


 Sign Out
Sign Out



Multiple mechanisms may contribute to potential interactions with HMG Co-A reductase inhibitors. Drugs or herbal products that inhibit certain enzymes and/or transporter (e.g. OATP1B) pathways may increase rosuvastatin plasma concentrations and may lead to an increased risk of myopathy/rhabdomyolysis.
Consult the prescribing information of all concomitantly used drugs to obtain further information about their potential interactions with rosuvastatin and/or the potential for enzyme or transporter alterations and possible adjustments to dose and regimens.
Ezetimibe: In preclinical studies, it has been shown that ezetimibe does not induce cytochrome P450 drug metabolizing enzymes. No clinically significant pharmacokinetic interactions have been observed between ezetimibe and drugs known to be metabolized by cytochromes P450 1A2, 2D6, 2C8, 2C9, and 3A4, or N-acetyltransferase.
Ezetimibe had no effect on the pharmacokinetics of dapsone, dextromethorphan, digoxin, oral contraceptives (ethinyl estradiol and levonorgestrel), glipizide, tolbutamide, or midazolam during co-administration. Cimetidine, co-administered with ezetimibe, had no effect on the bioavailability of ezetimibe.
Antacids: Concomitant antacid administration decreased the rate of absorption of ezetimibe but had no effect on the bioavailability of ezetimibe. This decreased rate of absorption is not considered clinically significant.
Cholestyramine: Concomitant cholestyramine administration decreased the mean AUC of total ezetimibe (ezetimibe + ezetimibe glucuronide) approximately 55 %. The incremental LDL‑C reduction due to adding ezetimibe to cholestyramine may be lessened by this interaction.
Cyclosporine: In a study of eight post-renal transplant patients with creatinine clearance of >50 mL/min on a stable dose of cyclosporine, a single 10-mg dose of ezetimibe resulted in a 3.4-fold (range 2.3- to 7.9-fold) increase in the mean AUC for total ezetimibe compared to a healthy control population from another study (n=17). In a different study, a renal transplant patient with severe renal insufficiency (creatinine clearance of 13.2 mL/min/1.73 m2) who was receiving multiple medications, including cyclosporine, demonstrated a 12‑fold greater exposure to total ezetimibe compared to concurrent controls. In a two-period crossover study in twelve healthy subjects, daily administration of 20 mg ezetimibe for 8 days with a single 100‑mg dose of cyclosporine on Day 7 resulted in a mean 15% increase in cyclosporine AUC (range 10% decrease to 51% increase) compared to a single 100‑mg dose of cyclosporine alone.
Fibrates: The safety and effectiveness of ezetimibe co-administered with fenofibrate have been evaluated in a clinical study; co-administration of ezetimibe with other fibrates has not been studied. Fibrates may increase cholesterol excretion into the bile, leading to cholelithiasis. In a preclinical study in dogs, ezetimibe increased cholesterol in the gallbladder bile. Although the relevance of this preclinical finding to humans is unknown, co-administration of ezetimibe with fibrates (other than fenofibrate) is not recommended until use in patients is studied.
Fenofibrate: In a pharmacokinetic study, concomitant fenofibrate administration increased total ezetimibe concentrations approximately 1.5‑fold. This increase is not considered clinically significant.
Gemfibrozil: In a pharmacokinetic study, concomitant gemfibrozil administration increased total ezetimibe concentrations approximately 1.7‑ fold. This increase is not considered clinically significant. No clinical data are available.
Statins: No clinically significant pharmacokinetic interactions were seen when ezetimibe was co-administered with atorvastatin, simvastatin, pravastatin, lovastatin, fluvastatin, or rosuvastatin.
Anticoagulants: Concomitant administration of ezetimibe (10 mg once daily) had no significant effect on bioavailability of warfarin and prothrombin time in a study of twelve healthy adult males. There have been post-marketing reports of increased International Normalized Ratio in patients who had ezetimibe added to warfarin or fluindione. Most of these patients were also on other medications [see Anticoagulants under PRECAUTIONS].
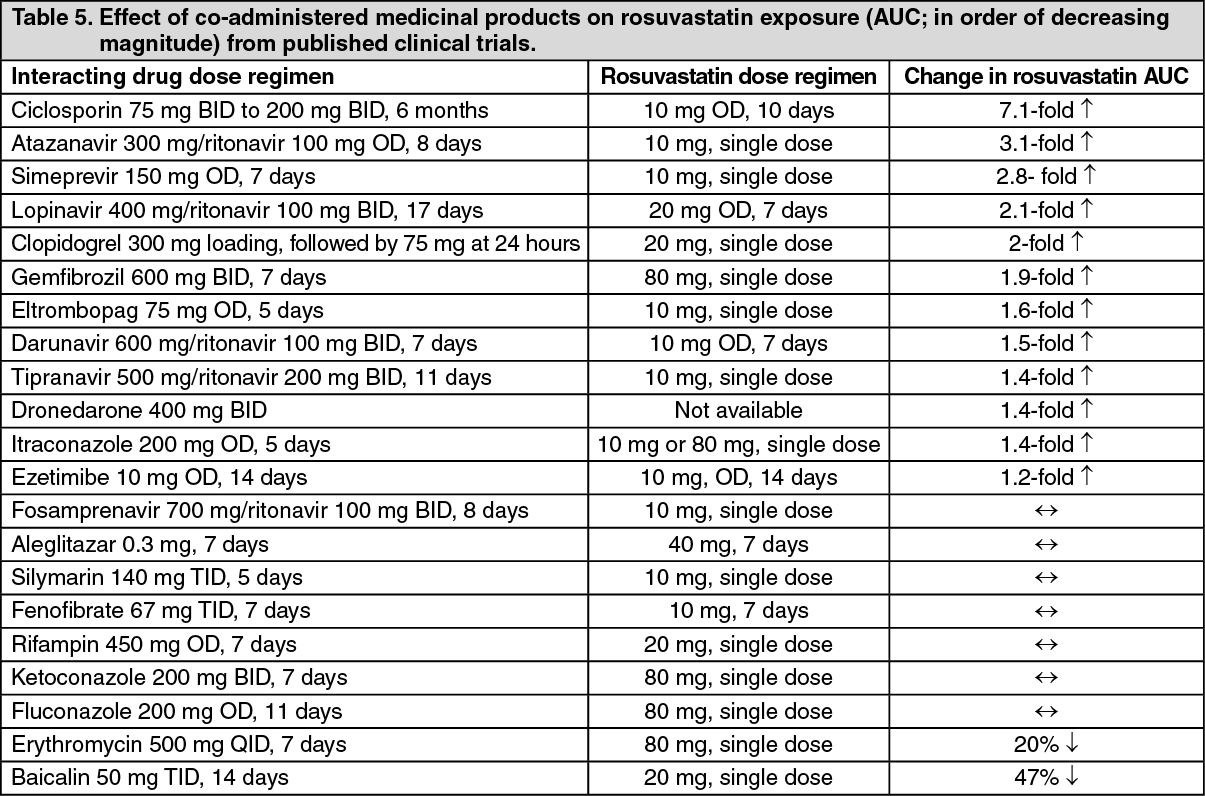
Rosuvastatin: In vitro and in vivo data indicate that rosuvastatin has no clinically significant cytochrome P450 interactions (as a substrate, inhibitor or inducer). Rosuvastatin is a substrate for certain transporter proteins including the hepatic uptake transporter OATP1B1 and efflux transporter BCRP. Concomitant administration of rosuvastatin with medicinal products that are inhibitors of these transporter proteins may result increased rosuvastatin plasma concentrations and an increased risk of myopathy [see Table 5, DOSAGE & ADMINISTRATION and PRECAUTIONS].
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageInteraction requiring rosuvastatin dose adjustments (see also Table 5): When it is necessary to co-administer Ezetimibe + Rosuvastatin (ROSUZET) with other medicinal products known to increase exposure to rosuvastatin, doses of Ezetimibe + Rosuvastatin (ROSUZET) should be adjusted. It is recommended that prescribers consult the relevant product information when considering administration of such products together with Ezetimibe + Rosuvastatin (ROSUZET). Start with a 10/5 mg once daily dose of Ezetimibe + Rosuvastatin (ROSUZET) if the expected increase in exposure (AUC) is approximately 2-fold or higher. The maximum daily dose of Ezetimibe + Rosuvastatin (ROSUZET) should be adjusted so that the expected rosuvastatin exposure would not likely exceed that of a 10/40 mg daily dose of Ezetimibe + Rosuvastatin (ROSUZET) taken without interacting medicinal products, for example a 10/5 mg dose of Ezetimibe + Rosuvastatin (ROSUZET) with ciclosporin (7.1-fold increase in exposure), a 10/10 mg dose of Ezetimibe + Rosuvastatin (ROSUZET) with ritonavir/atazanavir combination (3.1-fold increase) and a 10/20 mg dose of Ezetimibe + Rosuvastatin (ROSUZET) with gemfibrozil (1.9-fold increase). Not all strengths are available locally.
Other interacting medicinal products: Antacid: The simultaneous dosing of rosuvastatin with an antacid suspension containing aluminum and magnesium hydroxide resulted in a decrease in rosuvastatin plasma concentration of approximately 50%. This effect was mitigated when the antacid was dosed 2 hours after rosuvastatin. The clinical relevance of this interaction has not been studied.
Fusidic Acid: Interaction studies with rosuvastatin and fusidic acid have not been conducted. As with other statins, muscle related events, including rhabdomyolysis, have been reported in post-marketing experience with rosuvastatin and fusidic acid given concurrently. Patients should be closely monitored and temporary suspension of rosuvastatin treatment may be appropriate.
Effect of rosuvastatin on co-administered medicinal products: Warfarin: The pharmacokinetics of warfarin are not significantly affected following co-administration with rosuvastatin. However, as with other HMG-CoA reductase inhibitors, co-administration of rosuvastatin and warfarin may result in a rise in INR compared to warfarin alone. In patients taking vitamin K antagonists monitoring of INR is recommended both at initiation or cessation of therapy with rosuvastatin or following dose adjustment.
Fenofibrates/fibric acid derivatives: Although no pharmacokinetic interaction between rosuvastatin and fenofibrate was observed; a pharmacodynamic interaction may occur. Gemfibrozil, fenofibrate and other fibric acids, including nicotinic acid, may increase the risk of myopathy when given concomitantly with HMG-CoA reductase inhibitors [see Fenofibrate under PRECAUTIONS].
Ciclosporin: Co-administration of rosuvastatin with ciclosporin resulted in no significant changes in ciclosporin plasma concentration.
Other medications: There was no clinically significant interactions with an oral contraceptive, digoxin, or ezetimibe or fenofibrate.
In clinical studies rosuvastatin was co-administered with antihypertensive agents, antidiabetic agents and hormone replacement therapy. These studies did not produce any evidence of clinically significant adverse interactions.
Daptomycin: The risk of myopathy and/or rhabdomyolysis may be increased by concomitant administration of HMG-CoA reductase inhibitors and daptomycin [see PRECAUTIONS].