


 Sign Out
Sign Out


Pharmacology: Pharmacodynamics: Mechanism of action: BeneFIX contains recombinant coagulation factor IX, (nonacog alfa). Recombinant coagulation factor IX is a single chain glycoprotein with an approximate molecular mass of 55,000 Daltons that is a member of the serine protease family of vitamin K-dependent coagulation factors. Recombinant coagulation factor IX is a recombinant DNA-based protein therapeutic, which has structural and functional characteristics comparable to endogenous factor IX. Factor IX is activated by factor VII/tissue factor complex in the extrinsic pathway as well as factor XIa in the intrinsic coagulation pathway activate factor IX. Activated factor IX, in combination with activated factor VIII, activates factor X. This results ultimately in the conversion of prothrombin to thrombin. Thrombin then converts fibrinogen into fibrin and a clot can be formed. Factor IX activity is absent or greatly reduced in patients with hemophilia B and substitution therapy may be required.
Hemophilia B is a sex-linked hereditary disorder of blood coagulation due to decreased levels of factor IX and results in profuse bleeding into joints, muscles or internal organs, either spontaneously or as a result of accidental or surgical trauma. By replacement therapy the plasma levels of factor IX is increased, thereby enabling a temporary correction of the factor deficiency and correction of the bleeding tendencies.
Clinical trials data on efficacy: Text as follows is from studies using Previous Formulation BeneFIX and is also applicable to Reformulated BeneFIX.
In 4 clinical studies of BeneFIX, a total of 128 subjects (56 previously treated patients [PTPs], 9 subjects participating only in the surgical study, and 63 previously untreated patients [PUPs]) received more than 28 million IU administered over a period of up to 64 months. The studies included 121 HIV-negative and 7 HIV-positive subjects.
Fifty-six PTPs received approximately 20.9 million IU of BeneFIX in two clinical studies. The median number of exposure days was 83.5. These PTPs who were treated for bleeding episodes on an on-demand basis or for the prevention of bleeds were followed over a median interval of 24 months (range 1 to 29 months; mean 23.4 ± 5.34 months). Fifty-five of these PTPs received a median of 42.8 IU/kg (range 6.5 to 224.6 IU/kg; mean 46.6 ± 23.5 IU/kg) per infusion for bleeding episodes. All subjects were evaluable for efficacy. One subject discontinued the study after one month of treatment due to bleeding episodes that were difficult to control; he did not have a detectable inhibitor. The subject's dose had not been adequately titrated. The remaining 55 subjects were treated successfully. Bleeding episodes that were managed successfully included hemarthroses and bleeding in soft tissue and muscle. Data concerning the severity of bleeding episodes were not reported. Eighty-eight percent of the total infusions administered for bleeding episodes were rated as providing an "excellent" or "good" response. Eighty-one percent of all bleeding episodes were managed with a single infusion of BeneFIX. One subject developed a low-titer, transient inhibitor (maximum titer 1.5 BU). This subject had previously received plasma-derived products without a history of inhibitor development. He was able to continue treatment with BeneFIX with no anamnestic rise in inhibitor or anaphylaxis; however, increased frequency of BeneFIX administration was required; subsequently, the subject's factor IX inhibitor and its effect on the half-life of BeneFIX resolved.
Forty-one of the subjects had measurements of fibrinopeptide A and prothrombin fragment 1 + 2 prior to infusion, 4 to 8 hours and then 24 hours following the infusion. Twenty-nine of the subjects had elevations in fibrinopeptide A with a maximum value of 35.3 nmol/L (22 of the 29 subjects had elevated baseline values). Ten of the subjects had elevated prothrombin fragment 1 + 2 with a maximum value of 1.82 nmol/L (3 of the 10 subjects had elevated baseline values).
Prophylaxis: A total of 20 PTPs were treated with BeneFIX for secondary prophylaxis (the regular administration of FIX replacement therapy to prevent bleeding in patients who may have already demonstrated clinical evidence of hemophilic arthropathy or joint disease) at some regular interval during the study with a mean of 2.0 infusions per week. Nineteen subjects were administered BeneFIX for routine secondary prophylaxis (at least twice weekly) for a total of 345 patient-months with a median follow-up period of 24 months per subject. The average dose used by these 19 subjects was 40.3 IU/kg, ranging from 13 to 78 IU/kg. One additional subject was treated weekly, using an average dose of 33.3 IU/kg, over a period of 21 months. Ninety-three percent of the responses were rated as "excellent" or "effective". These 20 PTPs received a total of 2,985 infusions of BeneFIX for routine prophylaxis. Seven of these PTPs experienced a total of 26 spontaneous bleeding episodes within 48 hours after an infusion.
Management of hemostasis was evaluated in the surgical setting. Thirty-six surgical procedures have been performed in 28 subjects. Thirteen (13) minor surgical procedures were performed in 12 subjects, including 7 dental procedures, 1 punch biopsy of the skin, 1 cyst removal, 1 male sterilization, 1 nevus ablation, and 2 ingrown toenail removals. Twenty-three (23) major surgical procedures were performed in 19 subjects, including a liver transplant, splenectomy, 3 inguinal hernia repairs, 11 orthopedic procedures, a calf-debridement and 6 complicated dental extractions.
Twenty-three (23) subjects underwent 27 surgical procedures with a pulse-replacement regimen. The mean perioperative (preoperative and intraoperative) dose for these procedures was 85 ± 32.8 IU/kg (range 25-154.9 IU/kg). The mean total post-operative (inpatient and outpatient) dose was 63.1 ± 22.0 IU/kg (range 28.6-129.0).
Total BeneFIX coverage during the surgical period for the major procedures ranged from 4,230 to 385,800 IU. The pre-operative dose for the major procedures ranged from 75 to 155 IU/kg. Nine of the major surgical procedures were performed in 8 subjects using a continuous infusion regimen. Following pre-operative bolus doses (94.1 -144.5 IU/kg), continuous infusion of BeneFIX was administered at a median rate of 6.7 IU/kg/hr (range of average rates: 4.3-8.6 IU/kg/hr; mean 6.4 ± 1.5 IU/kg/hr) for a median duration of 5 days (range 1-11 days; mean 4.9 ± 3.1). Six of the 8 subjects who had received continuous infusion of BeneFIX in conjunction with major surgeries were switched over to intermittent pulse regimens at a median dose of 56.3 IU/kg (range 33.6-89.1 IU/kg; mean 57.8 ± 18.1 IU/kg SD) for a median of 3.5 exposure days (range 1-5 days, mean 3.3 ± 1.4 SD) during the post-operative period. Although circulating factor IX levels targeted to restore and maintain hemostasis were achieved with both pulse replacement and continuous infusion regimens, clinical trial experience with continuous infusion of BeneFIX for surgical prophylaxis in hemophilia B has been too limited to establish the safety and clinical efficacy of administration of the product by continuous infusion. Subjects administered BeneFIX by continuous infusion for surgical prophylaxis also received intermittent bolus infusions of the product.
Among the surgery subjects, the median increase in circulating factor IX activity was 0.7 IU/dL per IU/kg infused (range 0.3-1.2 IU/dL; mean 0.8 ± 0.2 IU/dL per IU/kg). The median elimination halflife for the surgery subjects was 19.4 hours (range 10-37 hours; mean 21.3 ± 8.1 hours).
Hemostasis was maintained throughout the surgical period; however, one subject required evacuation of a surgical wound site hematoma, and another subject who received BeneFIX after a tooth extraction required further surgical intervention due to oozing at the extraction site. There was no clinical evidence of thrombotic complications in any of the subjects. In seven subjects for whom fibrinopeptide A and prothrombin fragment 1 + 2 were measured pre-infusion, at 4 to 8 hours, and then daily up to 96 hours, there was no evidence of significant increase in coagulation activation. Data from two other subjects were judged to be not evaluable.
Sixty-three PUPs received approximately 6.2 million IU of BeneFIX in an open-label safety and efficacy study over 89 median exposure days. These PUPs were followed over a median interval of 37 months (range 4 to 64 months; mean 38.1 ± 16.4 months). Fifty-four of these PUPs received a median dose of 62.7 IU/kg (range 8.2 to 292.0 IU/kg; mean 75.6 ± 42.5 IU/kg) per infusion for bleeding episodes. Data concerning the severity of bleeding episodes were not reported. Ninety-four percent of the infusions administered to initiate treatment of bleeding were rated as providing "excellent" or "good" response.
Seventy-five percent of all bleeding episodes were managed with a single infusion of BeneFIX. Three of these 54 subjects were not successfully treated, including one episode in a subject due to delayed time to infusion and insufficient dosing, and in 2 subjects due to inhibitor formation. One subject developed a high-titer inhibitor (maximum titer 42 BU) on exposure day 7. A second subject developed a high-titer inhibitor (maximum titer 18 BU) after 15 exposure days. Both subjects experienced allergic manifestations in temporal association with their inhibitor development.
Thirty-two PUPs administered BeneFIX for routine prophylaxis. Twenty-four PUPs administered BeneFIX at least twice weekly for a total of 2,587 infusions. The mean dose per infusion was 72.5 ± 37.1 IU/kg, and the mean duration of prophylaxis was 13.4 ± 8.2 months. Eight PUPs administered BeneFIX once weekly for a total of 571 infusions. The mean dose per infusion was 75.9 ± 17.9 IU/kg, and the mean duration of prophylaxis was 17.6 ± 7.4 months. Five PUPs experienced a total of 6 spontaneous bleeding episodes within 48 hours after an infusion.
Twenty-three PUPs received BeneFIX for surgical prophylaxis in 30 surgical procedures. All surgical procedures were minor, except 2 hernia repairs. The preoperative bolus dose ranged from 32.3 IU/kg to 247.2 IU/kg. The perioperative total dose ranged from 385 to 23,280 IU. Five of the surgical procedures were performed using a continuous infusion regimen over 3 to 5 days. Clinical trial experience with continuous infusion of BeneFIX for surgical prophylaxis in hemophilia B has been too limited to establish the safety and clinical efficacy of administration of the product by continuous infusion.
Pediatric population: Safety and efficacy have been demonstrated in previously treated and previously untreated pediatric patients. See Dosage & Administration.
For dosing information regarding use in children, see Dosage & Administration.
Pharmacokinetics: A single infusion of BeneFIX in patients (baseline data) with hemophilia B has shown mean ± SD recovery values, determined by age, 0.78 ± 0.23 IU/dL/IU/kg (range 0.4 to 1.4 IU/dL per IU/kg) for those ≥15 years old (n=37), and 0.68 ± 0.30 IU/dL per IU/kg (range 0.18 to 2.08 IU/dL per IU/kg) for those <15 years old (n=56).
In a randomized, cross-over pharmacokinetic study, BeneFIX reconstituted in 0.234% sodium chloride diluent was shown to be pharmacokinetically equivalent to the previously marketed BeneFIX (reconstituted with Sterile Water for Injection) in 24 PTP patients (≥12 years) at a dose of 75 IU/kg. In addition, pharmacokinetic parameters were followed up in 23 of the same PTP after repeated administration of BeneFIX for six months and found to be unchanged compared with those obtained at the initial evaluation. A summary of pharmacokinetic data are presented in Table 1: (See Table 1.)
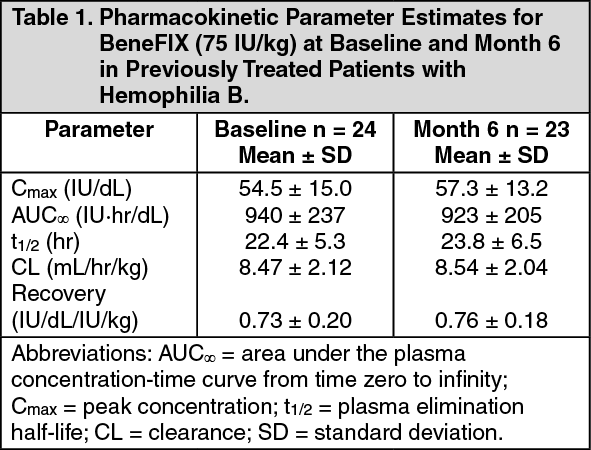 Click on icon to see table/diagram/image
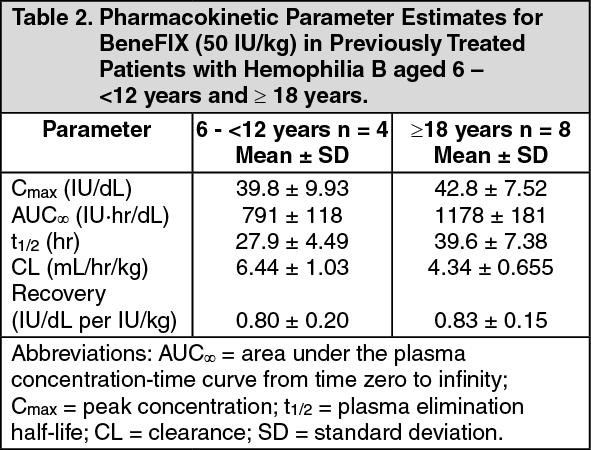
Click on icon to see table/diagram/imageA single-dose pharmacokinetic study reported a longer estimate of t1/2 when sample collection to measure factor IX activity (FIX) was extended to 96 hours. A summary of pharmacokinetic data is presented in Table 2. (See Table 2.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageToxicology: Preclinical Safety Data: BeneFIX has been shown to be non-mutagenic in the Ames assay and non-clastogenic in a chromosomal aberrations assay. No investigations on carcinogenesis or impairment of fertility have been conducted.