


 Sign Out
Sign Out


For posology, method of administration, and dose modifications of docetaxel, refer to the corresponding product information for docetaxel.
The recommended dose of OFEV is 200 mg twice daily administered approximately 12 hours apart, on days 2 to 21 of a standard 21-day docetaxel treatment cycle.
OFEV must not be taken on the same day of docetaxel chemotherapy administration (= day 1).
The recommended maximum daily dose of 400 mg should not be exceeded.
Patients may continue therapy with OFEV after discontinuation of docetaxel for as long as clinical benefit is observed or until unacceptable toxicity occurs.
Dosing in IPF/chronic fibrosing ILDs with a progressive phenotype/SSc-ILD: Treatment with OFEV should be initiated by physicians experienced in the diagnosis and treatment of conditions for which OFEV is indicated.
The recommended dose of OFEV is 150 mg twice daily administered approximately 12 hours apart.
The recommended maximum daily dose of 300 mg should not be exceeded.
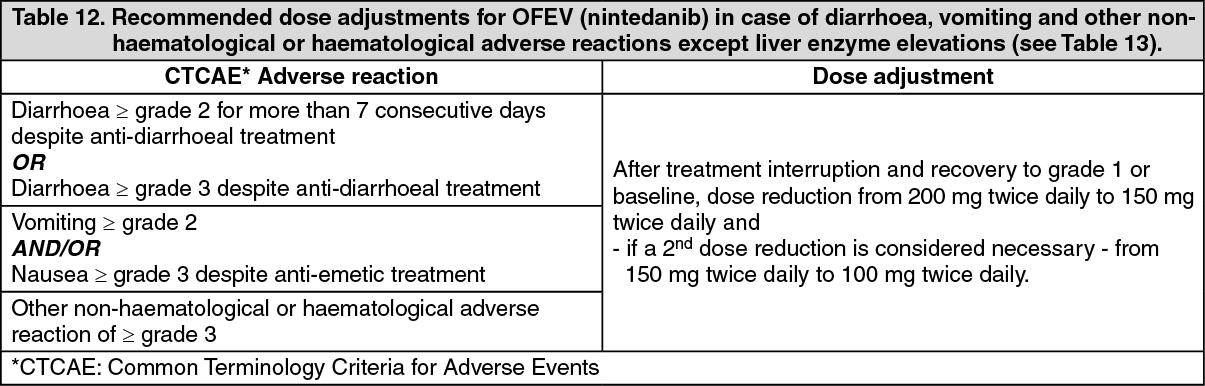
Dose adjustments: NSCLC: As initial measure for the management of adverse reactions (see Tables 12 and 13), treatment with nintedanib should be temporarily interrupted until the specific adverse reaction has resolved to levels that allow continuation of therapy (to grade 1 or baseline).
Nintedanib treatment may be resumed at a reduced dose. Dose adjustments in 100 mg steps per day (i.e. a 50 mg reduction per dosing) based on individual safety and tolerability are recommended as described in Table 12 and Table 13.
In case of further persistence of the adverse reaction(s), i.e. if a patient does not tolerate 100 mg twice daily, treatment with OFEV should be permanently discontinued. In case of specific elevations of aspartate aminotransferase (AST)/alanine aminotransferase (ALT) values to > 3 x upper limit normal (ULN) in conjunction with an increase of total bilirubin to ≥ 2 x ULN and alkaline phosphatase (ALKP) < 2 x ULN; (see Table 13) treatment with OFEV should be interrupted. Unless there is an alternative cause established, OFEV should be permanently discontinued (see Precautions). (See Tables 12 and 13.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image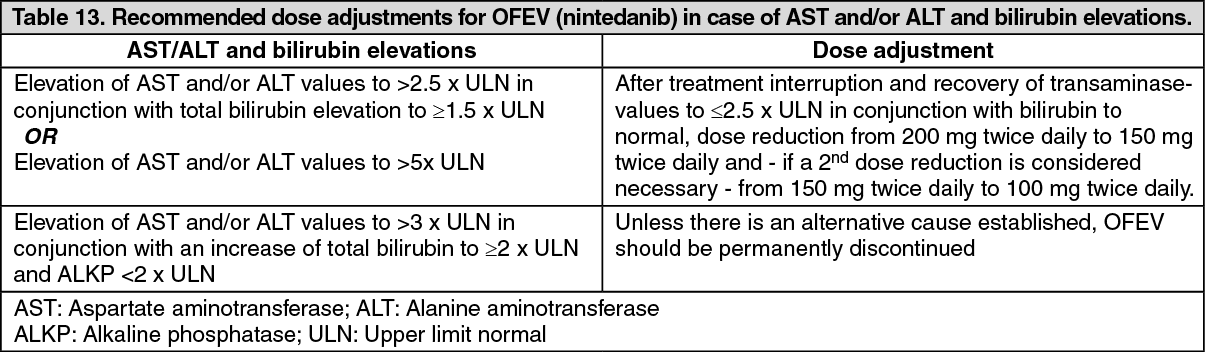 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageIPF/chronic fibrosing ILDs with a progressive phenotype/SSc-ILD: In addition to symptomatic treatment if applicable, the management of adverse reactions (see Precautions, Adverse Reactions) of OFEV may require dose reduction or temporary interruption until the specific adverse reaction resolves to levels that allow continuation of therapy. OFEV treatment may be resumed at the full dosage (150 mg twice daily) or at the reduced dosage (100 mg twice daily), which subsequently may be increased to the full dosage. If a patient does not tolerate 100 mg twice daily, treatment with OFEV should be discontinued.
Dose modifications or interruptions may be necessary for liver enzyme elevations. For aspartate aminotransferase (AST) or alanine aminotransferase (ALT) > 3 times to < 5 times the upper limit of normal (ULN) without signs of severe liver damage, interrupt treatment or reduce OFEV to 100mg twice daily. Once liver enzymes have returned to baseline values, treatment with OFEV may be reintroduced at a reduced dosage (100mg twice daily), which subsequently may be increased to the full dosage (150mg twice daily) [see Precautions, Adverse Reactions].
Special populations: Paediatric population: The safety and efficacy of OFEV in children aged 0-18 years have not been established.
Elderly patients (≥ 65 years): No overall differences in safety and efficacy were observed for elderly patients. No adjustment of the initial dosing is required on the basis of a patient's age (see Pharmacology: Pharmacokinetics under Actions). Patients ≥ 75 years may be more likely to require dose reduction to manage adverse effects.
Race: Based on population pharmacokinetic (-PK) analyses, no a priori dose adjustments of OFEV are necessary (see Special Populations under Precautions, Pharmacology: Pharmacokinetics under Actions). Safety data for Black patients are limited.
Body weight: Based on population PK analyses, no a priori dose adjustments of OFEV are necessary (see Pharmacology: Pharmacokinetics under Actions).
Renal impairment: Less than 1% of a single dose of nintedanib is excreted via the kidney (see Pharmacology: Pharmacokinetics under Actions). Adjustment of the starting dose in patients with mild to moderate renal impairment is not required. The safety, efficacy, and pharmacokinetics of nintedanib have not been studied in patients with severe renal impairment (< 30 ml/min CrCL).
Hepatic Impairment: IPF/chronic fibrosing ILDs with a progressive phenotype/SSc-ILD: Nintedanib is predominantly eliminated via biliary/faecal excretion (> 90%). Exposure increased in patients with hepatic impairment (Child Pugh A, Child Pugh B; see Pharmacology: Pharmacokinetics under Actions).
In patients with mild hepatic impairment (Child Pugh A), the recommended dose of OFEV is 100mg twice daily approximately 12 hours apart.
In patients with mild hepatic impairment (Child Pugh A), treatment interruption or discontinuation for management of adverse reactions should be considered.
The safety and efficacy of nintedanib have not been investigated in patients with hepatic impairment classified as Child Pugh B and C. Treatment of patients with moderate (Child Pugh B) and severe (Child Pugh C) hepatic impairment with OFEV is not recommended (see Pharmacology: Pharmacokinetics under Actions).
NSCLC: Nintedanib is predominantly eliminated via biliary/faecal excretion (> 90%). Exposure increased in patients with hepatic impairment (Child Pugh A, Child Pugh B; see Pharmacology: Pharmacokinetics under Actions).
No adjustment of the starting dose is needed for patients with mild hepatic impairment (Child Pugh A) based on clinical data.
Limited safety data available from 9 patients with moderate hepatic impairment (Child Pugh B) are insufficient to characterize this population.
The safety, efficacy and pharmacokinetics of nintedanib have not been investigated in patients with severe hepatic impairment (Child Pugh C). Treatment of patients with moderate (Child Pugh B) and severe (Child Pugh C) hepatic impairment with OFEV is not recommended (see Precautions and Pharmacology: Pharmacokinetics under Actions).
Method of Administration: OFEV capsules should be taken orally, preferably with food, swallowed whole with water, and should not be chewed. If a dose is missed, administration should resume at the next scheduled time at the recommended dose. If a dose is missed, the patient should not be given an additional dose.
OFEV capsules may be taken with a small amount (teaspoonful) of cold or room temperature soft food, such as apple sauce or chocolate pudding, and must be swallowed unchewed immediately, to ensure the capsule stays intact.
The capsule should not be opened or crushed. If contact with the content of the capsule occurs, hands should be washed immediately and thoroughly.