


 Sign Out
Sign Out

General Consideration: Dosage of Glucovance must be individualized on the basis of both effectiveness and tolerance while not exceeding the maximum recommended daily dose of 2000 mg metformin/20 mg glibenclamide. Glucovance should be given with meals with a sufficiently high carbohydrate content to prevent the onset of hypoglycaemic episode. Glucovance should be initiated at a low dose, with gradual dose escalation described as follows, in order to avoid hypoglycaemia (largely due to glibenclamide), to reduce GI side effects (largely due to metformin), and to permit determination of the minimum effective dose for adequate control of blood glucose for the individual patient.
With initial treatment and during dose titration, appropriate blood glucose monitoring should be used to determine the therapeutic response to Glucovance and to identify the minimum effective dose for the patient. Thereafter, HbA1c (glycosylated haemoglobin) should be measured at intervals of approximately 3 months to assess the effectiveness of therapy. The therapeutic goal in all patients with type 2 diabetes is to decrease FPG, PPG, and HbA1c, to normal or as near normal as possible. Ideally, the response to therapy should be evaluated using HbA1c which is a better indicator of long-term glycaemic control than FPR alone.
No studies have been performed specifically examining the safety and efficacy of switching of Glucovance therapy in patients taking concomitant glibenclamide (or other sulphonylurea) plus metformin. Changes in glycaemic control may occur in such patients, with either hyperglycaemia or hypoglycaemia possible. Any change in therapy of type 2 diabetes should be undertaken with care and appropriate monitoring.
When Glucovance is co-administered with colesevelam, it is recommended that Glucovance should be administered at least 4 hours prior to colesevelam in order to minimize the risk of reduced absorption.
Glucovance Use in Previously Treated Patients (Second-Line Therapy): Recommended starting dose: 500/2.5 mg or 500/5 mg twice daily with meals.
For patients not adequately controlled on either glibenclamide (or another sulphonylurea) or metformin alone, the recommended starting dose of Glucovance is 500/2.5 mg or 500/5 mg twice daily with the morning and evening meals. In order to avoid hypoglycaemia, the starting dose of Glucovance should not exceed the daily doses of glibenclamide or metformin already being taken. The daily dose should be titrated in increments of no more than 500/5 mg up to the minimum effective dose to achieve adequate control of blood glucose or to a maximum dose of 2000 mg/20 mg per day.
For patients previously treated with combination therapy of glibenclamide (or another sulphonylurea) plus metformin, if switched to Glucovance, the starting dose should not exceed the daily dose of glibenclamide (or equivalent dose of another sulphonylurea) and metformin already being taken. Patients should be monitored closely for signs and symptoms of hypoglycaemia following such a switch and the dose of Glucovance should be titrated as described previously to achieve adequate control of blood glucose.
The tablets should be taken with meals. The dosage regimen should be adjusted according to the individual eating habits. However, any intake must be followed by a meal with a sufficiently high carbohydrate content to prevent the onset of hypoglycaemic episodes.
When Glucovance is co-administered with a bile acid sequestrant, it is recommended that Glucovance should be administered at least 4 hours prior to the bile acid sequestrant in order to minimize the risk of reduced absorption (see Interactions).
Renal Impairment: A GFR should be assessed before initiation of treatment with metformin containing products and at least annually thereafter. In patients at an increased risk of further progression of renal impairment and in the elderly, renal function should be assessed more frequently, e.g. every 3-6 months. The maximum daily dose of metformin should preferably be divided into 2-3 daily doses. Factors that may increase the risk of lactic acidosis should be reviewed before considering initiation of metformin in patients with GFR <60 ml/min. If no adequate strength of Glucovance is available, individual monocomponents should be used instead of the fixed dose combination. (See table.)
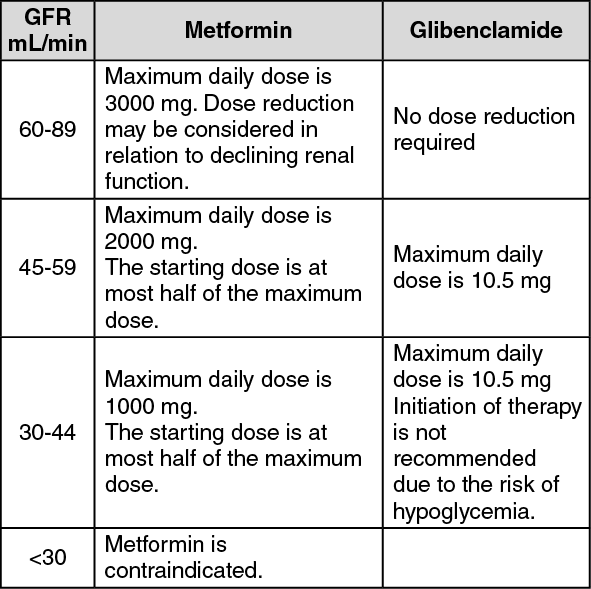 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageGeriatric population: The dosage of Glucovance should be adjusted depending on renal function parameters (start with 1 tablet of Glucovance 500 mg/2.5 mg); regular checks on the renal function are necessary (see Precautions).
Patients aged 65 years and older: starting and maintenance doses of glibenclamide must be carefully adjusted to reduce the risk of hypoglycaemia. Treatment should be started with the lowest available dose and increased gradually if necessary (see Precautions).
Paediatric population: Glucovance is not recommended for use in children (see Pharmacology: Pharmacodynamics under Actions).