ml/min. Thus, glibenclamide elimination is unaffected by renal insufficiency as long as the creatinine clearance remains above 30 ml/min.
Paediatric patients: There were no differences in pharmacokinetics of glibenclamide and metformin between paediatric patients and weight- and gender-matched healthy adults.
Toxicology: Preclinical safety data: No preclinical studies have been performed on the combination product. Preclinical evaluation of the constituents metformin and glibenclamide revealed no special hazard for humans based on conventional studies of repeated dose toxicity, genotoxicity and carcinogenic potential.
Animal studies on metformin and glibenclamide do not indicate direct or indirect harmful effects with respect to pregnancy, embryonal/foetal development, parturition or postnatal development (see Use in Pregnancy & Lactation).
Glucovance is indicated as second-line therapy when diet, exercise, and initial treatment with a sulphonylurea or metformin do not result in adequate glycaemic control in patients with type 2 diabetes.
ROUTE OF ADMINISTRATION: Oral.
General Consideration: Dosage of Glucovance must be individualized on the basis of both effectiveness and tolerance while not exceeding the maximum recommended daily dose of 2000 mg metformin/20 mg glibenclamide. Glucovance should be given with meals with a sufficiently high carbohydrate content to prevent the onset of hypoglycaemic episode. Glucovance should be initiated at a low dose, with gradual dose escalation described as follows, in order to avoid hypoglycaemia (largely due to glibenclamide), to reduce GI side effects (largely due to metformin), and to permit determination of the minimum effective dose for adequate control of blood glucose for the individual patient.
With initial treatment and during dose titration, appropriate blood glucose monitoring should be used to determine the therapeutic response to Glucovance and to identify the minimum effective dose for the patient. Thereafter, HbA
1c (glycosylated haemoglobin) should be measured at intervals of approximately 3 months to assess the effectiveness of therapy. The therapeutic goal in all patients with type 2 diabetes is to decrease FPG, PPG, and HbA
1c, to normal or as near normal as possible. Ideally, the response to therapy should be evaluated using HbA
1c which is a better indicator of long-term glycaemic control than FPR alone.
No studies have been performed specifically examining the safety and efficacy of switching of Glucovance therapy in patients taking concomitant glibenclamide (or other sulphonylurea) plus metformin. Changes in glycaemic control may occur in such patients, with either hyperglycaemia or hypoglycaemia possible. Any change in therapy of type 2 diabetes should be undertaken with care and appropriate monitoring.
When Glucovance is co-administered with colesevelam, it is recommended that Glucovance should be administered at least 4 hours prior to colesevelam in order to minimize the risk of reduced absorption.
Glucovance Use in Previously Treated Patients (Second-Line Therapy): Recommended starting dose: 500/2.5 mg or 500/5 mg twice daily with meals.
For patients not adequately controlled on either glibenclamide (or another sulphonylurea) or metformin alone, the recommended starting dose of Glucovance is 500/2.5 mg or 500/5 mg twice daily with the morning and evening meals. In order to avoid hypoglycaemia, the starting dose of Glucovance should not exceed the daily doses of glibenclamide or metformin already being taken. The daily dose should be titrated in increments of no more than 500/5 mg up to the minimum effective dose to achieve adequate control of blood glucose or to a maximum dose of 2000 mg/20 mg per day.
For patients previously treated with combination therapy of glibenclamide (or another sulphonylurea) plus metformin, if switched to Glucovance, the starting dose should not exceed the daily dose of glibenclamide (or equivalent dose of another sulphonylurea) and metformin already being taken. Patients should be monitored closely for signs and symptoms of hypoglycaemia following such a switch and the dose of Glucovance should be titrated as described previously to achieve adequate control of blood glucose.
The tablets should be taken with meals. The dosage regimen should be adjusted according to the individual eating habits. However, any intake must be followed by a meal with a sufficiently high carbohydrate content to prevent the onset of hypoglycaemic episodes.
When Glucovance is co-administered with a bile acid sequestrant, it is recommended that Glucovance should be administered at least 4 hours prior to the bile acid sequestrant in order to minimize the risk of reduced absorption (see Interactions).
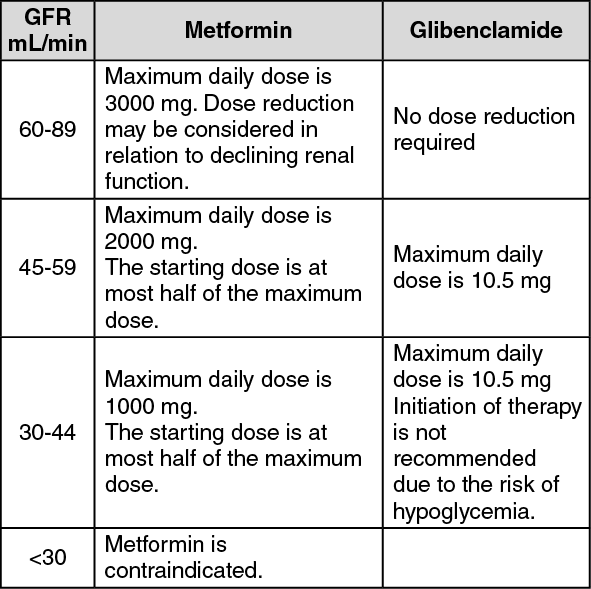
Renal Impairment: A GFR should be assessed before initiation of treatment with metformin containing products and at least annually thereafter. In patients at an increased risk of further progression of renal impairment and in the elderly, renal function should be assessed more frequently, e.g. every 3-6 months. The maximum daily dose of metformin should preferably be divided into 2-3 daily doses. Factors that may increase the risk of lactic acidosis should be reviewed before considering initiation of metformin in patients with GFR <60 ml/min. If no adequate strength of Glucovance is available, individual monocomponents should be used instead of the fixed dose combination. (See table.)
 Click on icon to see table/diagram/image
Geriatric population:
Click on icon to see table/diagram/image
Geriatric population: The dosage of Glucovance should be adjusted depending on renal function parameters (start with 1 tablet of Glucovance 500 mg/2.5 mg); regular checks on the renal function are necessary (see Precautions).
Patients aged 65 years and older: starting and maintenance doses of glibenclamide must be carefully adjusted to reduce the risk of hypoglycaemia. Treatment should be started with the lowest available dose and increased gradually if necessary (see Precautions).
Paediatric population: Glucovance is not recommended for use in children (see Pharmacology: Pharmacodynamics under Actions).
Overdose may precipitate hypoglycaemia due to the presence of the sulphonylurea (see Precautions).
High overdose or the existence of concomitant risk factors may lead to lactic acidosis due to the presence of metformin (see Precautions). Lactic acidosis is a medical emergency and must be treated in hospital. The most effective treatment is to remove lactate and metformin by haemodialysis.
The plasma clearance of glibenclamide may be prolonged in patients suffering from liver disease. Since glibenclamide is extensively bound to proteins, it is not eliminated by dialysis.
This medicinal product must never be used in case of: hypersensitivity to metformin hydrochloride, glibenclamide or other sulphonylurea(s) and sulphonamide(s), or to any of the excipients; type 1 diabetes (insulin-dependent diabetes), diabetic pre-coma; Any type of acute metabolic acidosis (such as lactic acidosis, diabetic ketoacidosis); Severe renal failure (GFR <30mL/min); acute conditions with the potential to alter renal function such as: dehydration, severe infection, shock; disease which may cause tissue hypoxia (especially acute disease, or worsening of chronic disease) such as as cardiac or respiratory failure, recent myocardial infarction, shock; hepatic insufficiency, acute alcohol intoxication, alcoholism; porphyria; lactation; in association with miconazole (see Interactions).
Lactic acidosis: Lactic acidosis, a very rare, but serious metabolic complication, most often occurs at acute worsening of renal function or cardiorespiratory illness or sepsis. Metformin accumulation occurs at acute worsening of renal function and increases the risk of lactic acidosis.
In case of dehydration (severe diarrhoea or vomiting, fever or reduced fluid intake), metformin should be temporarily discontinued and contact with a health care professional is recommended.
Medicinal products that can acutely impair renal function (such as antihypertensives, diuretics and NSAIDs) should be initiated with caution in metformin-treated patients. Other risk factors for lactic acidosis are excessive alcohol intake, hepatic insufficiency, inadequately controlled diabetes, ketosis, prolonged fasting and any conditions associated with hypoxia, as well as concomitant use of medicinal products that may cause lactic acidosis.
Diagnosis: Patients and/or care-givers should be informed of the risk of lactic acidosis. Lactic acidosis is characterised by acidotic dyspnoea, abdominal pain, muscle cramps, asthenia and hypothermia followed by coma. In case of suspected symptoms, the patient should stop taking metformin and seek immediate medical attention. Diagnostic laboratory findings are decreased blood pH (< 7.35), increased plasma lactate levels (>5 mmol/L) and an increased anion gap and lactate/pyruvate ratio.
Hypoglycaemia: As it contains a sulphonylurea, Glucovance exposes the patient to a risk of onset of hypoglycaemic episodes. After treatment initiation, a progressive dose titration may prevent the onset of hypoglycaemia. This treatment should only be prescribed if the patient adheres to a regular meal schedule (including breakfast). It is important that carbohydrate intake is regular since the risk of hypoglycaemia is increased by a late meal, insufficient or unbalanced carbohydrate intakes. Hypoglycaemia is more likely to occur in case of energy-restricted diet, after intensive or prolonged exercise, when alcohol intake or during the administration of a combination of hypoglycaemic agents.
Diagnosis: The symptoms of hypoglycaemia are: headache, hunger, nausea, vomiting, extreme tiredness, sleep disorder, restlessness, aggression, impaired concentration and reactions, depression, confusion, speech impediment, visual disturbances, trembling, paralysis and paraesthesia, dizziness, delirium, convulsions, somnolence, unconsciousness, superficial breathing and bradycardia. Due to a counterregulation caused by the hypoglycaemia, sweating, fear, tachycardia, hypertension, palpitations, angina and arrhythmia can occur. These latter symptoms can be absent when the hypoglycaemia is developed slowly, in case of autonomic neuropathy or when the patients take beta-blocking agents, clonidine, reserpine, guanethidine or sympathomimetics.
Management of hypoglycaemia: Moderate hypoglycaemic symptoms without loss of consciousness or neurological manifestations should be corrected by the immediate intake of sugar. An adjustment to the dosage and/or changes to meal patterns should be ensured. Severe hypoglycaemic reactions with coma, seizures or other neurological signs are also possible and constitute a medical emergency requiring immediate treatment with intravenous glucose once the cause is diagnosed or suspected, prior to prompt hospitalisation of the patient.
The careful selection of patients and dosage and adequate instructions for the patient are important to reduce the risk of hypoglycaemic episodes. If the patient encounters repeated episodes of hypoglycaemia, which are either severe or associated with unawareness of the situation, antidiabetic treatment options other than Glucovance should be taken into consideration.
Factors favouring hypoglycaemia: concomitant administration of alcohol, especially combined with fasting; refusal or (more particularly in elderly patients) inability of the patient to co-operate; malnutrition, irregular meals, missed meals, fasting or changes to diet; poor balance between physical exercise and carbohydrate intake; renal failure; severe liver failure; overdose of Glucovance; certain endocrine disturbances: thyroid insufficiency, pituitary and adrenal gland insufficiency; concomitant administration of certain other drugs (see Interactions).
Patient information: The risks of hypoglycaemia, its symptoms and its treatment, as well as its predisposing conditions, must be explained to the patient and his or her family. Similarly, the risk of lactic acidosis must be considered in the event of non-specific signs such as muscle cramps accompanied by digestive disorders, abdominal pain and severe asthenia, dyspnoea attributed to acidosis, hypothermia and coma.
In particular, the patient should be informed of the importance of adhering to a diet, following a programme of regular physical exercise and making regular checks on glycaemia.
Blood sugar imbalance: In case of surgery or any other cause of diabetic decompensation, temporary insulin therapy should be envisaged instead of this treatment.
The symptoms of hyperglycaemia are: increased urinating, raging thirst and a dry skin.
Cardiac function: Patients with heart failure are more at risk of hypoxia and renal insufficiency. In patients with stable chronic heart failure, Glucovance may be used with a regular monitoring of cardiac and renal function.
For patients with acute and unstable heart failure, Glucovance is contraindicated.
Renal function: GFR should be assessed before treatment initiation and regularly thereafter [See Dosage & Administration]. Metformin is contraindicated in patients with GFR <30 mL/min and should be temporarily discontinued in the presence of conditions that alter renal function [See Contraindications].
Administration of iodinated contrast materials: Intravascular administration of iodinated contrast agents may lead to contrast induced nephropathy, resulting in metformin accumulation and an increased risk of lactic acidosis. Glucovance should be discontinued prior to or at the time of the imaging procedure and not restarted until at least 48 hours after, provided that renal function has been re-evaluated and found to be stable, see Dosage & Administration and Interactions.
Concomitant use of glibenclamide with other medicinal products: The concomitant use of glibenclamide with alcohol, phenylbutazone or danazol is not recommended (see Interactions).
Surgery: Because Glucovance contains metformin hydrochloride, Glucovance must be discontinued 48 hours before elective surgery under general, spinal or peridural anaesthesia and may not be reinstituted earlier than 48 hours following surgery or resumption of oral nutrition and only after renal function has been re-evaluated and found to be normal.
Other precautions: All patients should continue their diet, with a regular distribution of carbohydrate intake during the day. Overweight patients should continue their energy-restricted diet.
Regular physical exercise is as necessary as taking Glucovance.
The usual laboratory tests for diabetes monitoring (glycaemia, HbA1c) should be performed regularly.
Metformin may reduce vitamin B12 serum levels. The risk of low vitamin B12 levels increases with increasing metformin dose, treatment duration, and/or in patients with risk factors known to cause vitamin B12 deficiency. In case of suspicion of vitamin B12 deficiency (such as anemia or neuropathy), vitamin B12 serum levels should be monitored. Periodic vitamin B12 monitoring could be necessary in patients with risk factors for vitamin B12 deficiency. Metformin therapy should be continued for as long as it is tolerated and not contra-indicated and appropriate corrective treatment for vitamin B12 deficiency provided in line with current clinical guidelines.
Treatment of patients with G6PD-deficiency with sulphonylurea agents can lead to haemolytic anaemia. Since glibenclamide belongs to the chemical class of sulphonylurea drugs, caution is recommended when using Glucovance in patients with G6PD-deficiency and a non-sulphonylurea alternative may be considered.
Because this medicinal product contains lactose, it is contraindicated in case of congenital galactosemia, glucose and galactose malabsorption syndrome or in case of lactase deficiency.
Effects on ability to drive and use machines: Patients should be alerted to the symptoms of hypoglycaemia and should be advised to exercise caution when driving or using machines.
Renal and hepatic failure: The pharmacokinetics and/or pharmacodynamics of Glucovance may be modified in patients with hepatic failure or severe renal failure. If hypoglycaemia occurs in such patients, it may be prolonged, and appropriate treatment must be initiated.
Use in the Elderly: Age 65 years and older has been identified as a risk factor for hypoglycemia in patients treated with sulfonylureas. Hypoglycemia can be difficult to recognize in the elderly. Starting and maintenance doses of glibenclamide must be carefully adjusted to reduce the risk of hypoglycaemia (see Dosage & Administration).
Pregnancy: No preclinical and clinical data on exposed pregnancies are available for Glucovance.
Risk related to diabetes: When uncontrolled, diabetes (gestational or permanent) gives rise to an increase in congenital abnormalities and perinatal mortality. Diabetes must be controlled as far as possible during the period of conception in order to reduce the risk of congenital abnormalities.
Risk related to metformin (see Pharmacology: Toxicology: Preclinical safety data under Actions): Animal studies do not indicate harmful effects with respect to pregnancy, embryonic or fetal development, parturition or postnatal development.
A limited amount of data from the use of metformin in pregnant women does not indicate an increased risk of congenital abnormalities.
Risk related to glibenclamide (see Pharmacology: Toxicology: Preclinical safety data under Actions): Studies in animals have shown no evidence of teratogenic activity. In the absence of a teratogenic effect in animals, foetal malformation in humans is not to be expected since to date, substances known to cause malformation in humans have proved to be teratogenic in well-conducted animal studies in two species.
In clinical practice, there are currently no relevant data on which to base an evaluation of potential malformation or fetotoxicity due to glibenclamide when administered during pregnancy.
Management: Adequate blood glucose control allows pregnancy to proceed normally in this category of patients. Glucovance must not be used for the treatment of diabetes during pregnancy.
It is imperative that insulin be used to achieve adequate blood glucose control. It is recommended that the patient be transferred from oral antidiabetic therapy to insulin as soon as the patient plans to become pregnant or if pregnancy is exposed to this medicinal product. Neonatal blood glucose monitoring is recommended.
Breast-feeding: Metformin is excreted in milk in lactating rats. In humans, in the absence of data concerning passage of metformin and glibenclamide into breast milk, and in view of the risk of neonatal hypoglycaemia, this medicinal product is contraindicated in the event of breast-feeding.
Fertility: Fertility of male or female rats was unaffected by metformin when administered at doses as high as 600 mg/kg/day, which is approximately three times the maximum recommended human daily dose based on body surface area comparisons.
Fertility of male or female rats was unaffected by glibenclamide when administered orally at dose of 100 and 300 mg/kg/day.
During treatment initiation, the most common adverse reactions are nausea, vomiting, diarrhoea, abdominal pain and loss of appetite which resolve spontaneously in most cases. To prevent them, it is recommended to take Glucovance in 2 or 3 daily doses and to increase slowly the doses.
Transient visual disturbances may occur at the start of treatment due to a decrease in glycaemia levels.
The following undesirable effects may occur under treatment with Glucovance. Frequencies are defined as follows: very common ≥1/10; common ≥1/100, <1/10; uncommon ≥1/1,000, <1/100; rare ≥1/10,000, <1/1,000); very rare <1/10,000; not known (cannot be estimated from the available data).
Blood and lymphatic system disorders: These are reversible upon treatment discontinuation.
Rare: Leukopenia, thrombocytopenia.
Very rare: Agranulocytosis, haemolytic anaemia, bone marrow aplasia and pancytopenia.
Metabolism and nutrition disorders: Hypoglycaemia (see Precautions).
Common: Vitamin B12 decrease/deficiency (see Other Precautions under Precautions).
Uncommon: Crises of hepatic porphyria and porphyria cutanea.
Very rare: Lactic acidosis (see Precautions).
Disulfiram-like reaction with alcohol intake.
Nervous system disorders: Common: Taste disturbance.
Eye disorders: Transient visual disturbances may occur at the start of treatment due to a decrease in glycaemia levels.
Gastrointestinal disorders: Very common: Gastrointestinal disorders such as nausea, vomiting, diarrhoea, abdominal pain and loss of appetite. These undesirable effects occur more frequently during treatment initiation and resolve spontaneously in most cases. To prevent them, it is recommended that Glucovance be taken in 2 or 3 daily doses. A slow increase of the dose may also improve gastrointestinal tolerability.
Skin and subcutaneous tissue disorders: A cross reactivity to sulphonamide(s) and their derivatives may occur.
Rare: Skin reactions such as pruritus, urticaria, maculopapular rash.
Very rare: Cutaneous or visceral allergic angiitis, erythema multiforme, exfoliative dermatitis, photosensitization, urticaria evolving to shock.
A cross reactivity to sulphonamide(s) and their derivatives may occur.
Hepatobiliary disorders: Very rare: Liver function test abnormalities or hepatitis requiring treatment discontinuation.
Investigations: Uncommon: Average to moderate elevations in serum urea and creatinine concentrations.
Very rare: Hyponatremia.
Contraindicated combination: Related to glibenclamide: Miconazole (systemic route, oromucosal gel): Increase in the hypoglycaemic effect with possible onset of hypoglycaemic manifestations, or even coma (see Contraindications).
Combinations not recommended: Related to sulphonylurea(s): Alcohol: Antabuse effect (intolerance to alcohol), notably for chlorpropamide, glibenclamide, glipizide, tolbutamide.
Increase of the hypoglycaemic reaction (inhibition of compensation reactions), which may facilitate the onset of a hypoglycaemic coma (see Precautions).
Avoid consumption of alcohol and alcohol-containing medications.
Phenylbutazone (systemic route): Increase in the hypoglycaemic effect of sulphonylurea(s) (displacement of sulphonylurea(s) from protein-binding sites and/or decrease in their elimination). Preferably use another anti-inflammatory agent exhibiting fewer interactions, or else warn the patient and step up self-monitoring; if necessary, adjust the dosage during treatment with the anti-inflammatory agent and after its withdrawal.
Related to all antidiabetic agents: Danazol: If the combination cannot be avoided, warn the patient and step up self-monitoring of blood glucose. Possibly adjust the dosage of the antidiabetic treatment during treatment with danazol and after its withdrawal.
Related to metformin: Alcohol: Alcohol intoxication is associated with an increased risk of lactic acidosis during acute alcoholic intoxication, particularly in cases of fasting (see Precautions) or malnutrition and hepatic impairment.
Avoid drinking alcoholic beverages and taking drugs that contain alcohol.
Combinations requiring precautions: Related to all antidiabetic agents: Chlorpromazine: At high dosages (100 mg per day of chlorpromazine), elevation in blood glucose (reduction in release of insulin).
Precaution for use: warn the patient and step up self-monitoring of blood glucose. Possibly adjust the dosage of the antidiabetic during treatment with the neuroleptic and after its withdrawal.
Corticosteroids (glucocorticoids) and tetracosactides (systemic and local routes): Elevation in blood glucose, sometimes accompanied by ketosis (decreased carbohydrate tolerance with corticosteroids).
Precaution for use: warn the patient and step up self-monitoring of blood glucose. Possibly adjust the dosage of the antidiabetic during treatment with corticosteroids and after their withdrawal.
β2-agonists: Elevation in blood glucose due to the β2-agonists.
Precaution for use: warn the patient, step up blood glucose monitoring and possibly transfer to insulin therapy.
Angiotensin converting enzyme inhibitors (e.g. captopril, enalapril): ACE inhibitors may decrease the blood glucose levels. If necessary, adjust the dosage of Glucovance during therapy with an ACE inhibitor and upon its discontinuation.
Related to metformin: Diuretics: Lactic acidosis due to metformin triggered by any functional renal insufficiency, related to diuretics and more particularly to loop diuretics.
Iodinated contrast materials: Intravascular administration of iodinated contrast materials may lead to renal failure. This may induce metformin accumulation and may expose to lactic acidosis. Depending on the renal function, Glucovance must be discontinued 48 hours before the test or at the time of the test and not reinstituted until 48 hours afterwards, and only after renal function has been re-evaluated and found to be normal.
Organic cation transporters (OCT): Metformin is a substrate of both transporters OCT1 and OCT2.
Co-administration of metformin with: Substrates/inhibitors of OCT1 (such as verapamil) may reduce efficacy of metformin.
Inducers of OCT1 (such as rifampicin) may increase gastrointestinal absorption and efficacy.
Substrates/inhibitors of OCT2 (such as cimetidine, dolutegravir, crizotinib, olaparib, daclatasvir, vandetanib) may decrease the renal elimination of metformin and thus lead to an increase metformin plasma concentration.
Therefore, caution is advised when these drugs are co-administered with metformin and a dose adjustment may be considered, particularly in patients with renal impairment.
Related to glibenclamide: Beta-blockers: All beta-blockers mask some of the symptoms of hypoglycaemia: palpitations and tachycardia; Most non-cardioselective beta-blockers increase the incidence and severity of hypoglycaemia.
Warn the patient and step up blood glucose self-monitoring, especially at the start of treatment.
Fluconazole: Increase in the half-life of sulphonylurea with possible onset of hypoglycaemic manifestations.
Warn the patient and step up blood glucose self-monitoring, and possibly adjust the dosage of the antidiabetic treatment during treatment with fluconazole and after its withdrawal.
Bosentan: Risk of decreased hypoglycaemic effect of glibenclamide because bosentan reduces the plasma concentration of glibenclamide. An increased risk of liver enzyme elevations was reported in patients receiving glibenclamide concomitantly with bosentan.
Warn the patient, set-up monitoring of glycaemia and liver enzymes and adjust the dosage of the antidiabetic treatment if necessary.
Bile acid sequestrants: When co-administered simultaneously the plasma concentration of glibenclamide is reduced which may lead to a reduced hypoglycaemic effect. This effect was not observed if glibenclamide is given in a certain period of time before taking the other medicine. It is recommended that Glucovance should be administered at least 4 hours prior a bile acid sequestrant.
Other interaction: combination to be taken into account: Related to glibenclamide: Desmopressin: Reduction in antidiuretic activity.
Colesevelam: When co-administered simultaneously the plasma concentration of glibenclamide is reduced which may lead to a reduced hypoglycaemic effect. This effect was not observed when glibenclamide is given in time lag. It is recommended that Glucovance should be administered at least 4 hours prior colesevelam.
Incompatibilities: Not applicable.
Special precautions for disposal: Any unused product or waste material should be disposed of in accordance with local requirements.
Store below 30°C.
This medicinal product does not require any special storage conditions.
Shelf life: 3 years.
A10BD02 - metformin and sulfonylureas ; Belongs to the class of combinations of oral blood glucose lowering drugs. Used in the treatment of diabetes.
Glucovance 500 mg/2.5 mg FC tab
120's
Glucovance 500 mg/5 mg FC tab
120's


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out
