Fluconazole may be administered either orally or by intravenous infusion at a rate of approximately 5-10ml/min, the route being dependent on the clinical state of the patient.
On transferring from the intravenous route to the oral route or vice versa, there is no need to change the daily dose.
The daily dose of fluconazole should be based on the nature and severity of the fungal infection. Most cases of vaginal candidiasis respond to single dose therapy.
Therapy for those types of infections requiring multiple dose treatment should be continued until clinical parameters or laboratory tests indicate that active fungal infection has subsided. An inadequate period of treatment may lead to recurrence of active infection.
For cryptococcal meningitis and cryptococcal infections at other sites, the usual dose is 400 mg on the first day followed by 200 to 400 mg once daily.
Duration of treatment for cryptococcal infections will depend on the clinical and mycological response, but is usually at least 6-8 weeks for cryptococcal meningitis.
For candidemia, disseminated candidiasis and other invasive candidal infections, the usual dose is 400 mg on the first day followed by 200 mg daily.
Depending on the clinical response, the dose may be increased to 400 mg daily.
Duration of treatment is based upon the clinical response.
For oropharyngeal candidiasis, the usual dose is 50 to 100 mg once daily for 7-14 days.
If necessary, treatment can be continued for longer periods in patients with severely compromised immune function.
For atrophic oral candidiasis associated with dentures, the usual dose is 50 mg once daily for 14 days administered concurrently with local antiseptic measures to the denture.
For other candidal infections of mucosa except genital candidiasis (e.g., esophagitis, non-invasive bronchopulmonary infections, candiduria, mucocutaneous candidiasis, etc.) the usual effective dose is 50 to 100 mg daily, given for 14-30 days.
Use In Children: As with similar infections in adults, the duration of treatment is based on the clinical and mycological response.
The maximum adult daily dosage should not be exceeded in children.
Fluconazole is administered as a single dose each day.
The recommended dosage of fluconazole for mucosal candidiasis is 3 mg/kg daily.
A loading dose of 6 mg/kg may be used on the first day to achieve steady state levels more rapidly.
For the treatment of systemic candidiasis and cryptococcal infections, the recommended dosage is 6 to 12 mg/kg daily, depending on the severity of the disease.
Use In Elderly: Where there is no evidence of renal impairment, normal dosage recommendations should be adopted. For patients with renal impairment (creatinine clearance <50 ml/min) the dosage schedule should be adjusted as described as follows.
Use In Renal Impairment: Fluconazole is predominantly excreted in the urine as unchanged drug.
No adjustments in single-dose therapy are necessary.
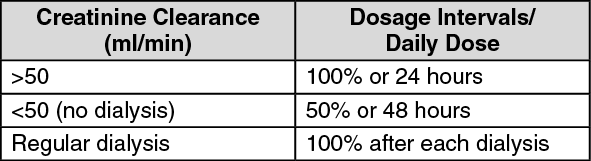
In patients (including children) with impaired renal function who will receive multiple doses of fluconazole, an initial loading dose of 50 to 400 mg should be given.
After the loading dose, the daily dose (according to indication) should be based on the following table: (see table).
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
These are suggested dose adjustments based on pharmacokinetics following administration of single doses. Further adjustment may be needed depending on clinical condition.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out
