Effervescent tab: FLUIMUCIL 600 mg white circular tablets, with a characteristic lemon, slightly sulphureous odour.
Powd for oral soln: FLUIMUCIL 100 mg and FLUIMUCIL 200 mg yellow granules with a characteristic orange and slightly sulphureous odour.
Syrup: Clear or slightly opalescent, colourless solution with a characteristic odour of raspberry.
100 ml oral solution contains: Active principle: N-acetylcysteine 2.00 g.
Excipients with known effects: sodium, sodium benzoate, methyl parahydroxybenzoate, ethanol, propylene glycol.
Excipients/Inactive Ingredients: Methyl para-hydroxybenzoate, sodium benzoate, disodium edetate, sucralose, carmellose sodium, saccharin sodium, raspberry flavour (containing Propylene glycol, ethyl alcohol and flavouring substances), sodium cyclamate, sodium hydroxide, purified water.
Pharmacotherapeutic group: Syrup: mucolytics. ATC: R05CB01.
Pharmacology: Effervescent tab/Powd for oral soln: N-acetyl-L-cysteine (NAC), the active ingredient of FLUIMUCIL exerts an intense mucolytic action on mucous and mucopurulent secretions, by depolymerizing the mucoproteic complexes and the nucleic acids which confer viscosity to the vitreous and purulent component of the sputum and of other secretions.
Furthermore, NAC, exerts a direct antioxidant action, being provided with a free thiol (-SH nucleophillic) group, which is able to interact directly with the electrophilic groups of the oxidant radicals. Of particular interest is the recent demonstration that NAC protects the a1-antitrypsin, enzyme inhibitor of elastase, from the inactivation due to the action of hypochlorous add (HOCI), a powerful oxidant agent produced by the myeloperoxidase enzyme of activated phagocytes.
These features make FLUIMUCIL A particularly suitable for the treatment of acute and chronic affections of the respiratory system, characterized by thick and viscous mucous and mucopurulent secretions. Furthermore, the molecular structure permits the molecule to cross easily cellular membranes. Inside the cell, NAC is deacetylized, forming L-cysteine, an amino acid indispensable for glutathione synthesis (GSH).
GSH is a highly reactive tripeptide, found ubiquitously in the various tissues of animals and is essential for the maintenance of functional capacity as well as cellular morphological integrity, as it represents the most important protective, endocellular mechanism against oxidant radials, either of external or internal nature, as well as towards numerous cytotoxic substances.
NAC plays a role of primary importance in the maintenance of adequate GSH levels thus contributing to the cellular protection from harmful agents which, through progressive GSH depletion, would be able to express their cytotoxic action, as the case of acetaminophen poisoning.
Due to this mechanism of action, NAC is also indicated as a specific antidote in acetaminophen poisoning, in the course of a cyclophosphamide treatment and a haemorrhagic cystitis, (in the latter case it provides SH-groups necessary to inactivate acrolein, a toxic metabolite that affects the urinary mucosae, whilst not interfering with chemotherapy).
Syrup: Pharmacodynamics: N-acetyl-L-cysteine (NAC), the active substance of Fluimucil, has an intense mucolytic-fluidifying action on mucous and mucopurulent secretions. It depolymerises the mucoprotein complexes and the nucleic acids that confer viscosity to the glassy and purulent elements of the sputum and other secretions.
NAC, as such, also has a direct antioxidant action because it has a free nucleophilic thiol group (SH) that can interact directly with the electrophilic groups of oxidising radicals. The recent evidence showing that NAC protects α1-antitrypsin (an elastase-inhibiting enzyme) from inactivation by hypochlorous acid (HOCl), a powerful oxidising agent produced by the myeloperoxidase enzyme of activated phagocytes, is particularly interesting. The molecule's structure allows it to easily cross cellular membranes. Inside the cell, NAC is de-acetylated and L-cysteine becomes available - this amino acid is essential for glutathione synthesis (GSH).
GSH is a highly reactive tripeptide that is ubiquitously present in the various tissues of animals. It is essential for maintaining the cell's capacity to function and its morphological integrity, because it is the most important intra-cellular defense mechanism against oxidising radicals (endogenous or exogenous) and against many cytotoxic substances.
These activities make Fluimucil particularly suitable for treating acute and chronic infections of the airways characterised by thick, viscous mucous and mucopurulent secretions.
Pharmacokinetics: Effervescent tab/Powd for oral soln: Absorption: Acetylcysteine absorption after oral administration is rapid and complete.
The bioavailability of free acetylcysteine is only of 10%, due to a high first-pass metabolism.
After administration of a relatively high dose of 30 mg/kg body weight acetylcysteine, total acetylcysteine (free and bound) peak plasma concentration is about 67 nmol/ml, with a tmax of 0.75-1 hour.
After administration of 600 mg acetylcysteine in the form of tablets, the peak plasma concentration (Cmax) of total acetylcysteine (free and bound) amounts to 3.40 μg/ml (20.83 nmol/ml) with a tmax of 0.71 h (43 minutes). The AUC (area under the curve) is 10.06 μg*h/ml. The effect of food intake on systemic bioavailability after orally administered acetylcysteine has not been tested.
Distribution: Acetylcysteine is found in the body both in unchanged form and as oxidative metabolites, either in free form or reversibly bound to plasma proteins through disulfide bonds.
Acetylcysteine is mainly spread within the extracellular aqueous milieu. It is found mostly in the liver, kidneys, lungs and bronchial mucus.
Biotransformation: The metabolic process starts soon after the product administration: acetylcysteine is deacetylated in the intestinal wall through first-pass metabolism to L-cysteine, equally active, and then metabolized to inactive products.
Élimination: Approximately 30% of the administered dose is eliminated directly by renal excretion. The main metabolites are cystine and cysteine, but also small amounts of taurine and sulfates are excreted.
No studies concerning the elimination of the non-renally cleared fraction are available to date. After intravenous administration of 200 mg acetylcysteine in 6 subjects, an elimination half-life of 1.95 (0.95-3.57) hours for the reduced forms and of 5.58 (4.1-9.5) hours for total acetylcysteine was observed. After administration by oral route of a 400mg effervescent tablet (not identical to Fluimucil formulations), the half-life of total acetylcysteine amounts to 6.25 (4.59-10.6) hours.
Syrup: Absorption: In humans, acetylcysteine is completely absorbed after oral administration. Because of the gut wall metabolism and first-pass effect, the bioavailability of acetylcysteine taken orally is very low (approx. 10%). No differences were reported for the various pharmaceutical forms. In patients with various respiratory or cardiac diseases, the maximum plasma concentration (Cmax) is obtained between 2 to 3 hours after administration and the levels remain high over a period of 24 hours.
Distribution: Acetylcysteine is distributed both in the non-metabolized (20%) and the metabolized (active) (80%) form, and can mainly be found in the liver, kidneys, lungs, and bronchial secretions.
The volume of distribution of acetylcysteine ranges from 0.33 to 0.47 L/kg. Protein binding is about 50%, four hours after the dose and decreases to 20% at 12 h.
Acetylcysteine crosses the placenta.
Biotransformation: Acetylcysteine undergoes rapid and extensive metabolism in the gut wall and liver following oral administration.
The resulting compound, cysteine, is considered to be an active metabolite. Following this stage of transformation, acetylcysteine and cysteine share the same metabolic route.
Elimination: Renal clearance may account for about 30% of total body clearance. Following oral administration, the terminal half-life of total acetylcysteine is 6.25 (4.59 to 10.6) hours.
Linearity/non-linearity: The pharmacokinetics of acetylcysteine is proportional to the administered dose in the dose range between 200-3200 mg/m2 for area under the plasma concentration time curve (AUC) and Cmax.
Toxicology: Preclinical safety data: Syrup: Non-clinical data reveal no special hazard for humans based on conventional studies of safety pharmacology, repeated dose toxicity, genotoxicity and toxicity to reproduction and development.
In acute toxicity studies, the oral LD50 values were determined as 8 g/kg and >10 g/kg in mice and rats, respectively.
In prolonged administration for 12 weeks, a dose of 1 g/kg/day by the oral route was well tolerated in rats. In dogs, the oral administration of 300 mg/kg/day for a period of one year did not result in toxic reactions.
Acetylcysteine was considered to be non-genotoxic on the basis of in vitro and in vivo studies.
Reproductive studies were conducted in rats at oral doses of up to 2,000 mg/kg per day and in rabbits at oral doses of up to 1,000 mg/kg per day; they did not demonstrate any impairment in female fertility or harmful effects on the foetus due to acetylcysteine. In addition, the treatment of male rats with acetylcysteine at an oral dose of 250 mg/kg per day for 15 weeks did not affect the fertility or general reproductive performance of the animals.
All respiratory tract diseases leading to the formation of thick secretions difficult to be expectorated, such as acute and chronic bronchitis, laryngitis, sinusitis, tracheitis, influenza, bronchial asthma and (as complementary treatment) mucoviscidosis.
Usual posology for acute diseases: Adults: 600 mg daily, divided into one or more administrations (e.g. 200 mg sachets 3 times daily or 10 ml 3 times daily or 30 ml daily).
Adolescents over 12 years of age: 600 mg daily, divided into one or more administrations (e.g. 200 mg sachets 3 times daily or 10 ml 3 times daily or 30 ml daily).
Children from 2 to 12 years of age: one 100 mg sachet 3 times daily or 200 mg twice daily or 300 mg (e.g., half measuring cup (5 ml) 3 times daily) or 400 mg (e.g., one 10 ml measuring cup twice times daily).
Special posologies: Long-term treatment: 400-600 mg daily, divided into one or more administrations, with a maximum treatment duration of 3-6 months.
If the excessive mucus production and the consequent cough do not disappear after a two-week treatment, the diagnosis should be re-evaluated in order to exclude a possible malignant disease of the respiratory tract.
Mucoviscidosis: the same dosage as previously mentioned, however, for children from 6 years of age, 200 mg 3 times daily or 600 mg once daily.
Effervescent tab/Powd for oral soln: Modality of Use: Dissolve the content of one sachet or the effervescent tablet into a glass of cold or warm water.
Effects of food on drug absorption are unknown. Therefore no recommendations on taking FLUIMUCIL before or after meals can be made.
Syrup: Method of administration: For Oral use.
No interactions with food have been reported; there are no indications concerning administration of the medicinal product before or after meals.
Healthy volunteers were treated for three months with an oral dose of 11.2 g of acetylcysteine per day without any serious undesirable effects being observed. Oral doses of up to 500 mg acetylcysteine per kg body weight have been tolerated without any signs of toxicity.
Symptoms: Overdose may lead to gastrointestinal effects such as nausea, vomiting and diarrhoea.
Treatment: There are no antidotes to acetylcysteine and treatments are symptomatic.
Hypersensitivity to the active substance acetylcysteine or to any of the excipients according to the composition.
Small children or infants under 2 years.
Effervescent tab/Powd for oral soln: Active peptic ulcer.
Effervescent tab/Powd for oral soln: Effervescent tablets, granules and tablets containing 600mg acetylcysteine cannot be used in children under 12 years (and in children with cystic fibrosis under 6 years).
The simultaneous administration of an antitussive drug is not reasonable from a medical point of view (see as follows).
Caution is recommended in patients with a risk for gastrointestinal haemorrhage (for example, in latent peptic ulcer or oesophageal varices), as orally administered acetylcysteine can induce vomiting.
Due to the risk of bronchospasm, caution is also recommended in patients with bronchial asthma and a hyper-reactive bronchial system.
When hypersensitivity reactions or bronchospasm occur, the medicine should be discontinued immediately, and if necessary appropriate measures must be taken.
The use of acetylcysteine might, mainly at treatment start, fluidify bronchial secretions and promote expectoration. If the patient is not able to effectively expectorate, it can be supported with postural drainage and broncho-aspiration.
Acetylcysteine leads in vitro to an inhibition of diamine oxidase (DAO) by 20-50%.
Therefore, caution should be used in patients with histamine intolerance.
The simultaneous administration of antitussive drugs may, by suppressing the cough reflex and the physiological self-cleaning of the respiratory tract, result in congestion of the mucus with a risk of bronchospasm and respiratory tract infection.
Mucolytic agents may cause respiratory obstruction in children under 2 years of age. Due to the physiological characteristics of the airways in this age group, the physiological self-cleaning ability may be limited. Therefore, mucolytic agents should not be used in children under 2 years of age (see "Contraindications").
Excipients of particular interest: Fluimucil granules (100 mg and 200 mg) contains 25 mg of aspartame for each sachet. In case of patients suffering from phenylketonuria, it should be considered that aspartame is a source of phenylalanine.
Patients with rare hereditary problems of galactose intolerance, total lactase deficiency or glucose-galactose malabsorption should not take this medicinal product, as the pharmaceutical form granules contain glucose and lactose.
Patients with rare hereditary problems of fructose intolerance, e.g. hereditary deficiency of fructose-1,6-diphosphatase, should not take this medicinal product, as the pharmaceutical form granules contain sorbitol (that will be metabolized into fructose).
Fluimucil, effervescent tablets contain 20 mg of aspartame. In case of patients suffering from phenylketonuria, it should be considered that aspartame is a source of phenylalanine. Patients with rare hereditary problems of glucose-galactose malabsorption should not take this medicinal product,as the pharmaceutical form effervescent tablets contain glucose.
Fluimucil 600 mg effervescent tablets contain 156,9 mg sodium per effervescent tablet, equivalent to 7,8% of the WHO recommended maximum daily intake of 2 g sodium for an adult.
The maximum daily dose of Fluimucil 200 mg effervescent tablets (e.g. 600 mg) corresponds to 23, 5% of the WHO recommended maximum daily sodium intake and has to be considered high in sodium. This should be considered in patients following a low sodium diet.
In such cases, the use of Fluimucil granules or tablets, which are sodium-free, or an alternative salt-free acetylcysteine preparation is advisable.
Syrup: A productive cough must not be suppressed since this is a fundamental part of the bronchopulmonary defense mechanism.
The combination of a mucolytic with a cough suppressant medicine and/or a substance that dries out secretions (atropinic drug) is not rational.
Mucolytic agents can cause excessive bronchial congestion in infants. This is because their bronchial mucus drainage capacities are limited by the specific physiological characteristics of their airways. These agents must not be used in infants therefore (see Contraindications).
Caution is advised when the product is used in patients with a peptic ulcer or a history of peptic ulcer disease, especially when used concomitantly with other medicinal products known to irritate the mucous membrane of the gastrointestinal tract.
Patients with bronchial asthma must be closely monitored during treatment. In the event of bronchospasm, acetylcysteine must be stopped immediately and appropriate treatment initiated.
Bronchial secretions may become more fluid and increase in volume, particularly at the start of treatment with acetylcysteine. If a patient is unable to cough up the secretions effectively, postural drainage and broncho-aspiration should be performed.
Acetylcysteine may have a moderate effect on histamine metabolism; consequently, caution is required if this medicinal product is given as long-term treatment in patients with histamine intolerance due to the potential development of intolerance symptoms (headaches, vasomotor rhinitis, pruritus).
A mild sulfur odour does not indicate a change in the medicinal product but is a property of the active substance itself.
This medicinal product contains methyl parahydroxybenzoate (E218) and may cause allergic reactions (possibly delayed).
This medicinal product contains 38.21 mg sodium per 10-mL measuring cup, equivalent to 1.9% of the WHO recommended maximum daily intake of 2 g sodium for an adult.
This medicinal product contains 15 mg of sodium benzoate per 10-mL measuring cup.
This medicinal product contains 4.88 mg of alcohol (ethanol) per 10-mL measuring cup. The quantity per 10-mL measuring cup of this medicinal product is equivalent to at least 1 mL of beer or 1 mL of wine.
The small quantity of alcohol in this medicinal product is not likely to cause any noteworthy effects.
This medicinal product contains 23.4 mg of propylene glycol per 10-mL measuring cup.
Treatment must be re-assessed if the symptoms or condition persist or worsen.
Effects on ability to drive and use machines: N-acetylcysteine has no effect on the ability to drive vehicles or use machines.
Effervescent tab/Powd for oral soln: Pregnancy: Data from a limited number of exposed pregnant women showed no adverse effects on pregnancy or the health of the foetus or the newborn.
No experience from epidemiological studies is available.
Animal studies do not indicate direct or indirect toxicity with any effect on pregnancy, embryonic development, development of the foetus and/or postnatal development.
Caution is indicated when used in pregnancy.
Lactation: There are no studies showing whether or not acetylcysteine passes into breast milk.
Fluimucil should not be used during breast-feeding, unless absolutely necessary.
Syrup: Pregnancy: There are limited data about the use of acetylcysteine in pregnant women. Animal studies do not indicate direct or indirect harmful effects with respect to reproductive toxicity.
As a precautionary measure, it is preferable to avoid the use of Fluimucil Syrup during pregnancy.
The benefit-risk balance should be assessed before using the product during pregnancy.
Breast-feeding: It is not known whether acetylcysteine and its metabolites are excreted in breast milk.
A risk to the breastfed infant cannot be excluded.
A decision must be made whether to discontinue breast-feeding or to discontinue/abstain from Fluimucil Syrup therapy taking into account the benefit of breastfeeding for the child and the benefit of therapy for the woman.
Fertility: There are no data available concerning the effect of acetylcysteine in human fertility. Animal studies do not indicate any harmful effects with respect to human fertility at the recommended dose.
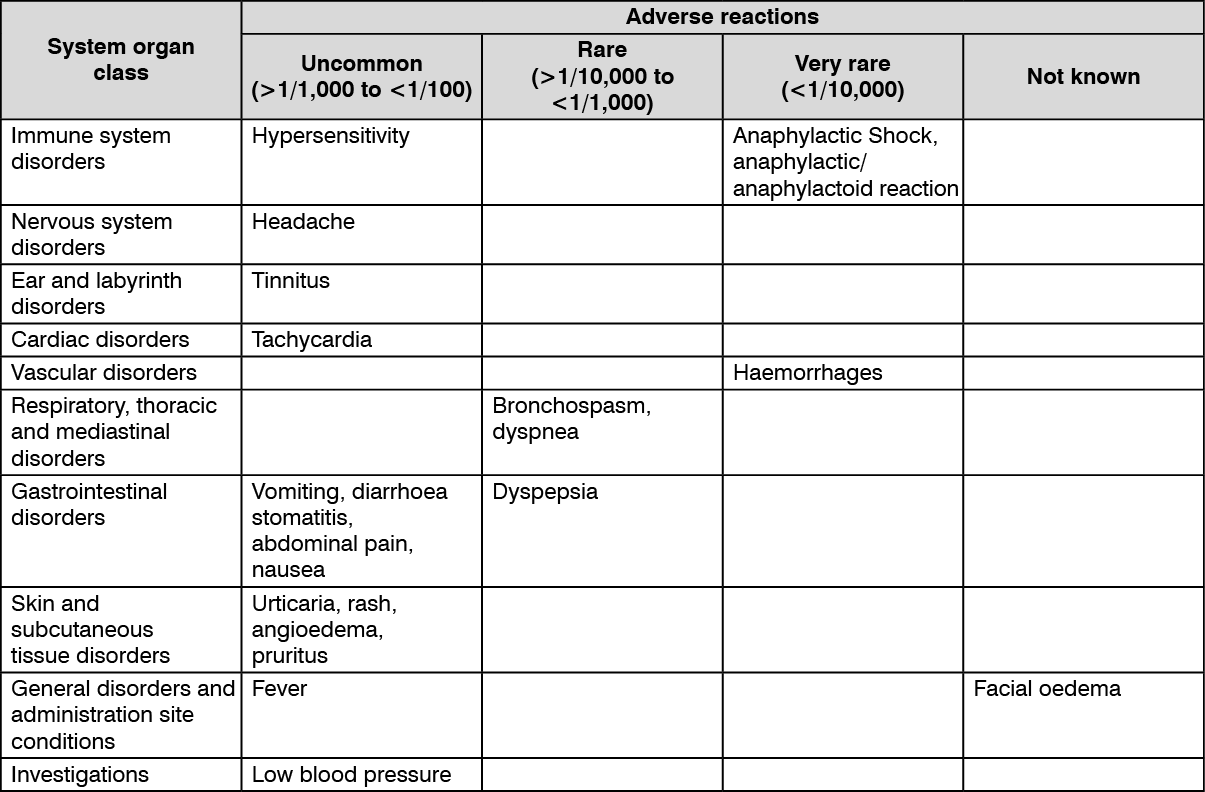
Syrup: Summary of the safety profile: The adverse effects most commonly associated with the oral administration of N-acetylcysteine are gastrointestinal. Hypersensitivity reactions including anaphylactic shock, anaphylactic/anaphylactoid reactions, bronchospasm, angioedema, rash and pruritus have been reported less frequently.
Summary table of undesirable effects: The table as follows lists the undesirable effects recorded according to system/organ class and frequency: very common (≥1/10), common (≥1/100 - <1/10), uncommon (≥1/1,000 - <1/100), rare (≥1/10,000 to <1/1,000), very rare (<1/10,000) and not known (cannot be estimated from the available data).
Within each frequency group, undesirable effects are presented in order of decreasing seriousness. (See table.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
There is also a risk of worsening of bronchial congestion, especially in infants and in certain patients incapable of effective expectoration.
Description of some adverse reactions: Severe skin reactions such as Stevens-Johnson syndrome and Lyell's syndrome have been reported in very rare cases with a chronological connection with the use of acetylcysteine. In most cases, at least one other suspect medicinal product that was more likely to have been the cause of the mucocutaneous syndrome could be identified. In the event of the recent onset of cutaneous or mucosal reactions, medical advice should be sought and the treatment with acetylcysteine should be discontinued immediately.
A decrease in platelet aggregation in the presence of acetylcysteine has been confirmed in various studies. The clinical significance of this has not yet been determined.
Effervescent tab/Powd for oral soln: The following undesirable effects have been observed in the long-term post-marketing experience; their frequency cannot be estimated from the available data: Hypersensitivity reactions, anaphylactic shock, anaphylactic/anaphylactoid reactions; Headache; Tinnitus; Tachycardia; Haemorrhage; Bronchospasm, dyspnea; Vomiting, diarrhoea, stomatitis, abdominal pain, nausea, dyspepsia; Urticaria, rash, angioedema, pruritus; Fever, facial oedema; Blood pressure decreased.
In predisposed patients, hypersensitivity can occur in the form of skin and respiratory organs reactions, and bronchospasm can occur in patients with bronchial asthma and a hyper-reactive bronchial system (see "Precautions").
The occurrence of severe skin reactions such as Stevens-Johnson syndrome and Lyell's syndrome has been very rarely reported in temporal relation to the use of acetylcysteine. In case of new manifestations of cutaneous and mucosal manifestations, a doctor should be consulted immediately, and the use of acetylcysteine should be discontinued. In most of these reported cases, at least one other drug had been used simultaneously and possibly enhanced the observed mucocutaneous effects.
Different studies confirm a decrease in platelet aggregation when using acetylcysteine. The clinical significance of this is still unknown.
The exhaled air may temporarily have an unpleasant odour, probably due to the elimination of hydrogen sulphide from the active substance.
Effervescent tab/Powd for oral soln: There are no in vivo interaction studies.
The co-administration of activated charcoal in case of intoxication may reduce the effect of acetylcysteine administered gastrointestinally.
So far, the reports mentioning an inactivation of antibiotics by acetylcysteine relate exclusively to in-vitro tests in which the substances concerned had been directly mixed. Nevertheless, for safety reasons, the oral administration of antibiotics should be done separately within an interval of at least two hours.
In case of a simultaneous administration of glyceryl trinitrate, the vasodilatory and the inhibiting thrombocytes aggregation effects may be enhanced.
The co-administration of acetylcysteine and carbamazepine may result in subtherapeutic carbamazepine concentrations.
Simultaneous administration of an antitussive: see "Precautions".
Syrup: Mucolytics such as acetylcysteine should not be administered concomitantly with antitussive medicinal products, because a reduction in the cough reflex could cause an accumulation of bronchial secretions.
Activated charcoal can decrease the effect of acetylcysteine.
Simultaneous dissolution of acetylcysteine formulations with other medicinal products is not recommended.
To date, the inactivation of antibiotics by acetylcysteine has been reported only in in vitro tests, whereby the relevant substances were mixed directly with each other. However, if oral antibiotics or other medicinal products are required, it is advised that these should be taken 2 hours before or after acetylcysteine. This does not apply to loracarbef.
It has been shown that the concomitant use of nitrate derivatives and acetylcysteine can cause severe hypotension and an increase in vasodilation of the temporal artery. If concomitant administration of a nitrate derivative and acetylcysteine is necessary, patients must be monitored to detect any hypotension, which could potentially be severe. They must also be warned that they may develop headaches.
The concomitant use of acetylcysteine and carbamazepine can result in sub-therapeutic carbamazepine concentrations.
Paediatric population: Interaction studies have only been conducted in adults.
Laboratory test changes: N-acetylcysteine may interfere with the colorimetric analysis method used to assay salicylates.
N-acetylcysteine may interfere with assay of ketonuria.
Syrup: Incompatibilities: Not applicable.
Special precautions for disposal and other handling: Rinse the measuring cup after use. Recap the bottle after use.
Effervescent tab/Powd for oral soln: FLUIMUCIL 100 mg, FLUIMUCIL 200 mg and FLUIMUCIL A 600 mg: Store below 30°C, prevent from heat and humidity.
Syrup: Store below 25°C.
After opening: Do not store for more than 15 days.
Shelf life: Effervescent tab/Powd for oral soln: 3 years.
Syrup: 2 years.
R05CB01 - acetylcysteine ; Belongs to the class of mucolytics. Used in the treatment of wet cough.
Fluimucil effervescent tab 600 mg
10's (RM35/blister)
Fluimucil powd for oral soln 100 mg
30 × 1's (RM26.8/box)
Fluimucil powd for oral soln 200 mg
30 × 1's
Fluimucil syr 100 mg/5 mL
(raspberry flavour) 100 mL x 1's


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out
