Adverse Drug Reaction Overview: Very common adverse events occurring in ≥ 10% of infants who received BLES (bovine lipid extract surfactant), in descending order of frequency, were patent ductus arteriosus, decreased post-dose pulmonary function values, intraventricular haemorrhage of all grades, sepsis, retinopathy of prematurity, bradycardia and severe intraventricular haemorrhage.
Common adverse events occurring in ≥ 1% and < 10% of infants who received BLES, in descending order of frequency, were pulmonary interstitial emphysema, periventricular leukomalacia, pneumothorax, pulmonary haemorrhage, endotracheal tube complications, necrotizing enterocolitis, respiratory acidosis, convulsions, hypotension, apnoea, hydrocephalus and pneumonia.
Due to the rapid effect of BLES on lung compliance and oxygenation, infants should be monitored for respiratory parameters and any of the common adverse events.
Clinical Trial Adverse Drug Reaction: Because clinical trials are conducted under very specific conditions, the adverse drug reaction rates observed in practice and should not be compared to the rates in the clinical trials of another drug. Adverse drug reaction information from clinical trials is useful for identifying drug-related adverse and for approximating rates.
In a double-blinded, comparative, multicentre clinical trial comparing the safety and efficacy of BLES and Exosurf Neonatal (colfosceril palmitate; Glaxo Wellcome), 568 infants received BLES and 565 received Exosurf for rescue treatment of NRDS.
Adverse events occurring in ≥ 1% of instants treated with BLES are summarized by body system and in order of decreasing frequency in Table 6, as follows. The incidence of these events in Exosurf -treated infants is provided for comparison. (See Table 6.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
The most frequent events reported to occur in either treatment group were patent ductus arteriosus in almost half of the infants, and decreased pulmonary in almost half on the infants, and decreases pulmonary function (defined as incidences of a fall in saturation or oxygenation, or an increase in CO2 value after dosing) in approximately one third of infants. These events occurred with similar frequency in either treatment group, and are anticipated complications when infants in distress and handled.
Sepsis and pneumonia occurred significantly more frequently in BLES -treated infants than in those who received Exosurf. Not with standing this higher incidence of sepsis, death due to infections was comparable between the two arms of the study.
Although the incidence of pulmonary haemorrhage was low (<1%) within the first two hours after dosing, it was observed to increase to 8% before discharge from intensive care. This was not significantly different from the incidence of pulmonary haemorrhage with Exosurf. For the 750-1250 gram birth weight group receiving BLES, 7 of 32 deaths (22%) were attributed to pulmonary haemorrhage.
There was a significantly greater incidence of respiratory acidosis following treatment with BLES. All incidences of respiratory acidosis occurred within two hours of dosing, and almost all incidences following either surfactant occurred at one study centre, perhaps due to too rapid weaning of the ventilator pressure and rate with decreased minute ventilation.
Significantly fewer infants who received BLES developed pulmonary interstitial emphysema or pneumothorax than did those who were treated with Exosurf. This may reflect the increased ventilator requirements of infants who received Exosurf. Thus, a reduction in ventilator pressure following treatment with BLES may protect infants from pulmonary air leaks.
Table 7, as follows, summarizes the adverse events that were reported to occur within two hours post-dose, in ≥1% of infants treated with BLES. The incidence of these events in Exosurf-treated infants is provided for comparison. (See Table 7.)
Click on icon to see table/diagram/image
Decreased pulmonary function (reported incidences of a fall in saturation or oxygenation, or an increase in CO
2 values), bradycardia and endotracheal tube complications occurred with the same frequency in each treatment group, and are commonly associated with handling and treatment of premature infants. As discussed previously, respiratory acidosis occurred, for the most part, at one site and may have been due to inadequate monitoring of lung compliance at that site.
Other adverse events that were reported to occur within two hours afters administration of BLES, but a frequency of <1% were: acidosis; hypertension; hypotension; hypoxia; patent ductus arteriosus; pneumonia; pneumothorax; and pulmonary haemorrhage.
Less Common Clinical Trial Adverse Drug Reactions: Uncommon adverse events that were reported to occur in < 1% of infants treated with BLES were:
Infections and infestations: miscellaneous infections other than pneumonia.
Blood and lymphatic system: neonatal coagulation disorder, neonatal jaundice; thrombocytopenia.
Endocrine disorders: hypercalcaemia; hypoglycaemia.
Metabolism and nutritional: acidosis; hyperkalemia.
Nervous system disorders: abnormal electroencephalogram; cerebral infarction; encephalopathy; ependymitis; meningitis.
Cardiac disorders: cardiac arrest; cardiomegaly; cor pulmonale; hypertrophic cardiomyopathy; pneumopericardium; pulmonary oedema; pulmonary valve stenosis; supraventricular tachycardia.
Vascular disorders: haemorrhage; hypertension.
Respiratory disorders: asphyxia; bronchopulmonary dysplasia; hypoxia; pulmonary hypertension.
Gastrointestinal disorders: enteritis; gastrointestinal haemorrhage; gastrointestinal reflux; ileus; intestinal perforation; pneumoperitoneum.
Hepato-biliary disorders: hepatomegaly.
Skin disorders: cellulitis.
Renal and urinary disorders: anuria; hydronephrosis; hydroureter; nephrocalcinosis.
General disorders: growth retardation; neonatal hypothermia.
Abnormal Hematologic and Clinical Chemistry Findings: Laboratory values were not collected in clinical trials. However, respiratory acidosis was reported as an adverse event in 4% of infants receiving BLES, occurring primarily at one study centre. Lung compliance and oxygenation should be monitored closely, as ventilation parameters may change rapidly after dosing (See Precautions).
Post-Market Adverse Drug Reactions: No new adverse reactions have been reported, nor has there been an increase in the incidence of known adverse reactions identified in the clinical trials.
Three infants at one site, who were administered very small aliquots of 1 mL at a time without rotation of the infant, developed pulmonary haemorrhage, intraventricular haemorrhage and/or periventricular leukomalacia, and died. The very small doses given without rotation may have led to uneven surfactant distribution and uneven lung compliance.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image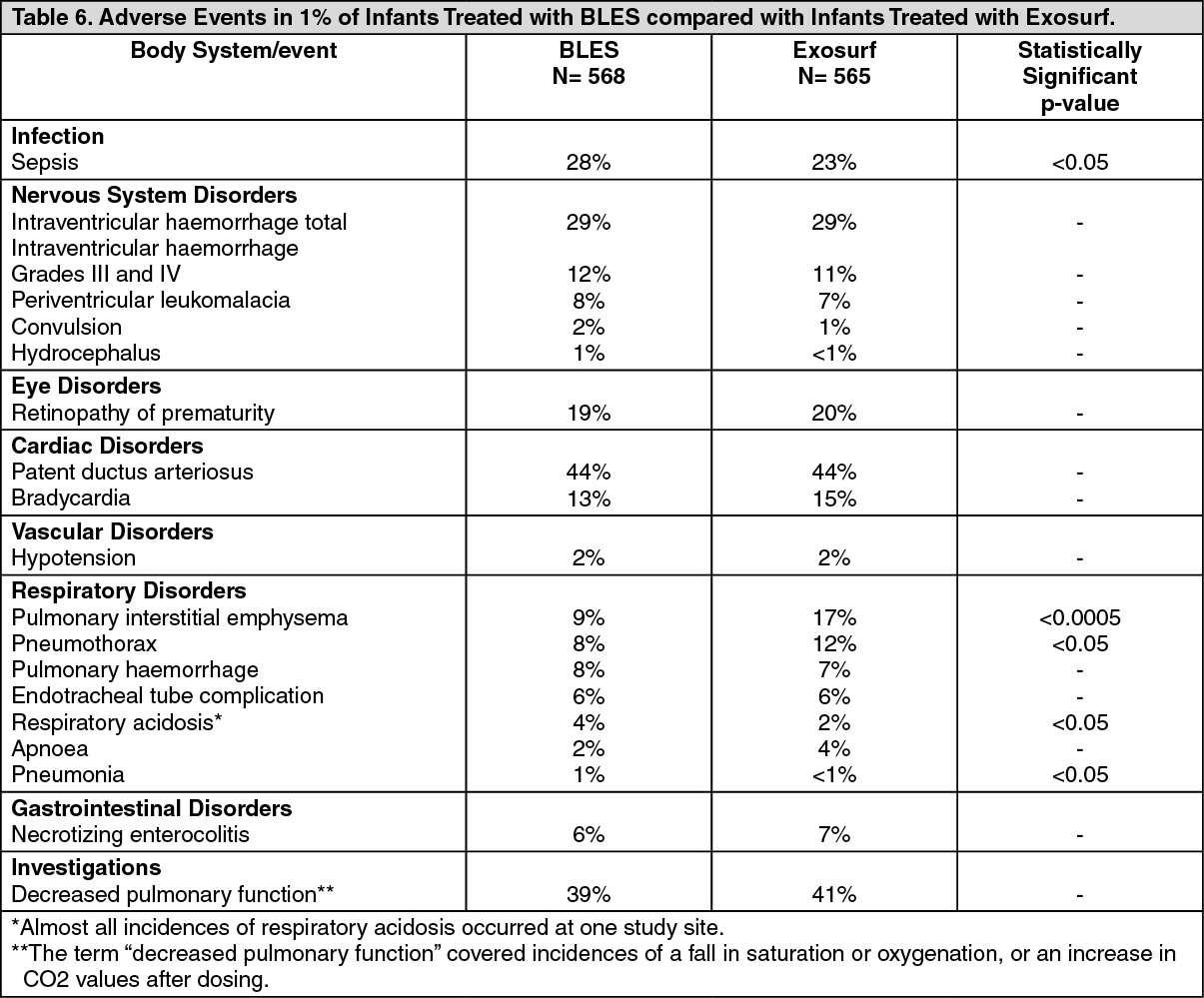 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image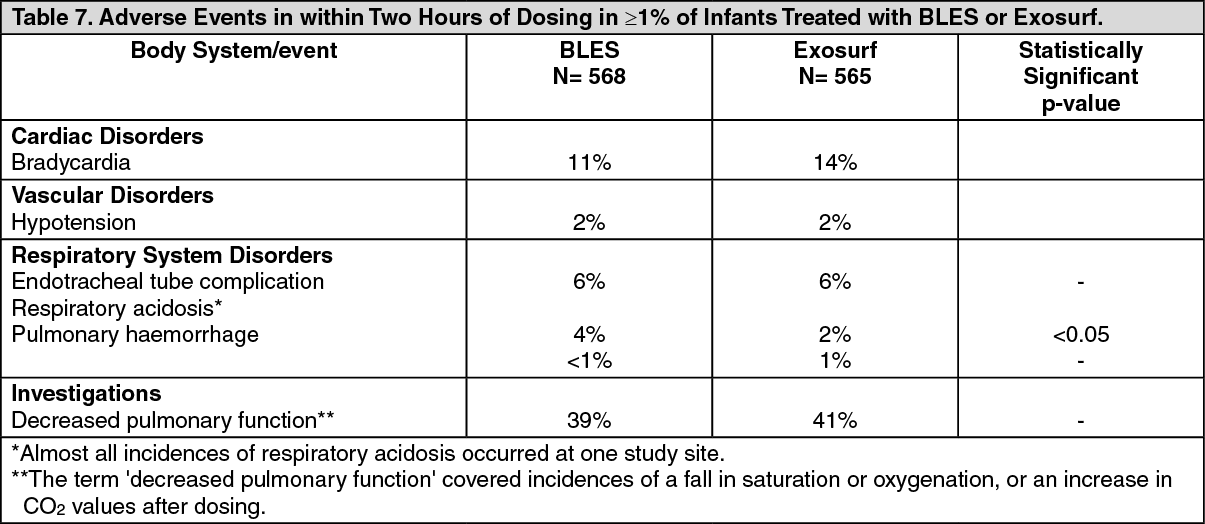 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out
