


 Sign Out
Sign Out


Pharmacology: Pharmacodynamics: Mechanism of action: Activated factor VIII acts as a cofactor for activated factor IX, accelerating the conversion of factor X to activated factor X. Activated factor X converts prothrombin into thrombin. Thrombin then converts fibrinogen into fibrin, and a clot is formed. Factor VIII activity is greatly reduced in patients with hemophilia A, and therefore replacement therapy is necessary. The administration of XYNTHA increases plasma levels of factor VIII activity and can temporarily correct the coagulation defect in these patients.
XYNTHA, recombinant coagulation factor VIII is a glycoprotein with an approximate molecular mass of 170,000 Da, consisting of 1,438 amino acids, which does not contain the non-functional B-domain. XYNTHA is a recombinant DNA-based substance that has functional characteristics comparable to those of endogenous factor VIII.
The factor VIII/von Willebrand factor complex consists of two molecules (factor VIII and von Willebrand factor) with different physiological functions. When infused into a hemophiliac patient, factor VIII binds to von Willebrand factor in the patient's circulation.
Hemophilia A is an X chromosome-linked hereditary disorder of blood coagulation due to decreased levels of factor VIII:C and results in bleeding into joints, muscles or internal organs, either spontaneously or as a result of accidental or surgical trauma. By replacement therapy the plasma levels of factor VIII are increased, thereby enabling a temporary correction of the factor deficiency and correction of the bleeding tendency.
Clinical trials data on efficacy: Immune tolerance induction: Data on immune tolerance induction (ITI) have been collected in patients with hemophilia A who had developed inhibitors to factor VIII. As part of the pivotal trial with ReFacto in PUPs, ITI data from 25 patients were reviewed (see Adverse Reactions). Of these 25 patients, 20 had a decrease in inhibitor titres to <0.6 BU/mL, of whom initially 11 of 15 had high titres (≥5 BU/mL) and 9 of 10 had low titres (<5 BU/mL). Out of 6 patients who developed low titre inhibitors in this study but did not receive ITI, 5 had similar titre decreases. No long-term outcome is available.
Pivotal data with XYNTHA: In a pivotal phase 3 study (Study 3082B2-310WW/CSR 66997), the efficacy of XYNTHA was evaluated in routine prophylaxis and on-demand treatment. Prophylaxis was to be initiated at a dose of 30 IU/kg given 3 times per week. The on-demand treatment dosing regimen was to be determined by the investigator. Ninety-four (94) PTPs with moderately severe or severe hemophilia A (factor VIII:C ≤2%) received at least 1 dose of XYNTHA and were included in the intent-to-treat (ITT) population. Eighty-nine (89) patients accrued at least 50 exposure days (EDs) to XYNTHA in the study.
Of the 94 patients in the ITT population, 30 patients with factor VIII:C ≤1% also participated in the double-blind, randomized, crossover PK period of the study and were included in the per-protocol population for analyses of pharmacokinetic equivalence versus another rFVIII product, Advate, and full PK characterization. The results of these analyses showed that XYNTHA is pharmacokinetically equivalent to Advate, and the pharmacokinetic profile of XYNTHA remained stable after 6 months of repeated use.
Intent-to-treat analysis of clinical efficacy variables in the open-label safety and efficacy period yielded similarly positive outcomes. All 94 patients received XYNTHA for routine prophylaxis; the median dose administered was 30.2 IU/kg (range 6.8 to 76.9 IU/kg). Most patients (57/94; 60.6%) reported no spontaneous bleeding while on routine prophylaxis. The median annualized bleeding rate (ABR) for all bleeding episodes was 1.9 (mean 3.9, range 0 to 42.1), indicating effective prevention of bleeding in the study population. Fifty-three (53) of 94 patients received XYNTHA for on-demand treatment; the median dose administered was 30.6 IU/kg (range 6.4 to 74.4 IU/kg). The majority of bleeding episodes (173/187; 92.5%) resolved with 1 or 2 infusions. This outcome was not restricted to any particular bleeding location, as similar efficacy was seen in bleeding occurring in joints, soft tissues/muscles, and other sites. A wide range of doses was used to initiate treatment of bleeding; however, the distribution of doses used to initiate treatment of bleeding was similar regardless of location of bleeding. Patients rated the majority of infusions used to initiate treatment of bleeding as either excellent or good (132/187; 70.6%). The incidence of less-than-expected therapeutic effect (LETE) occurred at a rate of 0.4% (25/6404 prophylactic infusions) when XYNTHA was administered for prophylaxis and 0.5% (1/187 bleeding episodes) when administered for on-demand treatment.
A pivotal phase 3 study (study 311) for surgical prophylaxis in patients with hemophilia A included PTPs with severe or moderately severe (factor VIII:C ≤2%) hemophilia A undergoing major surgical procedures who received XYNTHA. Thirty (30) patients were treated with XYNTHA and comprised the ITT population; 29 patients underwent major surgery and completed the study. Thirty (30) subjects were assigned to receive XYNTHA by bolus injection (BI; 22 patients) or by continuous infusion (CI; 8 patients) at the physician's discretion to support surgical hemostasis followed by inpatient and outpatient postoperative care. One subject assigned to CI received XYNTHA for a pre-surgery pharmacokinetic assessment only and subsequently elected not to undergo surgery. The 22 patients treated by BI received a total of 942 infusions (ranging from 16 to 72 infusions per patient) for a cumulative total dose of 2,037,386 IU of XYNTHA over 682 cumulative total exposure days (EDs) (ranging from 15 to 40 EDs per patient). The 8 patients assigned to treatment by CI, including 1 patient who received only 1 dose for PK assessment, received a total dose of 529,977 IU of XYNTHA over 204 total EDs (range 1 to 37 EDs per patient).
Of the 29 patients who underwent surgery, 25 were included in the efficacy evaluable population. Major surgical procedures for the 25 efficacy evaluable subjects were 11 total knee replacements, 1 hip replacement, 5 synovectomies, 1 left ulnar nerve transposition release, 1 ventral hernia repair/scar revision, 1 knee arthroscopy, 1 revision and debridement of the knee after a total knee replacement, 1 hip arthroplasty revision, 1 stapes replacement, 1 ankle arthrodesis, and 1 pseudotumor excision. For the 25 surgical subjects, investigator's ratings of the efficacy at the end of surgery and at the end of the initial postoperative period were excellent or good for all assessments, intraoperative blood loss was reported as normal or absent for all procedures. Thirteen of the 25 evaluable patients had blood loss in the postoperative period, and in 10 cases the postoperative blood loss was rated normal. In 3 cases, the postoperative blood loss was rated abnormal: 1 due to hemorrhage following surgical trauma to the epigastric artery, 1 due to an 800 mL blood loss after hip replacement surgery, and 1 after an elbow synovectomy where the blood loss could not be measured by the investigator.
Additional data with XYNTHA in pediatric population <16 years of age: The safety and efficacy of XYNTHA, and factor VIII:C pharmacokinetics after XYNTHA in children <16 years of age with moderately severe to severe hemophilia A (factor VIII:C ≤2%) were evaluated in an open-label study that compared (1) the efficacy of routine prophylaxis to on-demand treatment in a cohort of pediatric subjects <6 years of age, and (2) compared two routine prophylaxis regimens in a cohort of children <16 years of age.
51 subjects with at least 20 prior EDs to factor VIII products were enrolled and included in the ITT population. 50 subjects received at least 1 dose of XYNTHA, and 41 subjects completed the study.
9 pediatric subjects <6 years of age received on-demand treatment with XYNTHA at a median dose of 24 IU per kg for a 6-month period followed by routine prophylaxis regimen at a dose of 25 IU/kg every other day (EOD) for 12 months for 8 of these subjects. The median ABR observed during the on-demand treatment period was 34.0 (mean 47.0, range 0 to 92.4) compared to 0.6 (mean 1.5, range 0 to 6.2) while on the routine prophylaxis regimen (p=0.0040) (see Table 1).
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image42 pediatric subjects <16 years of age received either routine prophylaxis dosing regimen 45 IU/kg twice per week or 25 IU/kg every other day for 12 months before crossing over to receive the alternate regimen, and 35 subjects provided data for both regimens. Because the 90% confidence interval (CI) for the difference of (0.03, 2.22) was inside the prospectively defined equivalence limit of (-3.3), equivalent efficacy was established with respect to ABR for both regimens (mean±SD 3.3±5.3 compared to 2.2±4.1).
A total of 838 OD infusions were administered to treat the 562 bleeding episodes. The majority of bleeding episodes (518/562; 92.2%) resolved with 1 or 2 infusions. A total 526 (93.6%) bleeding episodes treated with study drug were rated "Excellent" or "Good" in their response to initial treatment (i.e., first infusion).
The incidence of LETE occurred at a rate of 0.16% (18/10927 prophylactic infusions) when XYNTHA was administered for prophylaxis and no occurrence when administered for on-demand treatment.
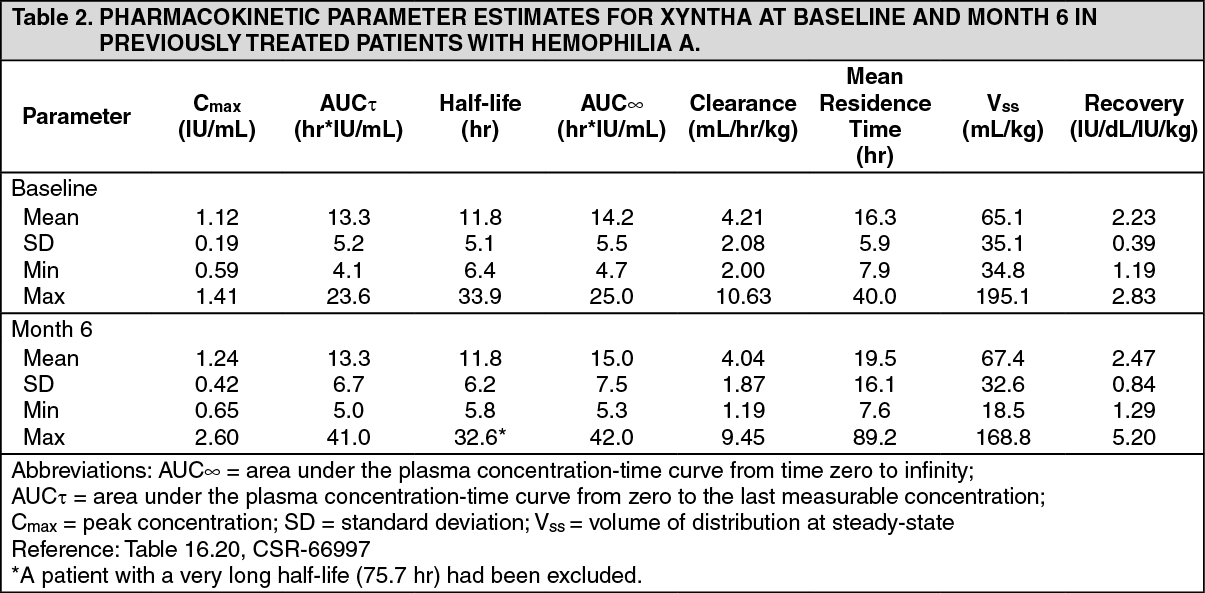
Pharmacokinetics: The pharmacokinetic parameters for XYNTHA were determined at baseline and followed-up in 25 PTPs (≥12 years) after repeated administration of XYNTHA for six months. These patients received a single infusion of 50 IU/kg of XYNTHA. No time-dependent changes in the pharmacokinetic properties of XYNTHA were observed (see Table 2).
 Click on icon to see table/diagram/image
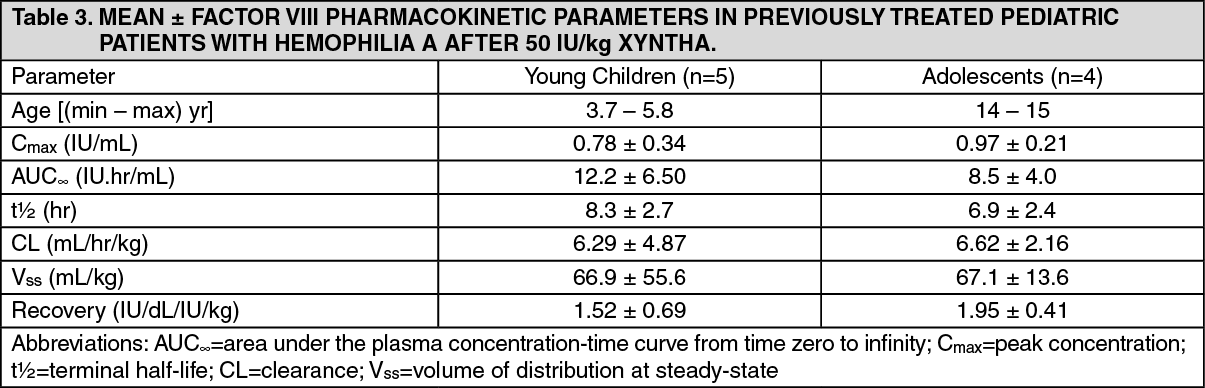
Click on icon to see table/diagram/imageTable 3 shows the pharmacokinetic parameters of nine children, four aged 14 or 15 years of age, who are also included in the summary for the adults as previously mentioned, along with five children aged 3.7 to 5.8 years after XYNTHA administration. Compared with adults, the half-life of XYNTHA is shorter in children and clearance (based on body weight) is approximately 40% higher in children. (See Table 3.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageTable 4 presents pharmacokinetic data from the clinical study (4433) on PTPs. (See Table 4.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageIn a ReFacto AF study (4434) of 19 PUPs, the recovery at the beginning of the study in the 17 children aged 28 days to less than 2 years was 1.32 ± 0.65 IU/dl per IU/kg and in the 2 children aged 2 to <6 years were 1.7 and 1.8 IU/dl per IU/kg. Except in cases where inhibitors were detected, the mean recovery was stable over time (6 visits during a 2-year period) and individual values ranged from 0 (in presence of inhibitor) to 2.7 IU/dl per IU/kg.
Toxicology: Preclinical safety data: No studies have been conducted with XYNTHA to assess its mutagenic or carcinogenic potential. XYNTHA has been shown to be comparable to the predecessor product ReFacto with respect to its biochemical and physicochemical properties, as well as its non-clinical in vivo pharmacology and toxicology. By inference, predecessor product ReFacto and XYNTHA would be expected to have equivalent mutagenic and carcinogenic potential. The predecessor product ReFacto has been shown to be nongenotoxic in the mouse micronucleus assay. No studies have been conducted in animals to assess impairment of fertility or fetal development.
In preclinical studies, XYNTHA was used to safely and effectively restore hemostasis. XYNTHA demonstrated a toxicological profile that was similar to the toxicological profile observed with the predecessor product ReFacto, which had in turn been shown to demonstrate a similar toxicological profile to a plasma-derived factor VIII product when tested in repeated dose toxicology studies in animals.