General: Prescribing Factive in the absence of a proven or strongly suspected bacterial infection is unlikely to provide benefit to the patient and increases the risk of the development of drug-resistant bacteria.
Rash: In clinical studies, rash occurred more often with Factive than with therapy with comparator agents (2.7% vs. 0.6%). Increasing incidence of rash was associated with younger age (especially below 40), female gender, use of hormone replacement therapy and longer durations of therapy (see Table 4). Urticarial reactions, some of which were not classified as rash, were more common in Factive patients than in comparator patients (0.6% vs. 0.2%). Factive should be discontinued in patients developing a rash or urticaria while on treatment. (See Table 4.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
The most common form of rash associated with Factive was described as maculopapular and mild to moderate in severity. Eighty percent of rashes resolved within 14 days. Approximately 10% of the rashes (0.5% of all patients) were described as of severe intensity and approximately 10% of those with rash were treated with systemic steroids. There were no documented cases in the clinical trials of more serious skin reactions known to be associated with significant morbidity or mortality.
Moderate to severe photosensitivity/phototoxicity reactions, the latter of which may manifest as exaggerated sunburn reactions (e.g., burning, erythema, exudation, vesicles, blistering, edema) involving areas exposed to light (typically the face, "V" area of the neck, extensor surfaces of the forearms, dorsa of the hands), can be associated with use of quinolones after sun or UV light exposure. Therefore, excessive exposure to these sources of light should be avoided. Drug therapy should be discontinued if phototoxicity occurs.
Information for Patients: Advice the patient to read the Consumer Medication Information Leaflet (RiMUP).
Serious Adverse Reactions: Advise patients to stop taking Factive if they experience an adverse reaction and to call their healthcare provider for advice on completing the full course of treatment with another antibacterial drug.
Inform patients of the following serious adverse reactions that have been associated with Factive or other fluoroquinolone use: Disabling and potentially irreversible serious adverse reactions that may occur together, including tendinitis and tendon rupture, peripheral neuropathies, and central nervous system effects, have been associated with use of Factive and may occur together in the same patient. Inform patients to stop taking Factive immediately if they experience an adverse reaction and to call their healthcare provider.
Tendinitis and tendon rupture: instruct patients to contact their healthcare provider if they experience pain, swelling, or inflammation of a tendon, or weakness or inability to use one of their joints; rest and refrain from exercise; and discontinue Factive treatment. The risk of severe tendon disorders with fluoroquinolones is higher in older patients usually over 60 years of age, in patients taking corticosteroid drugs, and in patients with kidney, heart or lung transplants.
Peripheral neuropathies: Inform patients that peripheral neuropathies have been associated with the use of Factive, that symptoms may occur soon after initiation of therapy and may be irreversible. If symptoms of peripheral neuropathy including pain, burning, tingling, numbness and/or weakness develop, patients should immediately discontinue Factive and contact their physician.
Central nervous system effects (for example, convulsions, dizziness, lightheadedness, increased intracranial pressure):
Inform patients that convulsions have been reported in patients receiving fluoroquinolones, including Factive. Patients should notify their physician before taking Factive if they have a history of convulsions, seizures, or epilepsy; Inform patients that other central nervous system problems such as tremors, restlessness, lightheadedness, confusion and hallucinations may occur rarely.
Exacerbation of Myasthenia Gravis: Inform patients that fluoroquinolones like Factive may cause worsening of myasthenia gravis symptoms, including muscle weakness and breathing problems. Patients should call their healthcare provider right away if they have any worsening muscle weakness or breathing problems.
Hypersensitivity Reactions: Inform patients that Factive may be associated with hypersensitivity reactions, including anaphylactic reactions, even following a single dose; patients should immediately discontinue the drug at the sign of a rash or other allergic reaction and seek medical care; Inform patients that Factive has been associated with rash and hives. Rash occurs more commonly in those under 40, especially women and in women on hormone replacement therapy. The incidence of rash increases with duration more than 5 days and particularly longer than 7 days. Patients should discontinue Factive and call their healthcare provider if they develop a rash.
Diarrhea: Inform patients that diarrhea is a common problem caused by antibiotics which usually ends when the antibiotic is discontinued. Sometimes after starting treatment with antibiotics, patients can develop watery and bloody stools (with or without stomach cramps and fever) even as late as two or more months after having taken the last dose of the antibiotic. If this occurs, patients should contact their physician as soon as possible.
Prolongation of the QT interval: inform patients of the following: that Factive may cause changes in the electrocardiogram (QTc interval prolongation); that Factive should be avoided in patients receiving Class IA (e.g., quinidine, procainamide) or Class III (e.g., amiodarone, sotalol) antiarrhythmic agents; that Factive should be used with caution in patients receiving drugs that affect the QTc interval such as cisapride, erythromycin, antipsychotics, and tricyclic antidepressants; to inform their physician of any personal or family history of QTc prolongation or proarrhythmic conditions such as hypokalemia, bradycardia, or recent myocardial ischemia; to contact their physician if they experience palpitations or fainting spells while taking Factive; that Factive may cause dizziness; if this occurs, patients should not operate an automobile or machinery or engage in activities requiring mental alertness or coordination.
Photosensitivity/Phototoxicity: Inform patients that photosensitivity/phototoxicity has been reported in patients receiving quinolones. Patients should minimize or avoid exposure to natural or artificial sunlight (tanning beds or UVA/B treatment) while taking quinolones. If patients need to be outdoors while using quinolones, they should wear loose-fitting clothes that protect skin from sun exposure and discuss other sun protection measures with their physician. If a sunburn-like reaction or skin eruption occurs, patients should contact their physician.
Other Information: Advise Patients: that increases of the International Normalized Ratio (INR), or prothrombin time (PT), and/or clinical episodes of bleeding have been noted with concurrent administration of warfarin or its derivatives, and Factive. Patients should notify their physicians if they are taking warfarin or its derivatives; to inform their physician of any other medications when taken concurrently with Factive, including over-the-counter medications and dietary supplements; that Factive may be taken with or without meals to drink fluids liberally; not to take antacids containing magnesium and/or aluminum or products containing ferrous sulfate (iron), multivitamin preparations containing zinc or other metal cations, or Videx (didanosine) chewable/buffered tablets or the pediatric powder for oral solution within 3 hours before or 2 hours after taking Factive tablets; that Factive should be taken at least 2 hours before sucralfate; that antibacterial drugs including Factive should only be used to treat bacterial infections. They do not treat viral infections (e.g., the common cold). When Factive is prescribed to treat a bacterial infection, patients should be told that although it is common to feel better early in the course of therapy, the medication should be taken exactly as directed. Skipping doses or not completing the full course of therapy may (1) decrease effectiveness of the immediate treatment and (2) increase the likelihood that bacteria will develop resistance and will not be treatable by Factive or other antibacterial drugs in the future.
Effects on ability to drive and use machines: CNS effects have been seen rarely in clinical trials with Factive. However, as with all drugs, patients should observe their reaction to Factive and, if affected, should not drive or operate machinery.
Hepatic Effects: Liver enzyme elevations (increased ALT and/or AST) occurred at similar rates in patients receiving Factive 320 mg daily relative to comparator antimicrobial agents (ciprofloxacin, levofloxacin, clarithromycin/cefuroxime axetil, amoxicillin/clavulanate potassium, and ofloxacin). In patients who received gemifloxacin at doses of 480 mg per day or greater there was an increased incidence of elevations in liver enzymes.
There were no clinical symptoms associated with these liver enzyme elevations. The liver enzyme elevations resolved following cessation of therapy. The recommended dose of Factive 320 mg daily should not be exceeded and the recommended length of therapy should not be exceeded.
Renal Effects: Alteration of the dosage regimen is necessary for patients with impairment of renal function (creatinine clearance ≤40 mL/min). Adequate hydration of patients receiving Factive should be maintained to prevent the formation of a highly concentrated urine.
Use in Children: Safety and effectiveness in children and adolescents less than 18 years of age have not been established. Fluoroquinolones including gemifloxacin cause arthropathy and osteochondrosis in immature animals.
Use in the Elderly: In clinical studies of FACTIVE, no significant differences in safety and effectiveness was observed between geriatric subjects and younger subjects. In adult subjects, the pharmacokinetics of FACTIVE are not affected by age. Geriatric patients are at increased risk for developing severe tendon disorders including tendon rupture when being treated with a fluoroquinolone such as FACTIVE. This risk is further increased in patients receiving concomitant corticosteroid therapy.
Epidemiologic studies reported an increased rate of aortic aneurysm/dissection within two months following use of fluoroquinolones, particularly in elderly patients. Elderly patients may be more susceptible to drug-associated effects on the QT interval.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image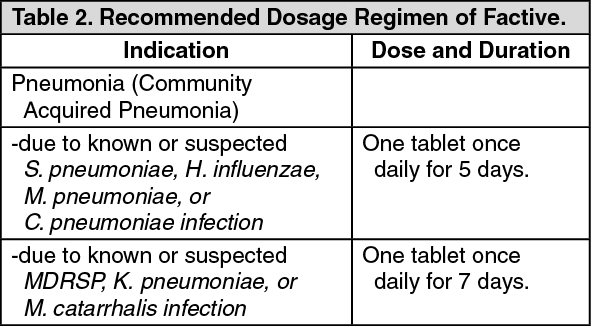 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image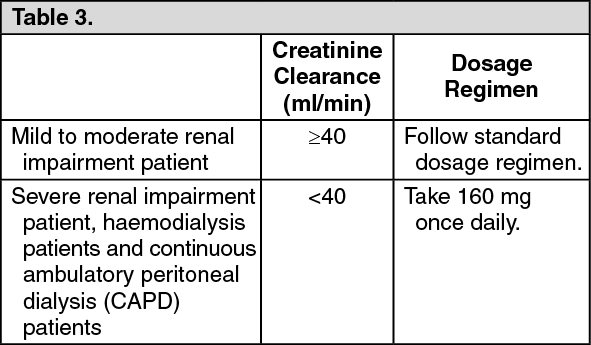 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out
