Therapeutic Class: Ezetimibe + Rosuvastatin (ROSUZET) is a lipid-lowering product that selectively inhibits the intestinal absorption of cholesterol and related plant sterols and inhibits the endogenous synthesis of cholesterol.
Pharmacology: Pharmacodynamics: Mechanism of Action: Ezetimibe + Rosuvastatin (ROSUZET): Plasma cholesterol is derived from intestinal absorption and endogenous synthesis. Ezetimibe + Rosuvastatin (ROSUZET) contains ezetimibe and rosuvastatin, two lipid-lowering compounds with complementary mechanisms of action. Ezetimibe + Rosuvastatin (ROSUZET) reduces elevated total-C, LDL-C, Apo B, TG, and non-HDL-C, and increases HDL-C through dual inhibition of cholesterol absorption and synthesis.
Ezetimibe: Ezetimibe inhibits the intestinal absorption of cholesterol. Ezetimibe is orally active and has a mechanism of action that differs from other classes of cholesterol-reducing compounds (e.g., statins, bile acid sequestrants [resins], fibric acid derivatives, and plant stanols). The molecular target of ezetimibe is the sterol transporter, Niemann-Pick C1-Like 1 (NPC1L1), which is responsible for the intestinal uptake of cholesterol and phytosterols.
Ezetimibe localizes at the brush border of the small intestine and inhibits the absorption of cholesterol, leading to a decrease in the delivery of intestinal cholesterol to the liver; statins reduce cholesterol synthesis in the liver and together these distinct mechanisms provide complementary cholesterol reduction.
In a 2-week clinical study in 18 hypercholesterolemic patients, ezetimibe inhibited intestinal cholesterol absorption by 54%, compared with placebo.
A series of preclinical studies was performed to determine the selectivity of ezetimibe for inhibiting cholesterol absorption. Ezetimibe inhibited the absorption of [
14C]-cholesterol with no effect on the absorption of triglycerides, fatty acids, bile acids, progesterone, ethinyl estradiol, or the fat-soluble vitamins A and D.
Rosuvastatin: Rosuvastatin is a selective, potent and competitive inhibitor of HMG-CoA reductase, the rate-limiting enzyme that converts 3-hydroxy-3-methylglutaryl coenzyme A to mevalonate, a precursor of cholesterol. Triglycerides (TG) and cholesterol in the liver are incorporated, with apolipoprotein B (ApoB), into very low density lipoprotein (VLDL) and released into the plasma for delivery to peripheral tissues. VLDL particles are TG-rich. Cholesterol-rich low density lipoprotein (LDL) is formed from VLDL and is cleared primarily through the high affinity LDL receptor in the liver.
Rosuvastatin produces its lipid-modifying effects in two ways; it increases the number of hepatic LDL receptors on the cell-surface, enhancing uptake and catabolism of LDL and it inhibits the hepatic synthesis of VLDL, thereby reducing the total number of VLDL and LDL particles. High density lipoprotein (HDL), which contains ApoA-I is involved, amongst other things, in transport of cholesterol from tissues back to the liver (reverse cholesterol transport).
The involvement of LDC-C in atherogenesis has been well documented. Epidemiological studies have established that high LDL-C, TG, low HDL-C and ApoA-I have been linked to a higher risk of cardiovascular disease. Intervention studies have shown the benefits in mortality and CV event rates of lowering LDL-C and TG or raising HDL-C. More recent data has linked the beneficial effects of HMG CoA reductase inhibitors to lowering of non-HDL (i.e. all circulating cholesterol not in HDL) and ApoB or reducing the ApoB/ApoA-I ratio.
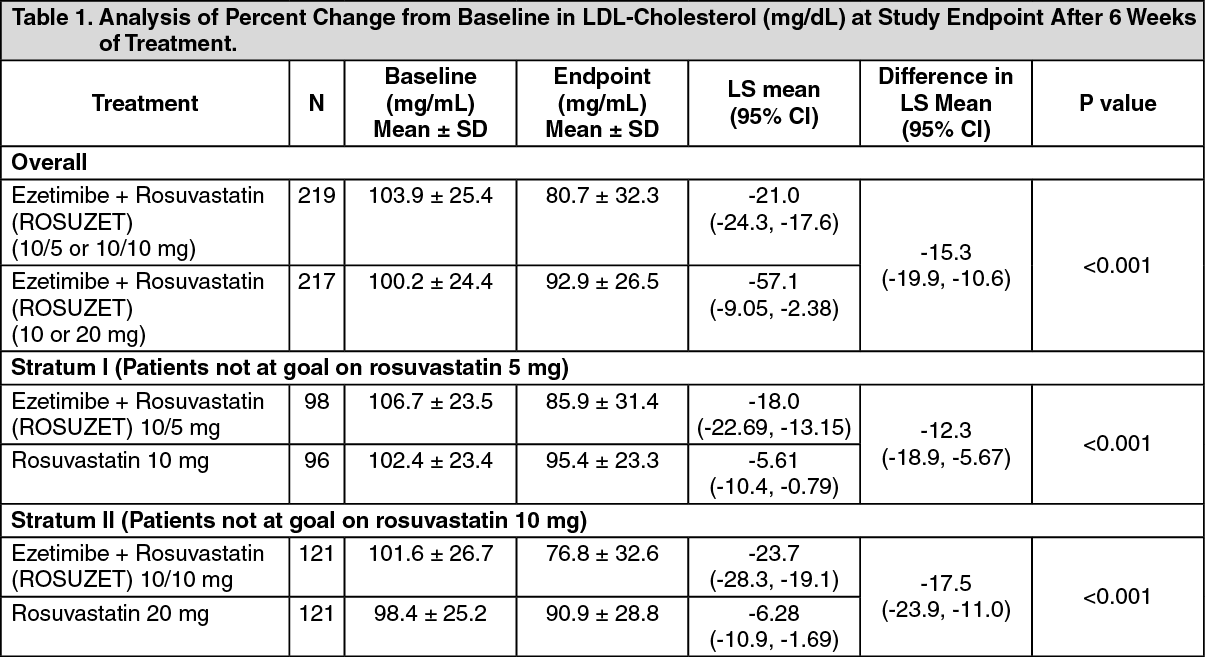
Clinical Studies: Primary Hypercholesterolemia: Ezetimibe + Rosuvastatin (ROSUZET): Ezetimibe Add-on to On-going Rosuvastatin Therapy (Titration Studies): In a multicenter, randomized, double-blind, 6 week-active comparator study (ACTE), 440 subjects at moderately high/high risk of coronary heart disease with LDL cholesterol levels failing to reach their LDL-C goal (100 mg/dL [<2.6 mmol/L] or 70 mg/dL [<1.8 mmol/L] depending on baseline characteristics) were stratified to treatment with rosuvastatin 5 mg or 10 mg for 4-5 weeks. Patients were then randomized to either doubling of their rosuvastatin dose (to 10 mg or 20 mg) or adding ezetimibe 10 mg to their rosuvastatin (5 or 10 mg) therapy, equivalent to Ezetimibe + Rosuvastatin (ROSUZET) 10/5 or 10/10.
Patients taking doses of ezetimibe and rosuvastatin equivalent to Ezetimibe + Rosuvastatin (ROSUZET) 10/5 or 10/10 achieved significantly greater LDL-C reductions compared to patients doubling the initial dose of rosuvastatin (to 10 mg or 20 mg) (p <0.001). The LS mean percent change in LDL-C from baseline to the study end was -20.96% when ezetimibe 10 mg was added to rosuvastatin and -5.71% when the original rosuvastatin dose was doubled (data pooled across the rosuvastatin 5 mg and 10 mg strata). The LS mean treatment difference was -15.25% with a 95% CI (-19.89, -10.60) (Table 1). (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Patients taking doses of ezetimibe and rosuvastatin equivalent to Ezetimibe + Rosuvastatin (ROSUZET) 10/5 or 10/10 significantly lowered total-cholesterol, non-HDL-C and Apo B, compared with doubling of the baseline dose of rosuvastatin (p <0.001) and resulted in a significantly greater proportion of patients reaching LDL-C goal compared with doubling the baseline dose of rosuvastatin (10 mg or 20 mg) (59.4% vs. 30.9%; p <0.001), where the LDL-C goal was <100 mg/dL (<2.6 mmol/L) for patients at moderately high risk/high risk for CHD without atherosclerotic vascular disease (AVD) and <70 mg/dL (<1.8 mmol/L) for patients at very high risk for CHD with AVD. In addition, there was a significantly greater proportion of patients reaching a LDL-C goal of <70 mg/dL (<1.8 mmol/L), regardless of risk status, in patients receiving Ezetimibe + Rosuvastatin (ROSUZET), compared with those receiving a doubling of the baseline rosuvastatin dose (43.8% vs. 17.5%; p <0.001). (See Figure 1.)
Click on icon to see table/diagram/image
Study of Efficacy and Safety of the Ezetimibe/Rosuvastatin Fixed-dose Combination: In a multi-center, 8-week, double-blind, Phase 3 study, 412 Korean hypercholesterolemic subjects were randomized to treatment with a fixed-dose combination of ezetimibe 10 mg plus rosuvastatin at doses of 5 mg, 10 mg or 20 mg or rosuvastatin monotherapy at doses of 5 mg, 10 mg or 20 mg.
Patients taking the fixed-dose combination of ezetimibe plus rosuvastatin achieved significantly greater LDL-C reductions compared to patients treated with rosuvastatin alone pooled across doses (p<0.0001) and at each dose comparison (p≤ 0.01) (Table 2). (See Table 2.)
Click on icon to see table/diagram/image
Pooled across doses, the fixed-dose combination of ezetimibe plus rosuvastatin lowered total cholesterol, non-HDL cholesterol, apolipoprotein B, and triglyceride levels more than rosuvastatin alone.
In addition, pooled across doses, treatment with ezetimibe/rosuvastatin resulted in a greater proportion of subjects reaching LDL-C goal compared with rosuvastatin alone (Table 3). The results for individual dose comparisons are shown in Table 4. (See Tables 3 and 4.)
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Ezetimibe: Monotherapy: In two multicenter, double-blind, placebo-controlled, 12-week studies in 1719 patients with primary hypercholesterolemia, ezetimibe 10 mg significantly lowered total-C (-13%), LDL-C (-19%), Apo B (-14%), TG (-8%), and non-HDL-C (-17%) and increased HDL-C (+3%) compared to placebo. Reduction in LDL-C was consistent across age, sex, race, and baseline LDL-C.
Rosuvastatin: Active-Controlled Study: Rosuvastatin was compared with the HMG-CoA reductase inhibitors atorvastatin, simvastatin, and pravastatin in a multicenter, open-label, dose-ranging study of 2240 patients with hyperlipidemia or mixed dyslipidemia. After randomization, patients were treated for 6 weeks with a single daily dose of either rosuvastatin, atorvastatin, simvastatin, or pravastatin (Figure 2). (See Figure 2.)
Click on icon to see table/diagram/image
JUPITER: In the Justification for the Use of Statins in Primary Prevention: An Intervention Trial Evaluating Rosuvastatin (JUPITER) study, the effect of rosuvastatin on the occurrence of major atherosclerotic cardiovascular disease events was assessed in 17,802 men (≥ 50 years) and women (≥ 60 years). Patients were randomly assigned to placebo (n=8901) or rosuvastatin 20 mg once daily (n=8901) and were followed for a mean duration of 2 years.
The primary end point was a composite end point consisting of the time-to-first occurrence of any of the following major CV events: CV death, nonfatal myocardial infarction, nonfatal stroke, hospitalization for unstable angina or an arterial revascularization procedure.
Rosuvastatin significantly reduced the risk of major CV events (252 events in the placebo group vs. 142 events in the rosuvastatin group) with a statistically significant (p<0.001) relative risk reduction of 44% and absolute risk reduction of 1.2% (see Figure 3). The risk reduction for the primary end point was consistent across the following predefined subgroups: age, sex, race, smoking status, family history of premature CHD, body mass index, LDL-C, HDL-C, and hsCRP levels.
The individual components of the primary end point are presented in Figure 4. Rosuvastatin significantly reduced the risk of nonfatal myocardial infarction, nonfatal stroke and arterial revascularization procedures. There were no significant treatment differences between the rosuvastatin and placebo groups for death due to cardiovascular causes or hospitalizations for unstable angina. (See Figures 3 and 4.)
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
The incremental benefit of Ezetimibe + Rosuvastatin (ROSUZET) on cardiovascular morbidity and mortality over and above that demonstrated for rosuvastatin has not been established.
Homozygous Familial Hypercholesterolemia (HoFH): Ezetimibe: A study was conducted to assess the efficacy of ezetimibe in the treatment of HoFH. This double-blind, randomized, 12-week study enrolled 50 patients with a clinical and/or genotypic diagnosis of HoFH, with or without concomitant LDL apheresis, already receiving atorvastatin or simvastatin (40 mg). Patients were randomized to one of three treatment groups, atorvastatin or simvastatin (80 mg), ezetimibe 10 mg administered with atorvastatin or simvastatin (40 mg), or ezetimibe 10 mg administered with atorvastatin or simvastatin (80 mg). Ezetimibe, administered with atorvastatin (40 or 80 mg) or simvastatin (40 or 80 mg), produced a reduction of LDL-C of 21% from baseline compared with increasing the dose of simvastatin or atorvastatin monotherapy from 40 to 80 mg, which resulted in a reduction of LDL-C of 7% from baseline. In those treated with ezetimibe plus 80mg atorvastatin or with ezetimibe plus 80mg simvastatin, LDL-C was reduced by 27%.
Rosuvastatin: In an open-label, forced-titration study, HoFH patients (n=40, 8-63 years) were evaluated for their response to rosuvastatin 20 to 40 mg titrated at a 6-week interval. In the overall population, the mean LDL-C reduction from baseline was 22%. About one-third of the patients benefited from increasing their dose from 20 mg to 40 mg with further LDL lowering of greater than 6%. In the 27 patients with at least a 15% reduction in LDL-C, the mean LDL-C reduction was 30% (median 28% reduction). Among 13 patients with an LDL-C reduction of <15%, 3 had no change or an increase in LDL-C. Reductions in LDL-C of 15% or greater were observed in 3 of 5 patients with known receptor negative status.
Pharmacokinetics: General Introduction: Ezetimibe + Rosuvastatin (ROSUZET): Ezetimibe + Rosuvastatin (ROSUZET) has been shown to be bioequivalent to coadministration of corresponding doses of ezetimibe and rosuvastatin tablets.
Absorption: Ezetimibe: After oral administration, ezetimibe is rapidly absorbed and extensively conjugated to a pharmacologically active phenolic glucuronide (ezetimibe-glucuronide). Mean maximum plasma concentrations (C
max) occur within 1 to 2 hours for ezetimibe-glucuronide and 4 to 12 hours for ezetimibe. The absolute bioavailability of ezetimibe cannot be determined as the compound is virtually insoluble in aqueous media suitable for injection.
Concomitant food administration (high fat or non-fat meals) had no effect on the oral bioavailability of ezetimibe when administered as ezetimibe 10-mg tablets.
Rosuvastatin: Rosuvastatin is administered orally in the active form with peak plasma levels occurring 5 hours after dosing. Exposure increases linearly over the dose range. Absolute bioavailability is 20%. There is minimal accumulation on repeated once daily dosing.
Distribution: Ezetimibe: Ezetimibe and ezetimibe-glucuronide are bound 99.7% and 88 to 92% to human plasma proteins, respectively.
Rosuvastatin: Rosuvastatin is approximately 90% bound to plasma proteins, mostly albumin. The parent compound, accounts for greater than 90% of the circulating active HMG CoA reductase inhibitor activity.
Metabolism: Ezetimibe: Ezetimibe is metabolized primarily in the small intestine and liver via glucuronide conjugation (a phase II reaction) with subsequent biliary excretion. Minimal oxidative metabolism (a phase I reaction) has been observed in all species evaluated. Ezetimibe and ezetimibe-glucuronide are the major drug-derived compounds detected in plasma, constituting approximately 10 to 20 % and 80 to 90 % of the total drug in plasma, respectively. Both ezetimibe and ezetimibe-glucuronide are slowly eliminated from plasma with evidence of significant enterohepatic recycling. The half-life for ezetimibe and ezetimibe-glucuronide is approximately 22 hours.
Rosuvastatin: Rosuvastatin undergoes first pass extraction in the liver, which is the primary site of cholesterol synthesis and LDL-C clearance.
Elimination: Ezetimibe: Following oral administration of
14C-ezetimibe (20 mg) to human subjects, total ezetimibe accounted for approximately 93% of the total radioactivity in plasma. Approximately 78% and 11% of the administered radioactivity were recovered in the feces and urine, respectively, over a 10-day collection period. After 48 hours, there were no detectable levels of radioactivity in the plasma.
Rosuvastatin: Rosuvastatin undergoes limited metabolism (approximately 10%), mainly to the N-desmethyl form, and 90% is eliminated as unchanged drug in the feces with the remainder being excreted in the urine.
Special Populations: Renal Impairment: Ezetimibe After a single 10-mg dose of ezetimibe in patients with severe renal disease (n=8; mean CrCl ≤ 30 mL/min/1.73 m
2), the mean AUC for total ezetimibe was increased approximately 1.5-fold, compared to healthy subjects (n=9).
An additional patient in this study (post-renal transplant and receiving multiple medications, including cyclosporine) had a 12-fold greater exposure to total ezetimibe.
Rosuvastatin: In a study in subjects with varying degrees of renal impairment, mild to moderate renal disease had little influence on plasma concentrations of rosuvastatin. However, subjects with severe impairment (CrCI <30 mL/min) had a 3-fold increase in plasma concentration compared to healthy volunteers.
Hepatic Impairment: Ezetimibe: After a single 10-mg dose of ezetimibe, the mean area under the curve (AUC) for total ezetimibe was increased approximately 1.7-fold in patients with mild hepatic impairment (Child-Pugh score 5 or 6), compared to healthy subjects. In a 14-day, multiple-dose study (10 mg daily) in patients with moderate hepatic impairment (Child-Pugh score 7 to 9), the mean AUC for total ezetimibe was increased approximately 4-fold on Day 1 and Day 14 compared to healthy subjects. No dosage adjustment is necessary for patients with mild hepatic impairment. Due to the unknown effects of the increased exposure to ezetimibe in patients with moderate or severe (Child-Pugh score >9) hepatic impairment, ezetimibe is not recommended in these patients [see Hepatic Impairment under PRECAUTIONS].
Rosuvastatin: In a study in subjects with varying degrees of hepatic impairment there was no evidence of increased exposure to rosuvastatin other than in the 2 subjects with the most severe liver disease (Child-Pugh scores of 8 and 9). In these subjects systemic exposure was increased by at least 2-fold compared to subjects with lower Child-Pugh scores.
Pediatric: Ezetimibe: The pharmacokinetics of ezetimibe are similar between children ≥ 6 years and adults. Pharmacokinetic data in the pediatric population < 6 years of age are not available.
Rosuvastatin: The exposure in children and adolescents with heterozygous familial hypercholesterolemia appears to be similar to or lower than that in adult patients with dyslipidemia.
Geriatric: Ezetimibe: Plasma concentrations for total ezetimibe are about 2-fold higher in the elderly (≥ 65 years) than in the young (18 to 45 years). LDL-C reduction and safety profile are comparable between elderly and young subjects treated with ezetimibe.
Rosuvastatin: There was no clinically relevant effect of age on the pharmacokinetics of rosuvastatin in adults.
Race: Ezetimibe: Based on a meta analysis of pharmacokinetic studies with ezetimibe, there were no pharmacokinetic differences between Blacks and Caucasians.
Rosuvastatin: Pharmacokinetic studies show an approximate 2-fold elevation in median AUC in Asian subjects compared with Caucasians.
A population pharmacokinetic analysis revealed no clinically relevant differences in pharmacokinetics among Caucasian, Hispanic and Black or Afro-Caribbean groups.
Sex: Ezetimibe: Plasma concentrations for total ezetimibe are slightly higher (<20 %) in women than in men. LDL-C reduction and safety profile are comparable between men and women treated with ezetimibe.
Rosuvastatin: There was no clinically relevant effect of sex on the pharmacokinetics of rosuvastatin in adults.
Genetic polymorphisms: Disposition of HMG-CoA reductase inhibitors, including rosuvastatin, involves OATP181 and BCRP transporter proteins. In patients with SLCO181 (OATP181) and/or ABCG2 (BCRP) genetic polymorphisms there is a risk of increased rosuvastatin exposure. Individual polymorphisms of SLCO181 c.521 CC and ABCG2 c.421AA are associated with an approximate 1.6-fold higher rosuvastatin exposure (AUC) or 2.4-fold higher exposure, respectively, compared to the SLCO1 B1 c.521 TT or ABCG2. c.421 CC genotypes.
Toxicology: Preclinical Safety Data: Rosuvastatin Preclinical data reveal no special hazards for humans based on conventional studies of safety pharmacology, repeat-dose toxicity, genotoxicity, carcinogenic potential and reproductive toxicity.




 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image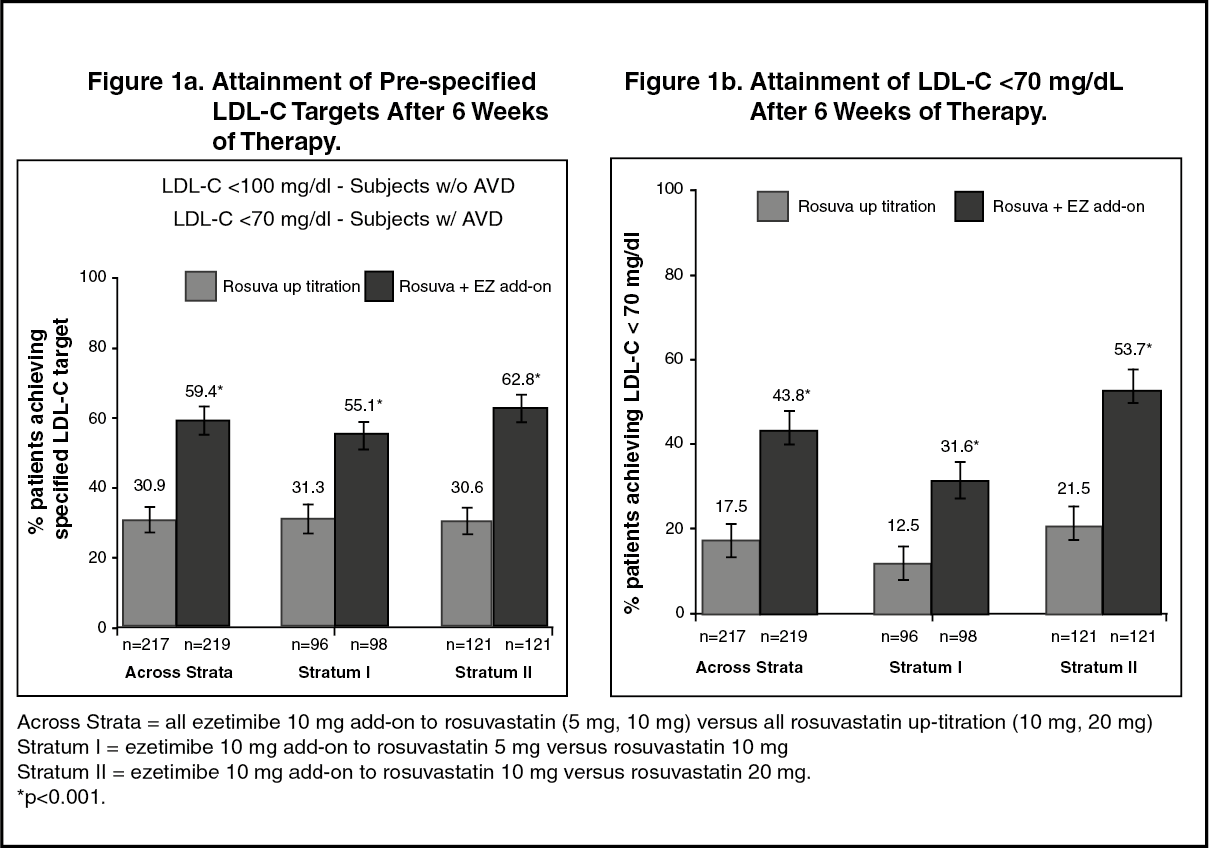 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image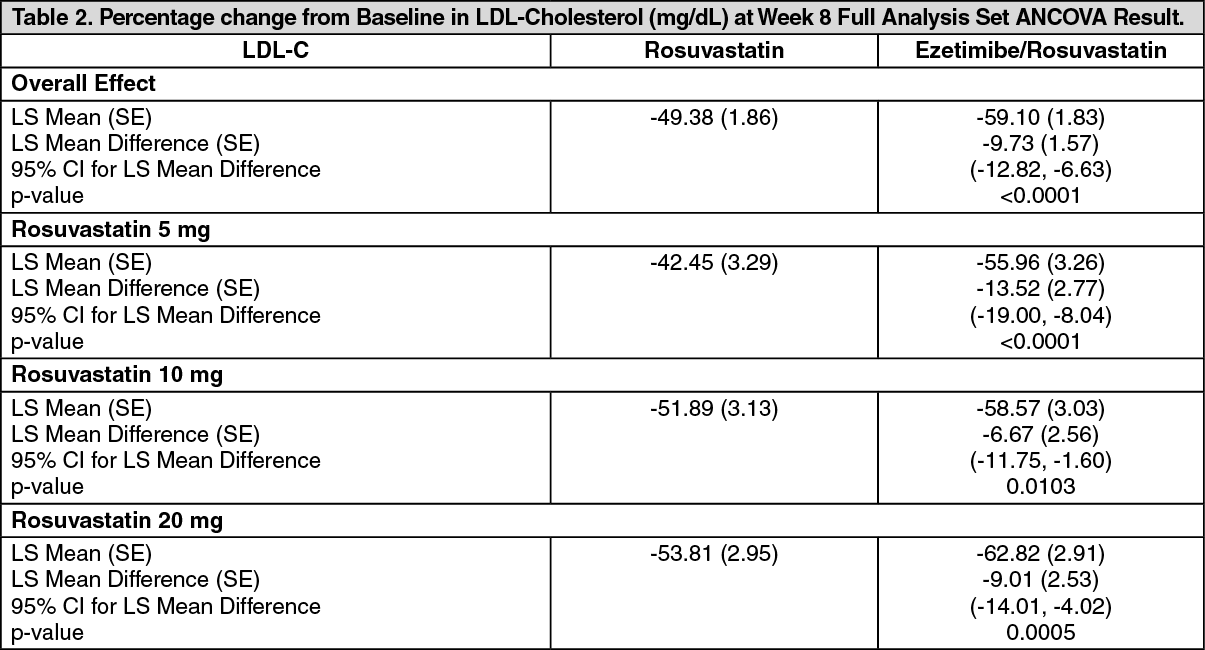 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image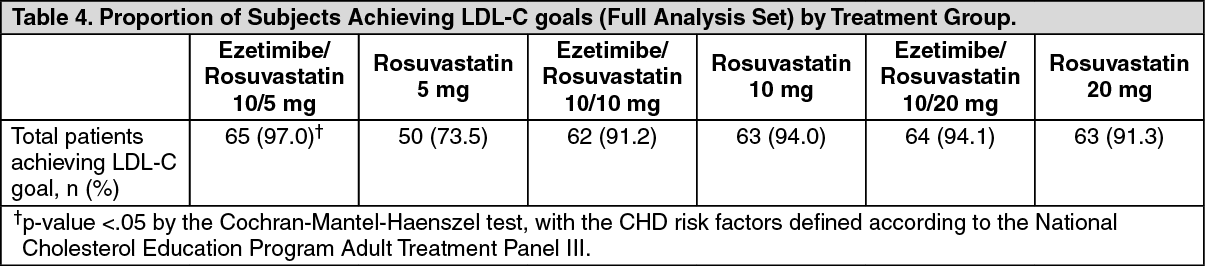 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image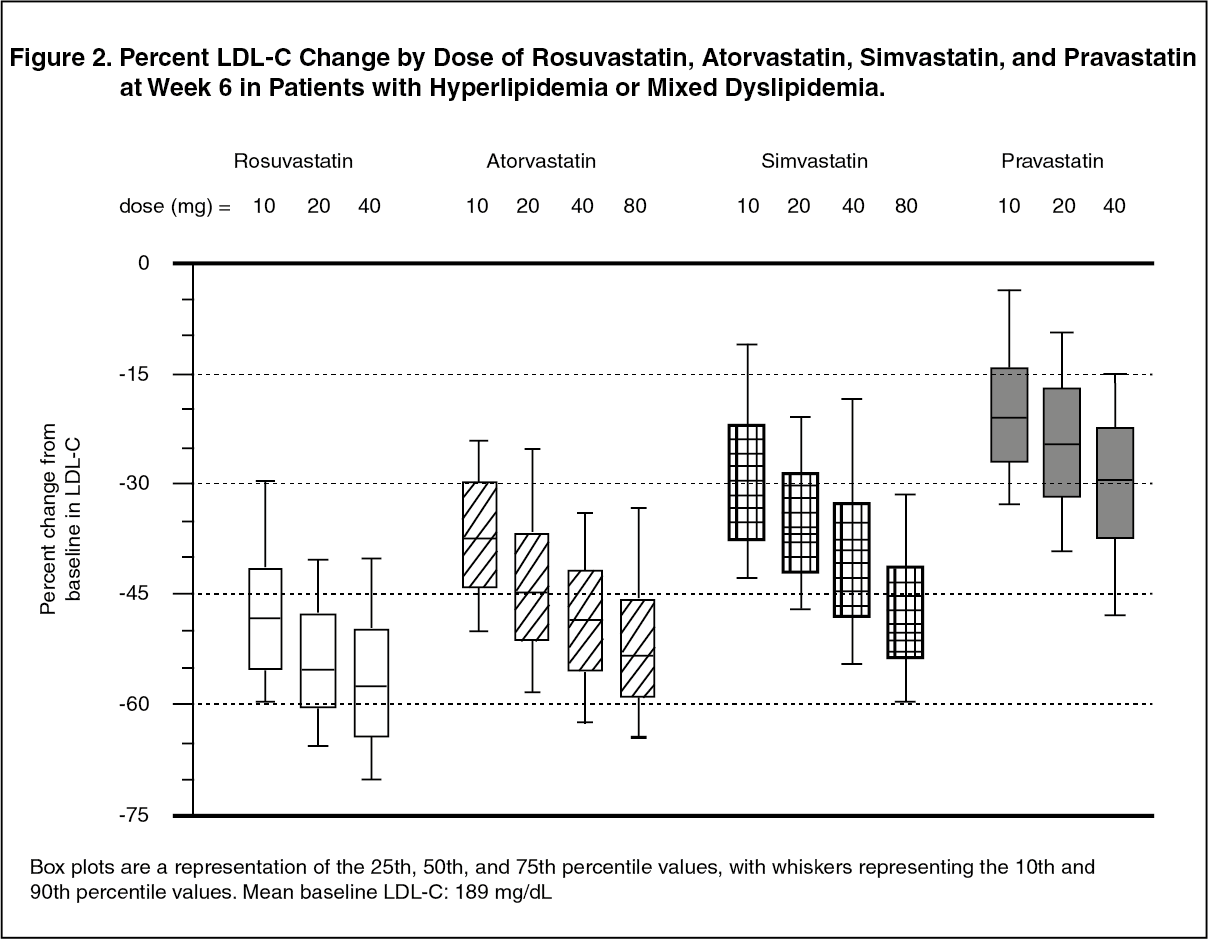 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image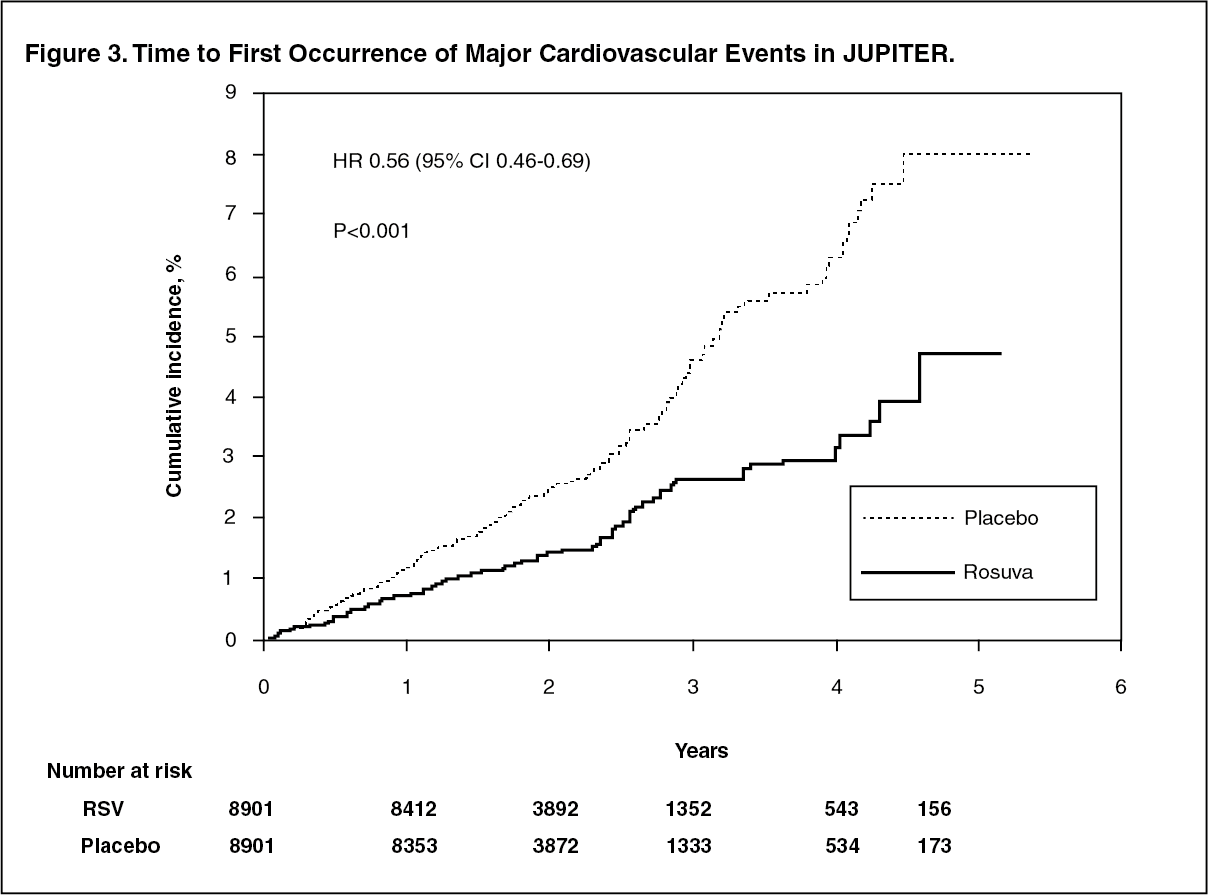 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image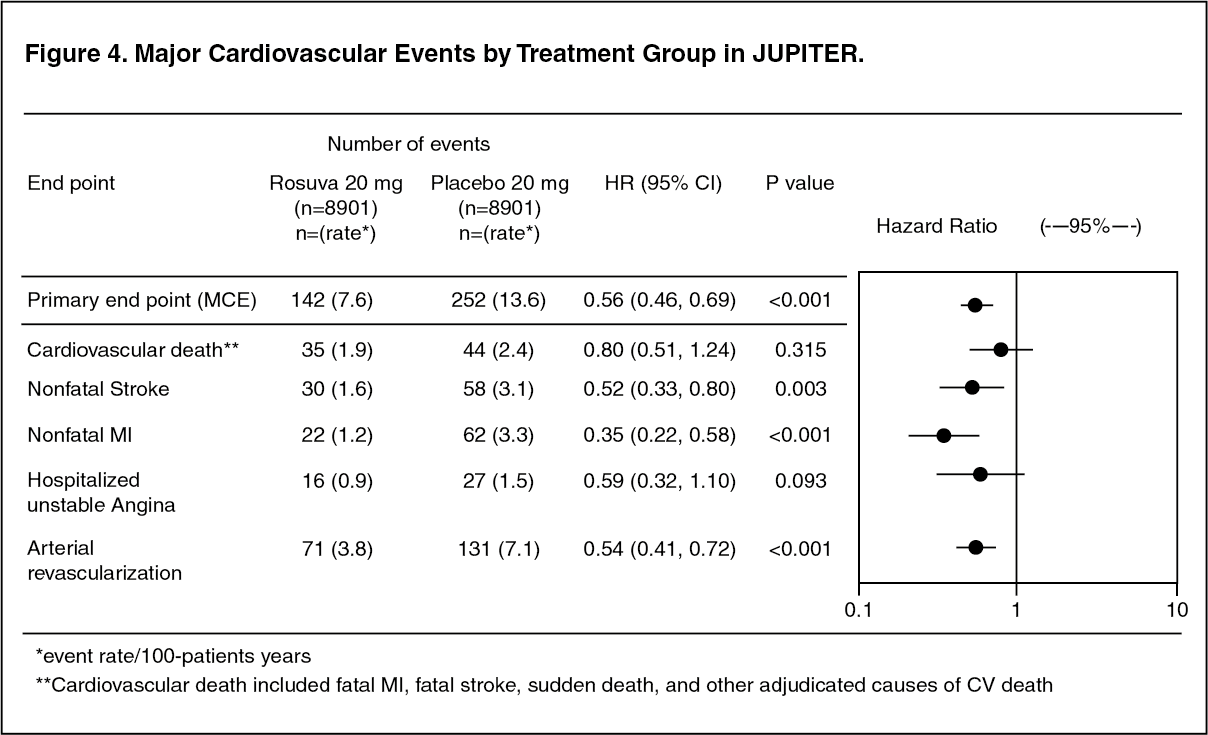 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image


 Sign Out
Sign Out
