One ampoule of 8.5 ml solution contains 1 mg terlipressin acetate, corresponding to 0.85 mg terlipressin free base. The concentration of the solution is 0.1 mg terlipressin free base/ml.
Excipients/Inactive Ingredients: Sodium chloride, acetic acid, sodium acetate trihydrate and water for injections.
Pharmacotherapeutic group: Posterior pituitary lobe hormones (vasopressin and analogues). ATC code: H01BA04.
Pharmacology: Pharmacodynamics: Terlipressin initially has an effect of its own, but is converted by enzymatic cleavage to lysine vasopressin. Doses of 1 and 2 mg terlipressin acetate effectively reduce the portal venous pressure and produce marked vasoconstriction. The lowering of portal pressure and azygos blood flow is dependent on dose. The effect of the low dose is reduced after 3 hours, while haemodynamic data show that 2 mg terlipressin acetate is more effective than 1 mg as the higher dose produces a dependable effect throughout the period of treatment (4 hours).
Pharmacokinetics: The pharmacokinetics follows a two-compartment model. It has been found that the half-life is approximately 40 min., metabolic clearance is approximately 9 ml/kg/min and the distribution volume is approximately 0.5 l/kg.
The desired concentration of lysine vasopressin in plasma is found initially after approximately 30 min. and reaches a peak value of 60 to 120 min. after administration of GLYPRESSIN. Because of 100% cross-reaction between terlipressin and lysine vasopressin, there is no specific RIA method for these substances.
Toxicology: Preclinical safety data: Preclinical data reveal no special hazard for humans based on conventional studies of single- and repeat-dose toxicity, and genotoxicity. At dosages relevant to humans, the only effects observed in animals were those attributable to the pharmacological activity of terlipressin.
No pharmacokinetic data are available from animals to compare with humans the plasma concentrations at which these effects occurred, but as the route of administration was intravenous, a substantial systemic exposure can be assumed for the animal studies.
An embryo-fetal study in rats demonstrated no adverse effects of terlipressin, but in rabbits abortions occurred, probably related to maternal toxicity, and there were ossification anomalies in a small number of fetuses and a single isolated case of cleft palate.
No carcinogenicity studies have been performed with terlipressin.
Bleeding oesophageal varices.
Treatment of patients with hepatorenal syndrome (HRS) Type 1 who are actively being considered for liver transplant.
Bleeding Oesophageal Varices (BOV): Posology: Adults: Initially an i.v. injection of 2 ampoules of GLYPRESSIN solution for injection (2 mg terlipressin acetate, equivalent to 1.7 mg terlipressin) is given every 4 hours. The treatment should be maintained until bleeding has been controlled for 24 hours, but up to a maximum of 48 hours. After the initial dose, the dose can be adjusted to 1 ampoule of GLYPRESSIN solution for injection (1 mg terlipressin acetate, equivalent to 0.85 mg terlipressin) i.v. every 4 hours in patients with body weight < 50 kg or if adverse effects occur.
Method of Administration: i.v. injection.
Hepatorenal Syndrome (HRS): Posology: 1 ampoule of GLYPRESSIN solution for injection (1 mg terlipressin acetate, equivalent to 0.85 mg terlipressin) every 6 to 12 hours by slow intravenous bolus injection for 7 to 14 days (administered in association with albumin 20% 100 mL IV twice daily for 7 to 14 days).
If serum creatinine (SCr) has not decreased by at least 30% from the baseline value after 3 days, the dose can be increased to a maximum of 2 ampoules of GLYPRESSIN solution for injection (2 mg terlipressin acetate, equivalent to 1.7 mg terlipressin) every 6 hours.
It is however recommended that the dose not be increased in patients with severe pre-existing cardiovascular disease or in the presence of an ongoing significant adverse event e.g. pulmonary oedema, ischaemia. Treatment should be continued until about 2 days after the patient achieves HRS reversal (SCr less than or equal to 132.6 μmol/L), or be discontinued if the patient undergoes dialysis or liver transplant or if SCr remains at or above baseline after 7 days of treatment.
Management of suspected adverse drug reactions may require temporary interruption and/or dose reduction. When the patient's symptoms resolve, GLYPRESSIN may be re-commenced at a lower dose or at a less frequent dosing interval (e.g., every 8 - 12 hours). The lowest doses used in the clinical studies ranged from 1.7 to 2.55 mg terlipressin/day. The maximum dose studied (TAHRS Study*) was 1.7 mg terlipressin every 4 hours.
*The study of Martín–Llahí et al. (2008), also known as the TAHRS study, was a supportive open-label, comparative multicentre study in 46 patients who were randomised in a 1:1 ratio to receive either intravenous terlipressin (0.85 - 1.7 mg (as 1 to 2 mg terlipressin acetate) every 4 hours) plus 20% albumin or 20% albumin alone, for a maximum of 15 days. The majority of patients had HRS type 1 (35/46) and the remainder, HRS type 2 (11/46).
Method of Administration: i.v. injection.
The recommended dose (2 mg terlipressin acetate or 1.7 mg terlipressin/4 hours) should not be exceeded as the risk of severe circulatory adverse effects is dose-dependent.
Elevated blood pressure in patients with recognised hypertension can be controlled with 150 mcg clonidine i.v.
Bradycardia requiring treatment should be treated with atropine.
Contraindicated in pregnancy.
Hypersensitivity to terlipressin or any other excipients of the product.
Blood pressure, heart rate and fluid balance should be monitored during treatment. To avoid local necrosis at the injection site, the injection must be given i.v.
Caution should be exercised in treating patients with hypertension or recognised heart disease. In patients with septic shock with a low cardiac output terlipressin should not be used.
This medicinal product contains 1.33 mmol (or 30.7 mg) of sodium per ampoule. To be taken into consideration in patients on a controlled sodium diet.
Cardiovascular Effects: Terlipressin should only be used with caution and under strict monitoring of the patients in the following cases: uncontrolled hypertension; cerebral or peripheral vascular diseases; cardiac arrhythmias; coronary artery disease or previous myocardial infarction.
Terlipressin should not be used in patients with unstable angina or recent acute myocardial infarction.
Torsade de pointes: During clinical trials and post-marketing experience, several cases of QT interval prolongation and ventricular arrhythmias including "Torsade de pointes" have been reported (see Adverse Reactions). In most cases, patients had predisposing factors such as basal prolongation of the QT interval, electrolyte abnormalities (hypokalaemia, hypomagnesaemia) or medications with concomitant effect on QT prolongation. Therefore, extreme caution should be exercised in the use of terlipressin in patients with a history of QT interval prolongation, electrolytic abnormalities, concomitant medications that can prolong the QT interval (see Interactions).
Ischaemic Events: To avoid local necrosis the injection must be administered intravenously.
During post-marketing experience several cases of peripheral ischemia and necrosis unrelated to the injection site have been reported. Patients with peripheral venous hypertension or morbid obesity seem to have a greater tendency to this reaction. Therefore, extreme caution should be exercised when administering terlipressin in these patients.
Respiratory Effects: Terlipressin may cause smooth muscle constriction and should be used with caution and under strict monitoring in patients with severe asthma or chronic obstructive pulmonary disease (COPD).
Laboratory Monitoring: During treatment with terlipressin, serum creatinine should be monitored at least daily as terlipressin should be used with caution in patients with renal insufficiency. Fluid balance and electrolytes should be monitored carefully as hyponatraemia, hypokalaemia, hypomagnesaemia and other electrolyte disturbances have been reported.
Effects on ability to drive and use machines: No studies on the effects on the ability to drive and use machines have been performed.
Use in Children: Particular caution should be exercised in the treatment of children and elderly patients, as experience is limited in these groups.
There are no data available regarding dosage recommendation in these special patient categories.
Use in the Elderly: Particular caution should be exercised in the treatment of children and elderly patients, as experience is limited in these groups.
There are no data available regarding dosage recommendation in these special patient categories.
Pregnancy: Treatment with terlipressin during pregnancy is contraindicated (see Contraindications and Pharmacology: Toxicology: Preclinical safety data under Actions).
Terlipressin has been shown to cause uterine contractions and increased intrauterine pressure in early pregnancy and may decrease uterine blood flow. Terlipressin may have harmful effects on pregnancy and foetus.
Spontaneous abortion and malformation has been shown in rabbits after treatment with Terlipressin.
Breastfeeding: It is not known whether terlipressin is excreted in human breast milk. The excretion of terlipressin in milk has not been studied in animals. A risk to the suckling child cannot be excluded. A decision on whether to continue/discontinue breast-feeding or to continue/discontinue therapy with terlipressin should be made taking into account the benefit of breast-feeding to the child and the benefit of terlipressin therapy to the woman.
The reporting of safety data rely on published literature and post marketing surveillance.
Clinical Trials: Three studies assessed safety as primary outcome in totally 1341 patients.
Caletti 1991, a prospective, uncontrolled observational study, enrolled 1258 patients. 21% of the patients experienced a side-effect. The side-effects reported were consistent with the known pharmacological actions of terlipressin.
Bruha 2009, a randomised, double-blind study enrolled 25 patients that were randomised to either 5-day or 10-day treatment. Serum sodium and serum creatinine decreased in both arms during treatment, but rose again after discontinuation of treatment.
Solà 2010, a retrospective cohort study, included 58 patients. Over a 5 day treatment period 67% of the patients developed acute reduction in serum sodium. The hyponatraemia was found to develop rapidly after start of therapy, but was usually reversible with a median recovery time of 4 days after discontinuation of terlipressin.
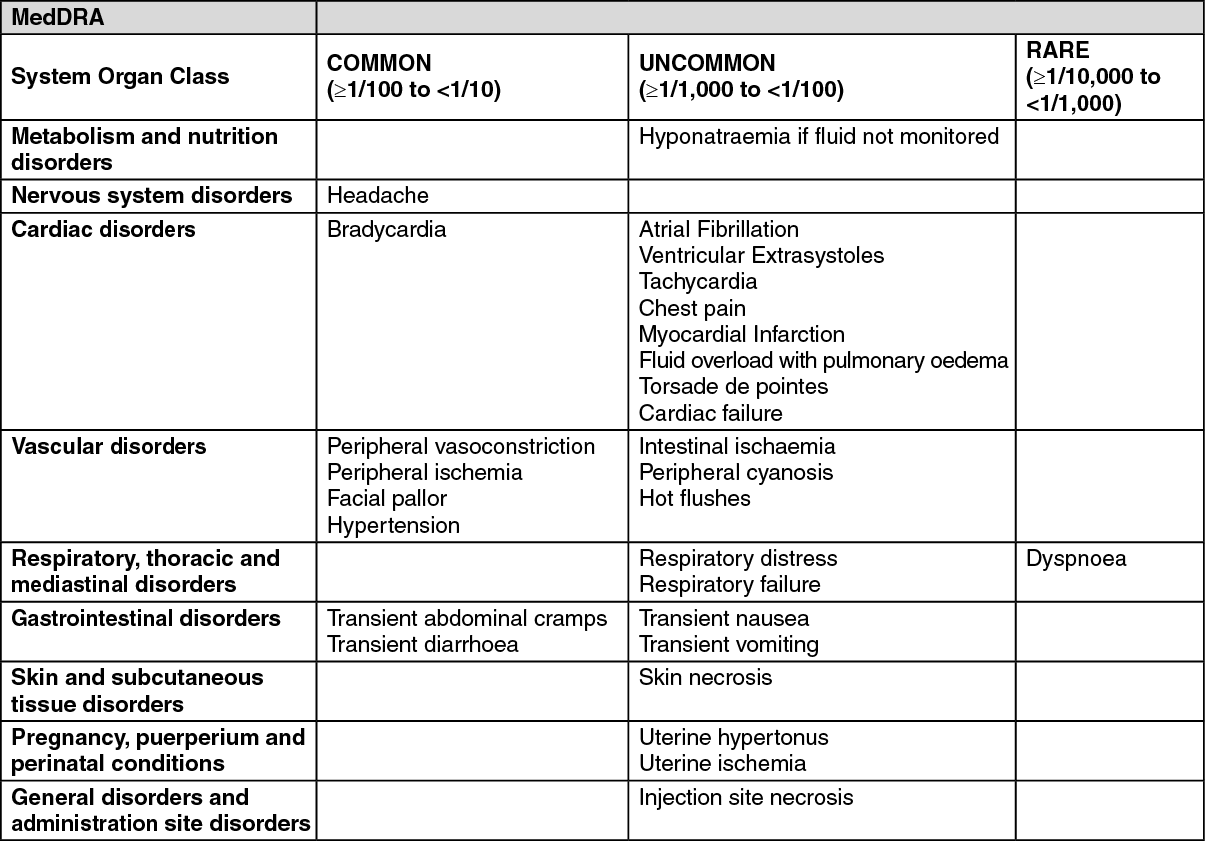
The most commonly reported undesirable effects in clinical trials (frequency 1-10%) are paleness, increased blood pressure, abdominal pain, nausea, diarrhoea and headache.
The antidiuretic effect of GLYPRESSIN may cause hyponatraemia unless the fluid balance is controlled. (See table.)
 Click on icon to see table/diagram/image
Post-Marketing Experience:
Click on icon to see table/diagram/image
Post-Marketing Experience: The following additional adverse reactions have been reported in post-marketing use: Venticular fibrillation (frequency not known).
The hypotensive effect of non-selective beta-blockers on the portal vein is increased with terlipressin.
Concomitant treatment with medicinal products with a known bradycardic effect (e.g. propofol, sufentanil) may lower the heart rate and cardiac output. These effects are due to reflexogenic inhibition of cardiac activity via the vagus nerve due to the elevated blood pressure.
Terlipressin can trigger "torsade de pointes" (see Precautions and Adverse Reactions). Therefore, extreme caution should be exercised in the use of terlipressin in patients with concomitant medications that can prolong the QT interval, such as class IA and III antiarrhythmics, erythromycin, certain antihistamines and tricyclic antidepressants or medications that may cause hypokalaemia or hypomagnesemia (e.g. some diuretics).
Special precautions for disposal and other handling: Any unused drug or waste materials should be disposed of in accordance with local requirements.
Incompatibilities: In the absence of compatibility studies, this medicinal product must not be mixed with other medicinal products.
Store in a refrigerator (2°C - 8°C). The ampoules are stored in the outer carton in order to protect from light.
Shelf life: 2 years.
H01BA04 - terlipressin ; Belongs to the class of vasopressin and analogues. Used in posterior pituitary lobe hormone preparations.
Glypressin soln for inj 1 mg/8.5 mL
5 × 1's



 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out
