ATC code: Not applicable.
Pharmacology: Pharmacodynamics: Mechanism of action: Elobixibat inhibits bile acid reabsorption via ileal bile acid transporter (IBAT) expressed on the epithelial cells of the terminal ileum and thereby increases the amount of bile acid passing into the large intestinal lumen. Bile acid promotes the secretion of water and electrolytes into the large intestinal lumen and enhances the colonic motility. Therefore, GOOFICE induces the therapeutic effect on constipation.
Effect on constipation induced by loperamide in rats: In rats of loperamide-induced constipation model, a single oral administration of elobixibat demonstrated the effect of improving constipation.
Clinical efficacy (Japanese): Phase III Study and Long-term Treatment Study were conducted in Japanese patients with chronic constipation (except for constipation associated with organic diseases, drug-induced and disease-induced constipations). The diagnosis of chronic constipation was defined as less than three spontaneous bowel movements (SBMs) per week and had at least one of the following 3 symptoms related to SBM: (1) straining during at least 25% of defecations; (2) lumpy or hard stools in at least 25% of defecations; and (3) sensation of incomplete evacuation for at least 25% of defecations.
Phase III Double-blind, Placebo-controlled Comparative Study (Japanese): A total of 132 patients (female: 82.5% (52/63) in placebo, 82.6% (57/69) in GOOFICE; age: 43.8±13.0 years in placebo, 43.0±13.7 years in GOOFICE; BMI: 21.81±2.65 kg/m
2 in placebo, 21.42±2.55 kg/m
2 in GOOFICE) were orally administered placebo or GOOFICE 10 mg once daily before breakfast for 2 weeks.
The primary endpoint, the change in SBM frequency at treatment Week 1 from baseline in GOOFICE was significantly greater than that in placebo (placebo: 1.73±1.88, GOOFICE: 6.40±4.73, p<0.0001). The change in SBM frequency at treatment Week 2 from baseline in GOOFICE was significantly greater than that in placebo (placebo: 1.79±1.78, GOOFICE: 5.00±3.20, p<0.0001). The median time to the first SBM was 25.5 hours in placebo and 5.2 hours in GOOFICE (p=0.0001). The changes in complete spontaneous bowel movements (CSBM) frequency at treatment Week 1 and at treatment Week 2 from baseline were also significantly greater in the GOOFICE than those in the placebo (placebo: 0.62±1.44 and 0.86±1.45, GOOFICE: 3.39±3.86 and 2.98±3.10, both p<0.0001). (See Figure 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Long-term Treatment Study (Japanese): A total of 340 patients (female: 83.2% (283/340), age: 43.9±12.0 years, and BMI: 21.84±3.15 kg/m
2) were orally administered GOOFICE once daily before breakfast for 52 weeks. The initial dose was 10 mg, and after 7 days from starting administration, the daily dose could be adjusted to 5 mg, 10 mg or 15 mg depending on symptoms.
The change in SBM frequency from baseline was 4.55±3.63, 4.01±3.10, and 3.70±2.92 at treatment Week 1, 2, and 3, respectively. Subsequently, it was stable between 3.12 and 3.88 until Week 52. A significant increase as compared to baseline was observed for all time points that were treatment Week 4, 12, 24, 36, and 52 (1 sample t test, p<0.0001 for all the time points). The estimate of median time to the first SBM by the Kaplan-Meier method was 7.00 hours (95% confidence interval, 5.67 to 7.75 hours). The change in CSBM frequency from baseline was 2.54±3.18 at treatment Week 1 and 2.39±2.93 at treatment Week 2. After treatment Week 2, it was stable between 2.11 and 2.48 until Week 52. A significant increase as compared to baseline was observed for all time points that were treatment Week 4, 12, 24, 36, and 52 (1 sample t test, p<0.0001 for all the time points). (See Figure 2.)
Click on icon to see table/diagram/image
Clinical efficacy (US): Phase IIb study in patients with chronic idiopathic constipation (CIC) was conducted in US. The diagnosis of CIC was defined as less than 3 CSBMs per week and had at least 2 of the following 4 symptoms for the previous 3 months with symptom onset at least 6 months prior to diagnosis: (1) straining during at least 25% of defecations; (2) lumpy or hard stools in at least 25% of defecations; (3) sensation of incomplete evacuation in at least 25% of defecations; (4) sensation of anorectal obstruction/blockage in at least 25% of defecations.
Phase IIb Double-blind, Placebo-controlled Comparative Study (US): A total of 190 patients (female: 89.5% (170/190), age 48.1 years (range, 20 to 79 years)) were orally administered placebo or 3 doses of GOOFICE (5, 10 and 15 mg) once daily before breakfast for 8 weeks. The primary endpoint, change from baseline in SBM frequency at treatment Week 1 was significantly increased in 10 mg and 15 mg as compared to placebo (10mg vs placebo: mean difference=2.31; 0.89-3.73; p=0.002, 15mg vs Placebo: mean difference=3.73; 2.33-5.13; p<0.001) in the modified intent-to-treat (mITT) population, excluding patients using rescue medications during Week 1. The change in SBM frequency per week from Week 1 to Week 8 from baseline was significantly greater in 10 mg and 15 mg compared to placebo. (See Table 2.)
Click on icon to see table/diagram/image
The change from baseline in CSBM frequency at week 1 was significantly increased in 5, 10 and 15 mg as compared to placebo. The change in CSBM frequency per week from Week 1 to Week 8 from baseline was significantly greater in all treatment groups compared to placebo. (See Table 3.)
Click on icon to see table/diagram/image
Pharmacokinetics: Absorption: A single oral dose of GOOFICE 5 mg, 10 mg or 15 mg was administered to patients with chronic constipation before breakfast and the pharmacokinetic parameters were noted as follows. Analysis using a power model showed that the slope of the regression equation for C
max and AUC
0-∞ indicated an increase in exposure with the dose increase. (See Table 4.)
Click on icon to see table/diagram/image
The repeated oral dose of GOOFICE 5 mg, 10 mg or 15 mg was administered to patients with chronic constipation before breakfast and the pharmacokinetic parameters on Day 14 were noted as follows. No accumulation potential was observed at dose levels >5 mg on Day 14 of repeated-dose administration. (See Table 5.)
Click on icon to see table/diagram/image
A single oral dose of
14C-elobixibat 5 mg (approx. 2.75 MBq) was administered to healthy adult male subjects (n=6) before breakfast and the pharmacokinetic parameters were noted as follows. (See Table 6.)
Click on icon to see table/diagram/image
Distribution: In vitro human plasma protein binding rate of elobixibat was in excess of 99% with human blood to plasma concentration ratio less than 5%.
Metabolism: No metabolites were observed in plasma of healthy adult male subjects (n=6) following a single oral dose of
14C-elobixibat 5 mg (approx. 2.75 MBq). Unchanged and monohydroxy forms of elobixibat were found in feces pooled over 24 to 48 hours post-dose, while the percentages of radioactivity were 96.06% and 3.16%, respectively, indicating that the majority was unchanged form.
Excretion: When a single oral dose of GOOFICE was administered to patients with chronic constipation under fasting conditions, the cumulative urine drug excretion rate up to 144 hours post-dose was approximately 0.01% of the amount of dose, indicating that drug excretion into urine was almost absent.
When a single oral dose of
14C-elobixibat 5 mg (approx. 2.75 MBq) was administered to healthy adult male subjects (n=6), 103.1% of radioactivity dosed was excreted in feces while 0.00 to 0.02% excreted in urine up to 144 hours post-dose.
Drug-drug interactions: IC
50 of elobixibat towards digoxin (P-glycoprotein substrate) transport was 2.65 μmol/L in Caco-2 cells, indicating the inhibitory effect of elobixibat on P-glycoprotein.
In healthy adult male and female subjects (n=25), GOOFICE 10 mg was orally administered once daily for 5 days with coadministration of both dabigatran etexilate 150 mg/dose/day on Day 1 and midazolam 2 mg/dose/day on Day 1 and Day 5 to compare with monoadministration of each drug. The results showed that AUC
0-t and C
max of dabigatran (P-glycoprotein substrate) were 1.17 fold greater (90% confidence interval: 1.00-1.36) and 1.13 fold greater (90% confidence interval: 0.96-1.33), respectively, compared with those under monoadministration and both the upper limit of 90% confidence intervals were above 1.25 as the reference value. AUC
0-t and C
max of midazolam on Day 5 were 0.78-fold greater (90% confidence interval: 0.73-0.83) and 0.94-fold greater (90% confidence interval: 0.87-1.01), respectively, compared with those under monoadministration and the lower limit of 90% confidence intervals of AUC
0-t was below 0.80 as the reference value.
Food effects: In patients with chronic constipation (n=60), the effect of food intake on pharmacokinetics was evaluated following a single oral dose of GOOFICE in a crossover design. C
max and AUC
0-∞ under fed condition were approximately 20 to 30% of those under fasting one.
Effect of gender difference: The repeated oral dose of GOOFICE 5 mg, 10 mg or 15 mg was administered to Japanese patients with chronic constipation before breakfast. When AUC
0-τ was subjected to analysis of covariance using covariates including gender, no gender difference was observed on Day 8 and Day 14 of repeated-dose administration.
Effect of race difference: Steady-state exposures following repeated doses of GOOFICE 15 mg or 20 mg once daily before breakfast were compared in Japanese patients with chronic constipation and US patients with functional constipation. C
max for US patients tended to be higher than that for Japanese patients, while AUC was almost the same for both (internal data).
Toxicology: Pre-clinical safety data: Though the liver-related findings (increase in blood AST and ALT and hepatocyte vacuolar degeneration) were observed in mice (500 mg/kg/day and higher at treatment Week 13) and the frequent vomiting was observed in dogs (139.2 mg/kg/day and higher at treatment Week 4 and 13) in repeated oral dose toxicity studies, wide safety margins were supported by NOAEL, and there seemed to be no concern about safety in clinical practice.
Neither genotoxicity nor carcinogenicity of elobixibat was recognized.



 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image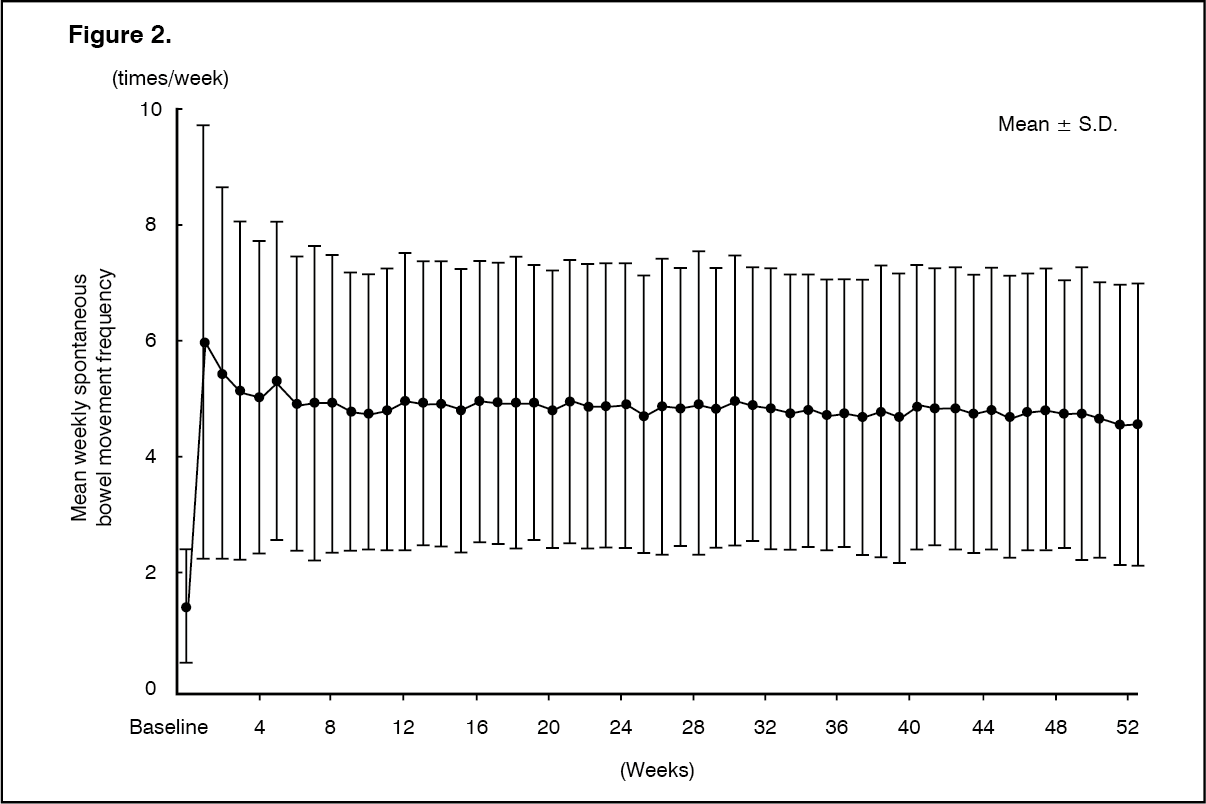 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image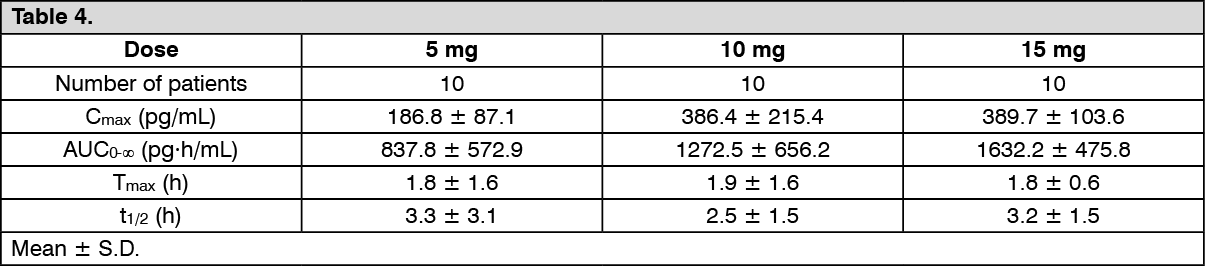 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image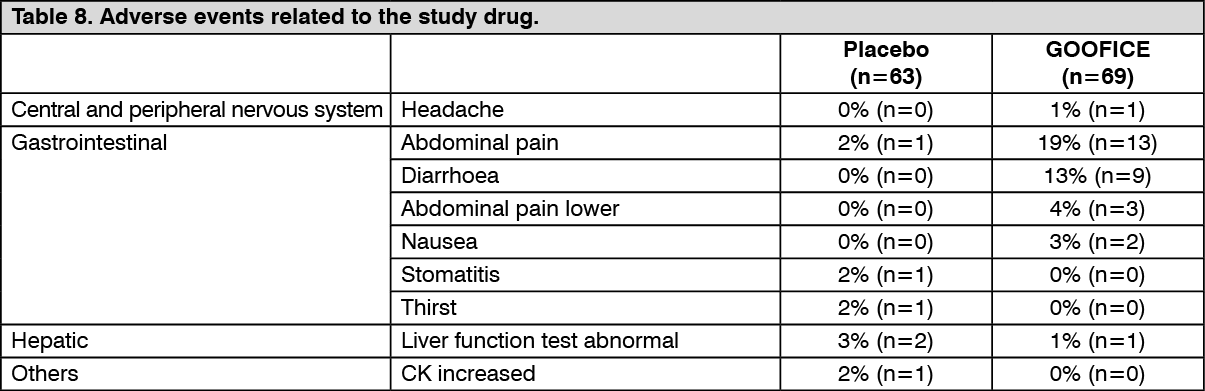 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image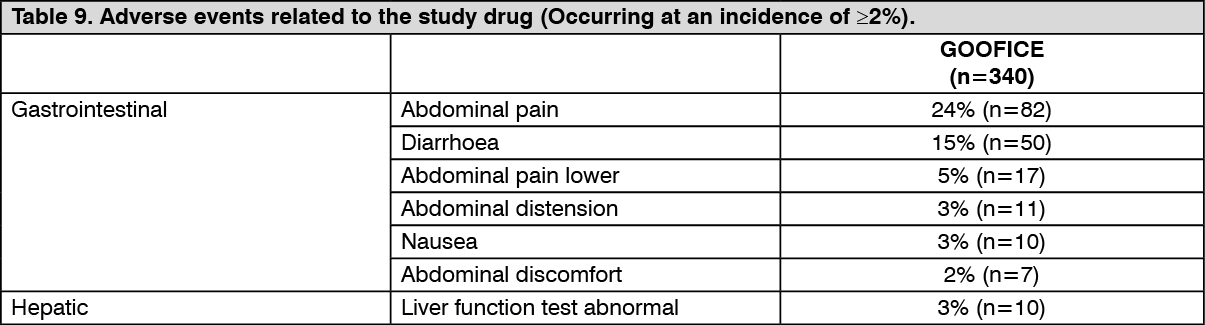 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image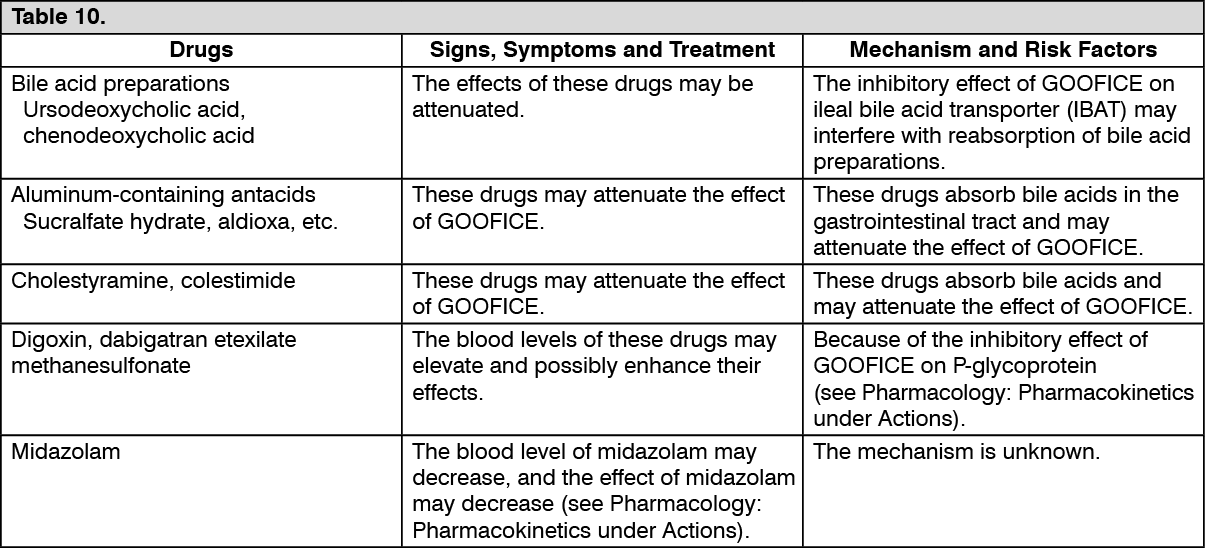 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out
