


 Sign Out
Sign Out

Dosing Considerations: BLES (bovine lipid extract surfactant) is intended for intratracheal instillation only after an endotracheal airway has been established.
BLES does not require reconstitution or filtering before use. Vials are for single use only, to ensure sterility. Once at room temperature, gently swirl or invert the vial to suspend the lipid and disperse any agglomerates. Inspect the vial for homogeneity. It is normal for warmed vials to have an even dispersion of fine but visible flecks of lipid. Contents should appear as an off-white to light yellow suspension. If contents are a darker colour or will not disperse evenly, discard the vial. Report this and the lot number to the manufacturer.
BLES should be warmed to at least room temperature, but no higher than body temperature before being administered. Warming can be accomplished in the following ways (times are approximate): See Table 4.
 Click on icon to see table/diagram/image
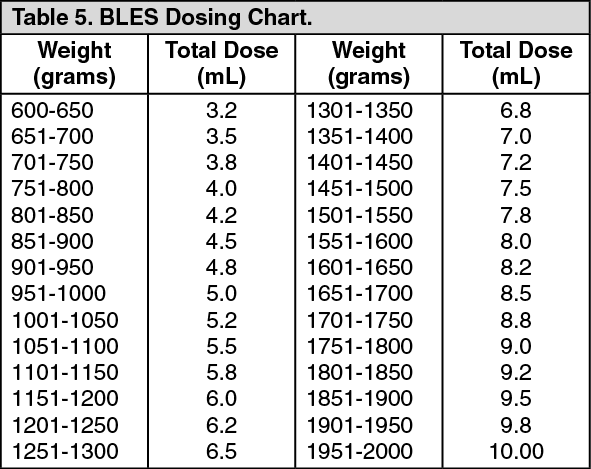
Click on icon to see table/diagram/imageRecommended Dosage: The recommended dosage of BLES is 5 mL/kg at 27 mg of phospholipids/mL which equals 135 mg phospholipid/kg. As many as 3 subsequent doses of BLES can be given within the first 5 days of life. See Repeat Doses as follows for details. Table 5 suggests the total dosage for a range of birth weights. (See Table 5.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageAdministration: Dosing Procedures: The infant should be suctioned and allowed to recover before commencing the procedure. Ensure proper placement of the endotracheal tube (ETT) via chest auscultation and radiograph, if available (1- 2 cm below the vocal cords, 1-2 cm above the carina). Do not instill BLES down the right mainstream bronchus.
Draw the full dose into a syringe with a large gauge needle, and fit the needle with a sterile #5 Fr feeding tube which has been cut to an appropriate length so that it will reach the distal tip of the ETT. Discharge the syringe to fill the feeding tube with surfactant. Briefly disconnect the infant from the ventilator so that the feeding tube may be threaded into the ETT. Alternately, to allow simultaneous mechanical ventilation or hand bagging, pass the feeding tube through the suction valve of a closed suctioning adaptor attached to the ETT.
Instill as a single bolus dose or up to three aliquots, as tolerated, with the infant supine for the first aliquot, then rotated to the left and right for subsequent aliquots. Instill each aliquot or dose over 2 to 3 seconds. After each aliquot is instilled, the infant should be ventilated manually for 30 seconds, using pressures sufficient to achieve good chest expansion before returning the infant to the ventilator. If the infant remains on mechanical ventilation during dosing, raise the pressure by 1 to 2 cm H2O, if necessary, to assist with emptying the ETT. Allow approximately 1-2 minutes recovery time after each aliquot. Ensure oxygen saturation readings are about 95% before commencing the next aliquot.
The volume of surfactant will rise in the ETT during administration. If the surfactant is slow to subside, interrupt administration and hand ventilate until the ETT is clear before continuing. If the surfactant fails to subside, investigate the possibility of a mucous plug. Small aliquots or a slow drip are not recommended, as this may lead to poor surfactant distribution and uneven lung compliance.
Monitoring after administration: Once instillation is complete, new mechanical ventilatory parameters need to be established according to the TcPO2/TcPCO2 readings, the oxygen saturation monitor and chest expansion.
TcPO2/TcPCO2 readings are preferred in infants of lower gestation (less than 32 weeks), and oxygen saturation readings preferred with older infants. Monitor tidal volume closely, as sudden lung compliance may occur without much chest movement. Start at pre-instillation settings and wean the pressures (PIP/PEEP), FiO2 and the ventilator rate, as indicated by the infant’s status. Follow-up blood gases one hour after dosing is a standard procedure for any infant who has received BLES (PaO2 should be between 60-70 torr, PaCO2 should be kept between 35-45 torr, and pH between 7.35 - 7.45). Avoid suctioning for 2 hours post-BLES, unless absolutely necessary. Due to the immediate effect of BLES on lung compliance and oxygenation (usually within 5 to 30 minutes), FiO2 should be decreased accordingly, to prevent hyperoxia. Chest expansion should be observed closely and ventilatory pressures (PIP/PEEP) decreased accordingly. High oxygen saturation levels (>95%) or high TcPO2/TcPCO2 readings (as confirmed by comparison to blood gas measurements) indicate the infant should be weaned off FiO2, ventilator rates and pressures. Blood gas readings should be 60 - 70 torr for PaO2 and 35 - 45 torr for PaCO2. Failure to wean appropriately may result in a pneumothorax.
Infants whose ventilation becomes markedly impaired during or shortly after dosing may have mucous plugging of the ETT, particularly if pulmonary secretions were prominent prior to drug administration. In addition, surfactant may promote the movement of resident mucus. If suctioning is unsuccessful in removing the obstruction, the blocked ETT should be replaced immediately.
Repeat Doses: Neonates can receive up to 3 additional doses of BLES within the first 5 days of life. The criteria for an additional dose are a positive response to the previous dose, and an increase in respiratory support as signalled by a gradual increase in FiO2. This increase must be at least 10% greater than the FiO2 required after the initial response to the previous dose of BLES.
All infants exhibiting respiratory deterioration should be evaluated for a patent ductus arteriosus (PDA), pneumothorax and pulmonary haemorrhage before retreatment with BLES. The regimen for repeat doses is the same as for the initial dose. See Dosing Procedures as previously mentioned for details.