


 Sign Out
Sign Out

Pharmacology: Pharmacodynamics: Mechanism of action: Cladribine is a nucleoside analogue of deoxyadenosine. A chlorine substitution in the purine ring protects cladribine from degradation by adenosine deaminase, increasing the intracellular residence time of the cladribine prodrug.
Subsequent phosphorylation of cladribine to its active triphosphate form, 2-chlorodeoxyadenosine triphosphate (Cd-ATP), is particularly efficiently achieved in lymphocytes, due to their constitutively high deoxycytidine kinase (DCK) and relatively low 5'-nucleotidase (5'-NTase) levels. A high DCK to 5'-NTase ratio favours the accumulation of Cd-ATP, making lymphocytes particularly susceptible to cell death. As a result of a lower DCK/5'-NTase ratio other bone marrow derived cells are less affected than lymphocytes.
DCK is the rate limiting enzyme for conversion of the cladribine prodrug into its active triphosphate form, leading to selective depletion of dividing and non-dividing T and B cells.
The primary apoptosis-inducing mechanism of action of Cd-ATP has direct and indirect actions on DNA synthesis and mitochondrial function. In dividing cells, Cd-ATP interferes with DNA synthesis via inhibition of ribonucleotide reductase and competes with deoxyadenosine triphosphate for incorporation into DNA by DNA polymerases. In resting cells cladribine causes DNA single-strand breaks, rapid nicotinamide adenine dinucleotide consumption, ATP depletion and cell death. There is evidence that cladribine can also cause direct caspase-dependent and -independent apoptosis via the release of cytochrome c and apoptosis-inducing factor into the cytosol of non-dividing cells.
MS pathology involves a complex chain of events in which different immune cell types, including autoreactive T and B cells play a key role. The mechanism by which cladribine exerts its therapeutic effects in MS is not fully elucidated but its predominant effect on B and T lymphocytes is thought to interrupt the cascade of immune events central to MS.
Variations in the expression levels of DCK and 5'-NTases between immune cell subtypes may explain differences in immune cell sensitivity to cladribine. Because of these expression levels, cells of the innate immune system are less affected than cells of the adaptive immune system.
Pharmacodynamic effects: Cladribine has been shown to exert long-lasting effects by preferentially targeting lymphocytes and the autoimmune processes involved in the pathophysiology of MS.
Across studies, the largest proportion of patients with grade 3 or 4 lymphopenia (< 500 to 200 cells/mm3 or < 200 cells/mm3) was seen 2 months after the first cladribine dose in each year, indicating a time gap between cladribine plasma concentrations and the maximum haematological effect.
Across clinical studies, data with the proposed cumulative dose of 3.5 mg/kg body weight show a gradual improvement in the median lymphocyte counts back to the normal range at week 84 from the first dose of cladribine (approximately 30 weeks after the last dose of cladribine). The lymphocyte counts of more than 75% of patients returned to the normal range by week 144 from the first dose of cladribine (approximately 90 weeks after the last dose of cladribine).
Treatment with oral cladribine leads to rapid reductions in circulating CD4+ and CD8+ T cells. CD8+ T cells have a less pronounced decrease and a faster recovery than CD4+ T cells, resulting in a temporarily decreased CD4:CD8 ratio. Cladribine reduces CD19+ B cells and CD19+/CD56+ natural killer cells, which also recover faster than CD4+ T cells.
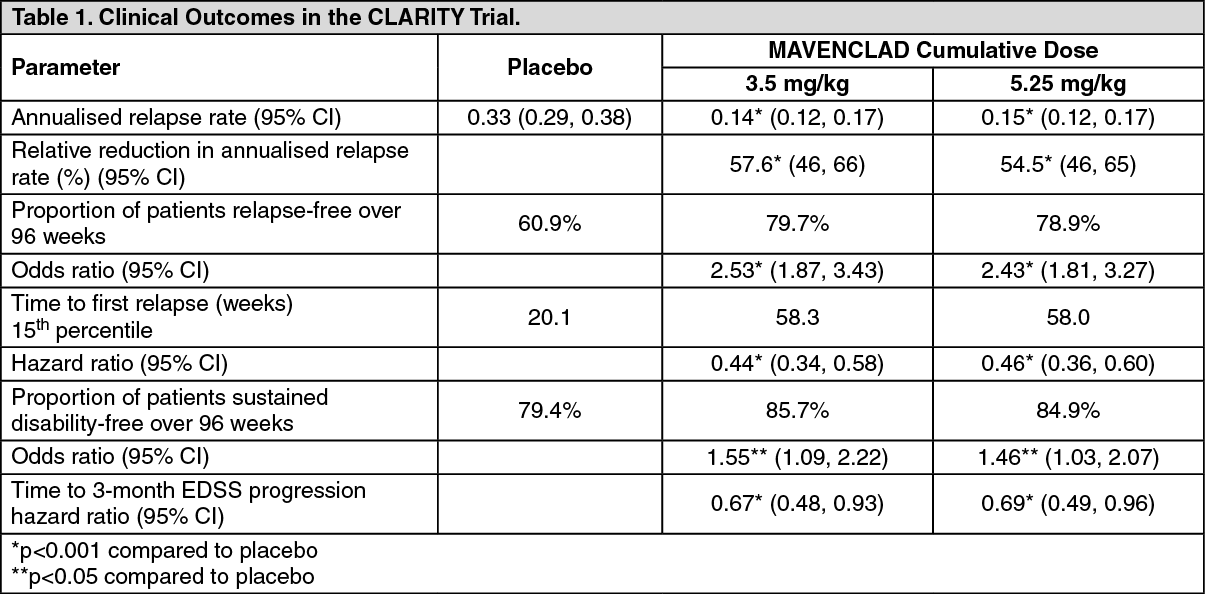
Clinical efficacy and safety: Efficacy and safety of MAVENCLAD tablets for oral use were evaluated in relapsing-remitting MS in the Cladribine Tablets Treating MS Orally (CLARITY) trial, a randomised, multicentre, double-blind, placebo-controlled clinical study in which 1326 patients were enrolled and randomly assigned to receive either placebo (n = 437), or a cumulative dose of MAVENCLAD of either 3.5 mg/kg (n = 433) or 5.25 mg/kg (n = 456) in 2 treatment courses over the 96 week (2-year) trial period.
MAVENCLAD was administered orally as 10 mg tablets, with the number of tablets taken daily based on the patient's body weight using 10 kg weight ranges. Patients randomised to the 3.5 mg/kg cumulative dose received a first treatment course at weeks 1 and 5 of the first year and a second treatment course at weeks 1 and 5 of the second year. Patients randomised to the 5.25 mg/kg cumulative dose received additional treatment at weeks 9 and 13 of the first year.
The majority of patients in the placebo (86.3%) and the MAVENCLAD 3.5 mg/kg (91.2%) and 5.25 mg/kg (86.2%) treatment groups completed both treatment courses through 52 weeks. A correspondingly high proportion of patients in the placebo and the MAVENCLAD 3.5 mg/kg and 5.25 mg/kg treatment groups (87.0%, 91.9%, and 89.0%, respectively) completed the full 96 weeks of the trial.
In the overall trial population, the median age was 39 years (range 18 to 65), and the female to male ratio was approximately 2:1. The median duration of MS prior to trial enrolment was 6.7 years, and the median baseline neurological disability based on Expanded Disability Status Scale (EDSS) score across all treatment groups was 3.0 (range 0 to 6.0). The mean number of T1 gadolinium-enhancing (Gd+) lesions, T1 hypointense lesions, and mean T2 lesion volumes were 0.93, 7.7, and 15,467 mm3, respectively. Over two thirds of the trial patients were treatment-naive for MS disease-modifying medications.
Both MAVENCLAD treatment groups, 5.25 mg/kg and 3.5 mg/kg, were significantly superior to placebo in the treatment of relapsing-remitting MS. Clinical outcomes are shown in Table 1. (See Table 1.)
 Click on icon to see table/diagram/image
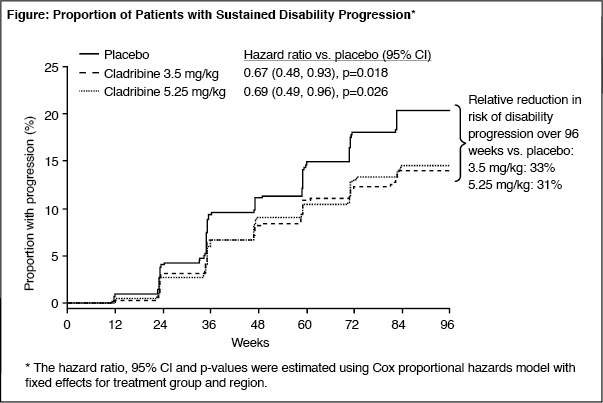
Click on icon to see table/diagram/imageTime to sustained disability progression was defined as the time to worsening in EDSS score of ≥ 1 unit if baseline EDSS was 0.5 to 4.5, or ≥ 1.5 units if baseline EDSS was 0, or ≥ 0.5 unit if EDSS was ≥ 5, and persistent for at least 12 weeks. Treatment with MAVENCLAD 3.5 mg/kg and 5.25 mg/kg resulted in a prolongation in time to sustained disability progression of 12 weeks (10th percentile, both treatment groups) compared with placebo (Figure 1).
The 3.5 mg/kg and 5.25 mg/kg treatment groups had a 33% and a 31% relative reduction in risk of developing disability progression over the 96-week trial period, respectively, compared with the placebo group (hazard ratio = 0.67, 95% CI [0.48, 0.93], p = 0.018; hazard ratio 0.69, 95% CI [0.49, 0.96], p = 0.026, respectively). The proportion of patients progressing to sustained disability was 20.6% in the placebo group, 14.3% in the 3.5 mg/kg treatment group and 15.1% in the 5.25 mg/kg treatment group. (See figure.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageIn addition, both MAVENCLAD treatment groups were statistically significantly superior to placebo with regard to number and relative reduction of T1 Gd+ enhancing lesions, active T2 lesions and combined unique lesions as demonstrated on brain magnetic resonance imaging (MRI) over the entire 96 weeks of the trial. Patients in the MAVENCLAD 3.5 mg/kg and the 5.25 mg/kg treatment groups compared to the placebo treatment group had 86% and 88% relative reductions in the mean number of T1 GD+ lesions, 73% and 77% relative reductions in the mean number of active T2 lesions, and 74% and 78% relative reductions, in the mean number of combined unique lesions per patient per scan (p < 0.001 for both groups across all 3 MRI outcomes).
As shown previously in Table 1, a higher cumulative dose did not add any clinically meaningful benefit, but was associated with a higher incidence in ≥ grade 3 lymphopenia (44.9% in the 5.25 mg/kg group vs. 25.6% in the 3.5 mg/kg group).
Post hoc analysis showed a greater relative reduction in risk of relapse over 2 years for patients with highly active disease prior to receiving cladribine than in the overall patient population (68% reduction compared with 58% overall). The relative risk of 3-month disability progression over 2 years was reduced to a greater extent in patients with more active disease at baseline (72% reduction compared with 33% overall).
Subgroup analyses of region, gender, age and relapse history all showed positive treatment effects from both doses of MAVENCLAD with no large differences between subgroups.
Patients who had completed the CLARITY study could be enrolled in CLARITY Extension (EXT) study. In this extension study, 806 patients received either placebo or a cumulative dose of cladribine 3.5 mg/kg (in a regimen similar to that used in CLARITY) over the 96-week study period.
Of these, 98 patients treated for 2 years in CLARITY with MAVENCLAD 3.5 mg/kg were switched to placebo for 2 years in CLARITY EXT. The magnitude of the effect in reducing the frequency of relapses and slowing disability progression in patients receiving the 3.5 mg/kg dose in years 1 and 2 was maintained during CLARITY EXT (in years 3 and 4). The annualised relapse rate was 0.15 and 72.4% of these patients did not experience 3-month confirmed disability progression during CLARITY EXT. Also, the group continued to exhibit low T1-Gd+ lesion activity.
In CLARITY EXT study, no additional efficacy was demonstrated when patients were given additional treatment courses of MAVENCLAD (n=186) in years 3 and 4.
Pharmacokinetics: Cladribine is a prodrug that has to be phosphorylated intracellularly to be efficacious. The pharmacokinetics of cladribine were studied following oral and intravenous administration in MS patients, in patients with malignancies and in in vitro systems.
Absorption: Following oral administration of MAVENCLAD tablets, cladribine is absorbed rapidly. Administration of 10 mg tablets resulted in a mean Cmax in the range of 22 to 29 ng/mL and corresponding mean AUC in the range of 80 to 101 ng·h/mL (arithmetic means from various studies). When oral cladribine was given in fasted state, median Tmax was 0.5 h (range 0.5 to 1.5 h). When administered with a high-fat meal, absorption of cladribine was delayed (median Tmax 1.5 h, range 1 to 3 h) and Cmax was reduced by 29% (based on geometric mean), while AUC was unchanged.
The oral bioavailability of cladribine 10 mg was approximately 40%.
Distribution: The volume of distribution is large, indicating extensive tissue distribution and intracellular uptake. The mean volume of distribution of cladribine was estimated as 487 L (SD ± 180). The plasma protein binding is 20%, and independent of plasma concentration. Intracellular concentrations of phosphorylated cladribine were found to be several hundred-folds higher than corresponding plasma concentrations.
Cladribine is able to penetrate the blood brain barrier as shown by a cerebrospinal fluid/plasma concentration ratio of approximately 0.25.
Metabolism: The metabolism of cladribine was studied in MS patients following the administration of a single 10-mg oral tablet and a single 3-mg intravenous dose. Following both oral and intravenous administration, the parent compound cladribine was the main component present in plasma and urine, e.g. accounting only for ≤ 3% of plasma parent drug exposure after oral administration. The primary metabolite 2-chloroadenine proved to be a minor metabolite both in plasma and in urine. Only traces of other metabolites could be found in plasma and urine.
In hepatic in vitro systems, minor metabolism of cladribine was observed (92% to 99% was unchanged cladribine). In vitro studies also showed negligible transporter-mediated uptake of cladribine into human hepatocytes.
After entering the cell, cladribine is phosphorylated to cladribine monophosphate (Cd-AMP) by deoxycytidine kinase (and also by deoxyguanosine kinase in the mitochondria). Cd-AMP is further phosphorylated to cladribine diphosphate (Cd-ADP) and cladribine triphosphate (Cd-ATP). The dephosphorylation and deactivation of Cd-AMP is catalysed by cytoplasmic 5'-nucleotidase.
In a study of the intracellular pharmacokinetics of Cd-AMP and Cd-ATP in patients with chronic myelogenous leukaemia, the levels of Cd-ATP were approximately half of the Cd-AMP levels. Intracellular t1/2 of Cd-AMP was 15 h. Intracellular t1/2 of Cd-ATP was 10 h.
Elimination: The renal and the non-renal routes of cladribine elimination are approximately equally important. Based on pooled population pharmacokinetic data from various studies, the median values for the two elimination routes were 22.2 L/h for renal clearance and 23.4 L/h for non-renal clearance. Renal clearance exceeded the glomerular filtration rate, indicating active renal secretion of cladribine.
The non-renal part of the elimination of MAVENCLAD (approximately 50%) consists of fractional hepatic metabolism and presumably of extensive intracellular distribution and trapping of the active cladribine principle (Cd-ATP) within the targeted intracellular compartment (i.e. the lymphocytes) and subsequent elimination of intracellular Cd-ATP according to the life-cycle and elimination pathways of these cells.
The pharmacokinetics of cladribine are best described by a three-compartment model where the estimated terminal half-life for a typical patient from the population pharmacokinetic analysis is approximately 1 day. This however does not result in any drug accumulation after once daily dosing as this half-life only accounts for a small portion of the AUC.
Dose and Time Dependence: After oral administration of cladribine tablets across a dose range from 3 mg to 20 mg, Cmax and AUC increase in a linear dose-proportional fashion, suggesting that absorption is not affected by rate- or capacity-limited processes up to a 20 mg oral dose.
No accumulation of cladribine plasma concentrations have been observed after repeated dosing.
There is no indication that cladribine pharmacokinetic parameters might change in a time-dependent fashion after repeated administration.
Special populations: No studies have been conducted to evaluate the pharmacokinetics of MAVENCLAD in elderly or paediatric MS patients, or in subjects with renal or hepatic impairment.
A population pharmacokinetic analysis did not show any effect of age (range 18 to 65 years) or gender on cladribine pharmacokinetics.
The results of the clinical trials did not show any evidence of cardiotoxicity, however patients with significant cardiac pathology, such as angina, congestive heart failure or arrhythmias, were not eligible to be enrolled in the clinical trials.
Renal impairment: Renal and non-renal routes are equally important for the elimination of MAVENCLAD. Total clearance was shown to be dependent on creatinine clearance. Based on a population pharmacokinetic analysis including patients with normal renal function and with mild renal impairment, total clearance in patients with mild renal impairment (CLCR = 60 mL/min) is expected to decrease moderately, leading to an increase in exposure of 25%.
Hepatic impairment: The importance of hepatic function for the elimination of cladribine is considered low.
Toxicology: Preclinical safety data: Carcinogenicity: While no treatment-related tumours were seen in a 26-week carcinogenicity study in transgenic mice by oral administration, an increased incidence of Harderian gland adenomas was seen in a 22-month carcinogenicity study in mice by subcutaneous administration. The clinical relevance of this is unclear as humans do not have this anatomical structure. However, based on its mode of action and positive findings in mammalian genotoxicity tests (in vitro and in vivo), a carcinogenic potential of cladribine cannot be excluded.
Genotoxicity: Cladribine was shown to be genotoxic, causing chromosomal damage in the bone marrow of mice in vivo and in CHO-WBL cells in vitro. These findings are expected since cladribine is known to cause inhibition of DNA synthesis by an imbalance of deoxynucleotide triphosphate pools, DNA strand breaks, inhibition of DNA repair, and depletion of intracellular nicotinamide adenine dinucleotide (NAD). Cladribine was not mutagenic in vitro (bacterial and mammalian cell mutation assays) and did not induce unscheduled DNA synthesis in primary rat hepatocyte cultures.