Therapeutic Class: Pembrolizumab (KEYTRUDA) is an antineoplastic agent, monoclonal antibody.
Pharmacology: Mechanism of Action: PD-1 is an immune-checkpoint receptor that limits the activity of T lymphocytes in peripheral tissues. The PD-1 pathway is an immune control checkpoint that may be engaged by tumor cells to inhibit active T-cell immune surveillance. Pembrolizumab (KEYTRUDA) is a high affinity antibody against PD-1, which exerts dual ligand blockade of the PD-1 pathway, including PD-L1 and PD-L2, on antigen presenting or tumor cells. By inhibiting the PD-1 receptor from binding to its ligands, Pembrolizumab (KEYTRUDA) reactivates tumor-specific cytotoxic T lymphocytes in the tumor microenvironment and reactivates anti-tumor immunity.
The anti-angiogenic effect of lenvatinib (multi-TKI) in combination with the immune-stimulatory effect of pembrolizumab (anti-PD-1) results in a tumor microenvironment with greater Tcell activation to help overcome primary and acquired resistance to immunotherapy and may improve tumor responses compared to either treatment alone.
In preclinical murine models, PD-1 plus TKI inhibitors have demonstrated enhanced anti-tumor activity compared to either agent alone.
Pharmacodynamics: Based on the modeling of dose/exposure relationships for efficacy and safety for pembrolizumab, there are no clinically significant differences in efficacy and safety between the doses of 200 mg or 2 mg/kg every 3 weeks or 400 mg every 6 weeks.
In peripheral blood of patients who received Pembrolizumab (KEYTRUDA) 2 mg/kg every 3 weeks or 10 mg/kg every 2 weeks or 3 weeks, an increased percentage of activated (i.e., HLA-DR+) CD4+ and CD8+ T-cells was observed after treatment at all doses and schedules without an increase in the circulating T-lymphocyte number.
Clinical Studies: Clinical efficacy and safety: Melanoma: KEYNOTE-006: Controlled trial in melanoma patients naïve to treatment with ipilimumab: The safety and efficacy of Pembrolizumab (KEYTRUDA) were investigated in KEYNOTE-006, a multicenter, controlled, Phase III study for the treatment of unresectable or metastatic melanoma in patients who were naïve to ipilimumab and who received no or one prior systemic therapy. Patients were randomized (1:1:1) to receive Pembrolizumab (KEYTRUDA) at a dose of 10 mg/kg every 2 (n=279) or 3 weeks (n=277) or ipilimumab (n=278). Randomization was stratified by line of therapy, ECOG performance status, and PD-L1 expression status. The study excluded patients with autoimmune disease or those receiving immunosuppression; previous severe hypersensitivity to other monoclonal antibodies; and HIV, hepatitis B or hepatitis C infection. Patients with BRAF V600E mutant melanoma were not required to have received prior BRAF inhibitor therapy.
Patients were treated with Pembrolizumab (KEYTRUDA) until disease progression or unacceptable toxicity. Clinically stable patients with initial evidence of disease progression were permitted to remain on treatment until disease progression was confirmed. Assessment of tumor status was performed at 12 weeks, then every 6 weeks through Week 48, followed by every 12 weeks thereafter.
Of the 834 patients in KEYNOTE-006, 60% were male, 44% were ≥65 years (median age was 62 years [range 18-89]) and 98% were white. Sixty-six percent had no prior systemic therapies and thus received study therapy as first-line treatment whereas 34% had one prior therapy and thus received study therapy as second-line treatment. Thirty-one percent had an ECOG PS of 1 and 69% had an ECOG PS of 0. Eighty percent of patients were PD-L1 positive (PD-L1 membrane expression in ≥1% of tumor and associated immune cells as assessed prospectively by an immunohistochemistry assay with the 22C3 anti-PDL1 antibody) and 18% were PD-L1 negative. Sixty-five percent of patients had M1c stage, 32% had elevated LDH and 9% had brain metastases. BRAF mutations were reported in 302 (36%) patients. Among patients with BRAF mutant tumors, 139 (46%) were previously treated with a BRAF inhibitor. Baseline characteristics were well-balanced across treatment arms.
The primary efficacy outcome measures were overall survival (OS) and progression-free survival (PFS; as assessed by Integrated Radiology and Oncology Assessment [IRO] review using Response Evaluation Criteria in Solid Tumors [RECIST 1.1]). Secondary efficacy outcome measures were overall response rate (ORR) and response duration. Table 1 summarizes key efficacy measures. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
The final analysis was performed after all patients had at least 21 months of follow-up. The final OS analysis was performed after 383 patient events [119 for Pembrolizumab (KEYTRUDA) 10 mg/kg every 3 weeks, 122 for Pembrolizumab (KEYTRUDA) 10 mg/kg every 2 weeks and 142 for ipilimumab]. The OS HRs vs. ipilimumab were 0.68 (95% CI: 0.53, 0.86; p<0.001) for patients treated with Pembrolizumab (KEYTRUDA) 10 mg/kg every 3 weeks and 0.68 (95% CI: 0.53, 0.87; p<0.001) for patients treated with Pembrolizumab (KEYTRUDA) 10 mg/kg every 2 weeks. The OS rate at 18 months and 24 months were 62% and 55% respectively for Pembrolizumab (KEYTRUDA) 10 mg/kg every 3 weeks, 60% and 55% respectively for Pembrolizumab (KEYTRUDA) 10 mg/kg every 2 weeks, and 47% and 43% respectively for ipilimumab. At the final analysis, a long-term PFS analysis was performed based on 566 patient events [183 for Pembrolizumab (KEYTRUDA) 10 mg/kg every 3 weeks, 181 for Pembrolizumab (KEYTRUDA) 10 mg/kg every 2 weeks and 202 for ipilimumab]. The PFS HRs vs. ipilimumab were 0.61 (95% CI: 0.50, 0.75) for patients treated with Pembrolizumab (KEYTRUDA) 10 mg/kg every 3 weeks and 0.61 (95% CI: 0.50, 0.75) for patients treated with Pembrolizumab (KEYTRUDA) 10 mg/kg every 2 weeks. (See Figures 1 and 2.) The percentage of responders with an ongoing response at 18 months was 68% for Pembrolizumab (KEYTRUDA) 10 mg/kg every 3 weeks, 71% for Pembrolizumab (KEYTRUDA) 10 mg/kg every 2 weeks and 70% for ipilimumab. (See Figures 1 and 2.)
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Sub-population analysis by BRAF mutation status: A subgroup analysis was performed as part of the final analysis of KEYNOTE-006 in patients who were BRAF wild type, BRAF mutant without prior BRAF treatment and BRAF mutant with prior BRAF treatment. The PFS hazard ratios (HRs) (pooled Pembrolizumab (KEYTRUDA) [10 mg/kg every 2 or 3 weeks] vs. ipilimumab) were 0.61 (95% CI: 0.49, 0.76) for BRAF wild type, 0.52 (95% CI: 0.35, 0.78) for BRAF mutant without prior BRAF treatment, and 0.76 (95% CI: 0.51, 1.14) for BRAF mutant with prior BRAF treatment. The OS HRs for pooled Pembrolizumab (KEYTRUDA) vs. ipilimumab were 0.68 (95% CI: 0.52, 0.88) for BRAF wild type, 0.70 (95% CI: 0.40, 1.22) for BRAF mutant without prior BRAF treatment, and 0.66 (95% CI: 0.41, 1.04) for BRAF mutant with prior BRAF treatment. ORR for pooled Pembrolizumab (KEYTRUDA) vs. ipilimumab was 38% vs. 14% for BRAF wild type, 41% vs. 15% for BRAF mutant without prior BRAF treatment, and 24% vs. 10% for BRAF mutant with prior BRAF treatment.
Sub-population analysis by PD-L1 status: A subgroup analysis was performed as part of the final analysis of KEYNOTE006 in patients who were PD-L1 positive vs. PD-L1 negative. The PFS HRs (pooled Pembrolizumab (KEYTRUDA) [10 mg/kg every 2 or 3 weeks] vs. ipilimumab) were 0.53 (95% CI: 0.44, 0.65) for PD-L1 positive patients and 0.87 (95% CI: 0.58, 1.30) for PD-L1 negative patients. The OS HRs for pooled Pembrolizumab (KEYTRUDA) vs. ipilimumab were 0.63 (95% CI: 0.50, 0.80) for PD-L1 positive patients and 0.76 (95% CI: 0.48, 1.19) for PD-L1 negative patients.
KEYNOTE-002: Controlled trial in melanoma patients previously treated with ipilimumab: The safety and efficacy of Pembrolizumab (KEYTRUDA) were investigated in KEYNOTE-002, a multicenter, controlled study for the treatment of unresectable or metastatic melanoma in patients previously treated with ipilimumab and if BRAF V600 mutation-positive, a BRAF or MEK inhibitor. Patients were randomized (1:1:1) to receive Pembrolizumab (KEYTRUDA) at a dose of 2 (n=180) or 10 mg/kg (n=181) every 3 weeks or chemotherapy (n=179; including dacarbazine, temozolomide, carboplatin, paclitaxel, or carboplatin+paclitaxel). The study excluded patients with autoimmune disease or those receiving immunosuppression; a history of severe or life-threatening immune-mediated adverse reactions from treatment with ipilimumab, defined as any Grade 4 toxicity or Grade 3 toxicity requiring corticosteroid treatment (greater than 10 mg/day prednisone or equivalent dose) for greater than 12 weeks; previous severe hypersensitivity to other monoclonal antibodies; a history of pneumonitis or interstitial lung disease; HIV, hepatitis B or hepatitis C infection.
Patients were treated with Pembrolizumab (KEYTRUDA) until disease progression or unacceptable toxicity. Clinically stable patients with initial evidence of disease progression were permitted to remain on treatment until disease progression was confirmed. Assessment of tumor status was performed at 12 weeks, then every 6 weeks through Week 48, followed by every 12 weeks thereafter. Patients on chemotherapy who experienced independently-verified progression of disease after the first scheduled disease assessment were able to crossover and receive 2 mg/kg or 10 mg/kg of Pembrolizumab (KEYTRUDA) every 3 weeks in a double-blind fashion.
Of the 540 patients in KEYNOTE-002, 61% were male, 43% were ≥65 years (median age was 62 years [range 15-89]) and 98% were white. Eighty-two percent of patients had M1c stage, 73% had at least two and 32% had three or more prior systemic therapies for advanced melanoma. Forty-five percent had an ECOG PS of 1, 40% had elevated LDH and 23% had a BRAF mutated tumor. Baseline characteristics were well-balanced across treatment arms.
The primary efficacy outcome measures were PFS (as assessed by IRO review using RECIST 1.1) and OS. Secondary efficacy outcome measures were PFS (as assessed by Investigator using RECIST 1.1), ORR and response duration. Table 2 summarizes key efficacy measures in patients previously treated with ipilimumab. There was no statistically significant difference between Pembrolizumab (KEYTRUDA) and chemotherapy in the final OS analysis that was not adjusted for the potentially confounding effects of crossover. Of the patients randomized to the chemotherapy arm, 55% crossed over and subsequently received treatment with Pembrolizumab (KEYTRUDA). (See Table 2.)
Click on icon to see table/diagram/image
At the final analysis, a long-term PFS analysis was performed based on 466 PFS events (150 for Pembrolizumab (KEYTRUDA) 2 mg/kg every 3 weeks; 144 for Pembrolizumab (KEYTRUDA) 10 mg/kg every 3 weeks and 172 for chemotherapy). The PFS HRs vs. chemotherapy were 0.58 (95% CI: 0.46,0.73) for patients treated with Pembrolizumab (KEYTRUDA) 2 mg/kg every 3 weeks and 0.47 (95% CI: 0.37, 0.60 for patients treated with Pembrolizumab (KEYTRUDA) 10 mg/kg every 3 weeks (Figure 3). (See Figure 3.)
Click on icon to see table/diagram/image
KEYNOTE-001: Open-label study in melanoma patients: The safety and efficacy of Pembrolizumab (KEYTRUDA) were also investigated in an uncontrolled, open-label study for the treatment of unresectable or metastatic melanoma. Efficacy was evaluated for 276 patients from two defined cohorts of KEYNOTE-001, one which included patients previously treated with ipilimumab (and if BRAF V600 mutation-positive, a BRAF or MEK inhibitor) and another which included patients naïve to treatment with ipilimumab. Patients were randomized to receive Pembrolizumab (KEYTRUDA) at a dose of 2 mg/kg every 3 weeks or 10 mg/kg every 3 weeks. Patients were treated with Pembrolizumab (KEYTRUDA) until disease progression or unacceptable toxicity. Clinically stable patients with initial evidence of disease progression were permitted to remain on treatment until disease progression was confirmed. Exclusion criteria were similar to those of KEYNOTE-002.
Of the 89 patients receiving 2 mg/kg of Pembrolizumab (KEYTRUDA) who were previously treated with ipilimumab, 53% were male, 33% were ≥65 years of age and the median age was 59 years (range 18-88). All but two patients were white. Eighty-four percent of patients had M1c stage and 8% had a history of brain metastases. Seventy-eight percent of patients had at least two and 35% had three or more prior systemic therapies for advanced melanoma. BRAF mutations were reported in 13% of the study population.
Of the 51 patients receiving 2 mg/kg of Pembrolizumab (KEYTRUDA) who were naïve to treatment with ipilimumab, 63% were male, 35% were ≥65 years of age and the median age was 60 years (range 35-80). All but one patient was white. Sixty-three percent of patients had M1c stage and 2% had a history of brain metastases. Forty-five percent had no prior therapies for advanced melanoma. BRAF mutations were reported in 39% of the study population.
The primary efficacy outcome measure was ORR as assessed by independent review using confirmed responses and RECIST 1.1. Secondary efficacy outcome measures were disease control rate (DCR; including complete response, partial response and stable disease), response duration, PFS, and OS. Tumor response was assessed at 12-week intervals. Table 3 summarizes key efficacy measures in patients, previously treated or naïve to treatment with ipilimumab, receiving Pembrolizumab (KEYTRUDA) at a dose of 2 mg/kg based on a minimum follow-up time of 30 months for all patients. (See Table 3.)
Click on icon to see table/diagram/image
Results for patients previously treated with ipilimumab (n=84) and naïve to treatment with ipilimumab (n=52) who received 10 mg/kg of Pembrolizumab (KEYTRUDA) every 3 weeks were similar to those seen in patients who received 2 mg/kg of Pembrolizumab (KEYTRUDA) every 3 weeks.
KEYNOTE-716: Placebo-controlled trial for the adjuvant treatment of patients with completely resected Stage IIB or IIC melanoma: The efficacy of Pembrolizumab (KEYTRUDA) was investigated in KEYNOTE-716, a multicenter, randomized, double-blind, placebo-controlled trial in patients with completely resected stage IIB or IIC melanoma. A total of 976 patients were randomized (1:1) to receive Pembrolizumab (KEYTRUDA) 200 mg or the pediatric (≥12 years old) dose of Pembrolizumab (KEYTRUDA) 2 mg/kg intravenously (up to a maximum of 200 mg) every three weeks (n=487) or placebo (n=489) for up to one year until disease recurrence or unacceptable toxicity. Randomization was stratified by American Joint Committee on Cancer 7th edition (AJCC) T stage. Patients must not have been previously treated for melanoma beyond complete surgical resection for their melanoma prior to study entry. Patients with active autoimmune disease or a medical condition that required immunosuppression or mucosal or ocular melanoma were ineligible. Patients underwent imaging every 6 months for 1 year from randomization, every 6 months from years 2 to 4, and then once in year 5 from randomization or until recurrence, whichever came first.
Among the 976 patients, the baseline characteristics were: median age of 61 years (range: 16 to 87), 39% age 65 or older; 60% male; and 93% ECOG PS of 0 and 7% ECOG PS of 1. Sixty-four percent had stage IIB and 35% had stage IIC.
The primary efficacy outcome measure was investigator-assessed recurrence free survival (RFS) in the whole population, where RFS was defined as the time between the date of randomization and the date of first recurrence (local, regional, or distant metastasis) or death, whichever occurs first. The secondary outcome measures were distant metastasis-free survival (DMFS) and OS in the whole population. DMFS and OS were not formally assessed at the time of this analysis.
The trial initially demonstrated a statistically significant improvement in RFS for patients randomized to the pembrolizumab arm compared with placebo. These efficacy results are summarized in Table 4. (See Table 4.)
Click on icon to see table/diagram/image
A pre-specified sensitivity analysis of RFS that included new primary melanomas was consistent with the primary RFS analysis, with an HR of 0.64 (95% CI: 0.46, 0.88).
An updated RFS analysis was performed with a median follow-up of 20.5 months (range: 4.6 to 32.7 months). At the time of this analysis, the hazard ratio in patients randomized to pembrolizumab versus patients randomized to placebo was 0.61 (95% CI: 0.45, 0.82) with 72/487 (14.8%) events and 115/489 (23.5%), respectively. These efficacy results are summarized in Figure 4. (See Figure 4.)
Click on icon to see table/diagram/image
KEYNOTE-054: Placebo-controlled trial for the adjuvant treatment of patients with completely resected Stage III melanoma: The efficacy of Pembrolizumab (KEYTRUDA) was evaluated in KEYNOTE-054, a multicenter, randomized double-blind, placebo-controlled trial in patients with completely resected stage IIIA (> 1 mm lymph node metastasis), IIIB or IIIC melanoma. A total of 1019 patients were randomized (1:1) to receive Pembrolizumab (KEYTRUDA) 200 mg every 3 weeks (n=514) or placebo (n=505), for up to one year until disease recurrence or unacceptable toxicity. Randomization was stratified by AJCC stage (IIIA vs. IIIB vs. IIIC 1-3 positive lymph nodes vs. IIIC ≥4 positive lymph nodes) and geographic region (North America, European countries, Australia, and other countries as designated). Patients must have undergone lymph node dissection and, if indicated, radiotherapy within 13 weeks prior to starting treatment. Patients with active autoimmune disease or a medical condition that required immunosuppression or mucosal or ocular melanoma were ineligible. Patients underwent imaging every 12 weeks after the first dose of Pembrolizumab (KEYTRUDA) for the first two years, then every 6 months from year 3 to 5, and then annually.
Among the 1019 patients, the baseline characteristics were: median age of 54 years (25% age 65 or older); 62% male; ECOG PS of 0 (94%) and 1 (6%). Sixteen percent had stage IIIA; 46% had stage IIIB; 18% had stage IIIC (1-3 positive lymph nodes), and 20% had stage IIIC (≥4 positive lymph nodes); 50% were BRAF V600 mutation positive and 44% were BRAF wild type; 84% had PD-L1 positive melanoma with tumor proportion score (TPS ≥1%) according to an investigational use only (IUO) assay.
The primary efficacy outcome measures were investigator-assessed RFS in the whole population and in the population with PD-L1 positive tumors. The secondary outcome measures were DMFS and OS in the whole population and in the population with PD-L1 positive tumors. OS was not formally assessed at the time of these analyses. The trial initially demonstrated a statistically significant improvement in RFS (HR 0.57; 98.4% CI 0.43, 0.74; p-Value < 0.0001) for patients randomized to the Pembrolizumab (KEYTRUDA) arm compared with placebo at its prespecified interim analysis. Updated efficacy results with a median follow-up time of 45.5 months are summarized in Table 5 and Figures 5 and 6. (See Table 5.)
Click on icon to see table/diagram/image
For patients in the whole population, the RFS rate at 42 months was 60% in the Pembrolizumab (KEYTRUDA) arm and 41% in the placebo arm (HR was 0.59 [95% CI: 0.49, 0.70]).
For patients with PD-L1 positive tumors, the RFS rate at 42 months was 61% in the Pembrolizumab (KEYTRUDA) arm and 44% in the placebo arm (HR was 0.59 (95% CI: 0.49, 0.73). Additionally, pre-defined subgroup analyses were performed in patients whose tumors were PD-L1 negative, BRAF mutation positive, or BRAF mutation negative. The RFS benefit for Pembrolizumab (KEYTRUDA) compared to placebo was observed regardless of tumor PD-L1 expression or BRAF mutation status.
The RFS HR for Pembrolizumab (KEYTRUDA) was 0.46 (95% CI: 0.27, 0.77) for patients with PD-L1 negative tumors. The RFS HR was 0.52 (95% CI: 0.40, 0.66) for patients with BRAF mutation positive tumors, and 0.67 (95% CI: 0.51, 0.88) for patients with BRAF mutation negative tumors.
For patients with PD-L1 positive tumors, the DMFS rate at 42 months was 67% in the Pembrolizumab (KEYTRUDA) arm and 52% in the placebo arm (HR was 0.61 (95% CI: 0.49, 0.76); p <0.0001). Additionally, pre-defined subgroup analyses were performed in patients whose tumors were PD-L1 negative, BRAF mutation positive, or BRAF mutation negative. The DMFS benefit for Pembrolizumab (KEYTRUDA) compared to placebo was observed regardless of tumor PD-L1 expression or BRAF mutation status. The DMFS HR for Pembrolizumab (KEYTRUDA) was 0.49 (95% CI: 0.28, 0.83) for patients with PDL1 negative tumors. The DMFS HR was 0.51 (95% CI: 0.39, 0.68) for patients with BRAF mutation positive tumors, and 0.73 (95% CI: 0.55, 0.98) for patients with BRAF mutation negative tumors. (See Figures 5 and 6.)
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Non-Small Cell Lung Carcinoma: KEYNOTE-189: Controlled trial of combination therapy in non-squamous NSCLC patients naïve to treatment: The efficacy of Pembrolizumab (KEYTRUDA) in combination with pemetrexed and platinum chemotherapy was investigated in a multicenter, randomized, active-controlled, double-blind trial, KEYNOTE-189. Key eligibility criteria were metastatic non-squamous NSCLC, no prior systemic treatment for metastatic NSCLC, and no EGFR or ALK genomic tumor aberrations. Patients with autoimmune disease that required systemic therapy within 2 years of treatment; a medical condition that required immunosuppression; or who had received more than 30 Gy of thoracic radiation within the prior 26 weeks were ineligible. Patients were randomized (2:1) to receive one of the following regimens: Pembrolizumab (KEYTRUDA) 200 mg with pemetrexed 500 mg/m
2 and investigator's choice of cisplatin 75 mg/m
2 or carboplatin AUC 5 mg/mL/min intravenously every 3 weeks for 4 cycles followed by Pembrolizumab (KEYTRUDA) 200 mg and pemetrexed 500 mg/m
2 intravenously every 3 weeks.
Placebo with pemetrexed 500 mg/m
2 and investigator's choice of cisplatin 75 mg/m
2 or carboplatin AUC 5 mg/mL/min intravenously every 3 weeks for 4 cycles followed by placebo and pemetrexed 500 mg/m
2 intravenously every 3 weeks.
Treatment with Pembrolizumab (KEYTRUDA) continued until RECIST 1.1-defined progression of disease as determined by the investigator, unacceptable toxicity, or a maximum of 24 months. Administration of Pembrolizumab (KEYTRUDA) was permitted beyond RECIST-defined disease progression by BICR or beyond discontinuation of pemetrexed if the patient was clinically stable and deriving clinical benefit as determined by the investigator. For patients who completed 24 months of therapy or had a complete response, treatment with Pembrolizumab (KEYTRUDA) could be reinitiated for disease progression and administered for up to 1 additional year. Assessment of tumor status was performed at Week 6 and Week 12, followed by every 9 weeks thereafter. Patients receiving placebo plus chemotherapy who experienced independently-verified progression of disease were offered Pembrolizumab (KEYTRUDA) as monotherapy.
Among the 616 patients in KEYNOTE-189 [410 patients in the Pembrolizumab (KEYTRUDA) combination arm and 206 in the placebo plus chemotherapy arm], baseline characteristics were: median age of 64 years (49% age 65 or older); 59% male; 94% White and 3% Asian; 43% and 56% ECOG performance status of 0 or 1 respectively; 31% with PD-L1 TPS <1%; and 18% with treated or untreated brain metastases at baseline. A total of 67 patients in the placebo plus chemotherapy arm crossed over to receive monotherapy Pembrolizumab (KEYTRUDA) at the time of disease progression and 18 additional patients received a checkpoint inhibitor as subsequent therapy.
The primary efficacy outcome measures were OS and PFS (as assessed by BICR using RECIST 1.1). Secondary efficacy outcome measures were ORR and response duration, as assessed by BICR using RECIST 1.1. The median follow-up time was 10.5 months (range: 0.2 - 20.4 months). Table 6 summarizes key efficacy measures. (See Table 6.)
Click on icon to see table/diagram/image
The final OS analysis was performed at a median duration of follow-up of 18.8 months after 421 patient events [258 for the Pembrolizumab (KEYTRUDA) combination arm and 163 for the placebo plus chemotherapy arm]. Median OS was 22.0 months (95% CI: 19.5, 24.5) for the Pembrolizumab (KEYTRUDA) combination arm and 10.6 months (95% CI: 8.7, 13.6) for the placebo plus chemotherapy arm. The OS HR was 0.56 (95% CI: 0.46, 0.69; p<0.00001). At final analysis, a PFS analysis was performed based on 534 patient events [337 for the Pembrolizumab (KEYTRUDA) combination arm and 197 for the placebo plus chemotherapy arm). The median PFS was 9.0 months (95% CI: 8.1, 10.4) for the Pembrolizumab (KEYTRUDA) combination arm and 4.9 months (95% CI: 4.7, 5.5) for the placebo plus chemotherapy arm. The PFS HR was 0.49 (95% CI: 0.41, 0.59, p<0.00001). See Figures 7 and 8.
The ORR at the final analysis was 48% for the Pembrolizumab (KEYTRUDA) combination arm and 20% for the placebo plus chemotherapy arm. The median duration of response was 12.5 months (range 1.1+, 34.9+) for the Pembrolizumab (KEYTRUDA) combination arm and 7.1 months (range 2.4, 27.8+) for the placebo plus chemotherapy arm. The percentage of patients with ongoing responses based on Kaplan-Meier estimation was 53% at 12 months or longer, in patients who received Pembrolizumab (KEYTRUDA) combination therapy, vs. 27% in patients who received placebo plus chemotherapy. (See Figures 7 and 8.)
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Patient-reported outcomes were assessed using the EORTC QLQ-C30 and EORTC QLQ-LC13. Exploratory analyses of patients receiving pembrolizumab combination therapy showed stable EORTC QLQ-C30 Global Health Status/QoL at Week 12 and Week 21 vs declines in patients receiving placebo plus chemotherapy. There was a trend toward a prolonged time to deterioration in the EORTC QLQLC13/QLQ-C30 endpoint of cough, dyspnea or chest pain observed for patients receiving pembrolizumab combination therapy.
KEYNOTE-407: Controlled trial of combination therapy in squamous NSCLC patients naïve to treatment The efficacy of Pembrolizumab (KEYTRUDA) in combination with carboplatin and either paclitaxel or nab-paclitaxel was investigated in Study KEYNOTE-407, a randomized, double-blind, multicenter, placebo-controlled study. The key eligibility criteria for this study were metastatic squamous NSCLC, regardless of tumor PD-L1 expression status, and no prior systemic treatment for metastatic disease. Patients with autoimmune disease that required systemic therapy within 2 years of treatment; a medical condition that required immunosuppression; or who had received more than 30 Gy of thoracic radiation within the prior 26 weeks were ineligible. Randomization was stratified by tumor PD-L1 expression (TPS <1% [negative] vs. TPS ≥1%), investigator's choice of paclitaxel or nab-paclitaxel, and geographic region (East Asia vs. non-East Asia). Patients were randomized (1:1) to one of the following treatment arms; all study medications were administered via intravenous infusion: Pembrolizumab (KEYTRUDA) 200 mg and carboplatin AUC 6 mg/mL/min on Day 1 of each 21-day cycle for 4 cycles, and paclitaxel 200 mg/m
2 on Day 1 of each 21-day cycle for 4 cycles or nab-paclitaxel 100 mg/m
2 on Days 1, 8 and 15 of each 21-day cycle for 4 cycles, followed by Pembrolizumab (KEYTRUDA) 200 mg every 3 weeks. Pembrolizumab (KEYTRUDA) was administered prior to chemotherapy on Day 1.
Placebo and carboplatin AUC 6 mg/mL/min on Day 1 of each 21-day cycle for 4 cycles and paclitaxel 200 mg/m
2 on Day 1 of each 21-day cycle for 4 cycles or nab-paclitaxel 100 mg/m
2 on Days 1, 8 and 15 of each 21-day cycle for 4 cycles, followed by placebo every 3 weeks.
Treatment with Pembrolizumab (KEYTRUDA) or placebo continued until RECIST 1.1-defined progression of disease as determined by blinded independent central review (BICR), unacceptable toxicity, or a maximum of 24 months. Administration of Pembrolizumab (KEYTRUDA) was permitted beyond RECIST-defined disease progression if the patient was clinically stable and deriving clinical benefit as determined by the investigator. Treatment with Pembrolizumab (KEYTRUDA) could be reinitiated for subsequent disease progression and administered for up to 1 additional year.
Patients in the placebo arm were offered Pembrolizumab (KEYTRUDA) as a monotherapy at the time of disease progression.
Assessment of tumor status was performed every 6 weeks through Week 18, every 9 weeks through Week 45 and every 12 weeks thereafter. The major efficacy outcome measures were progression-free survival and objective response rate (ORR) as assessed by BICR using RECIST 1.1 and overall survival. An additional efficacy outcome measure was duration of response as assessed by BICR using RECIST 1.1.
A total of 559 patients were randomized: 278 patients to the Pembrolizumab (KEYTRUDA) arm and 281 to the placebo arm. The study population characteristics were: median age of 65 years (range: 29 to 88); 55% age 65 or older; 81% male; 77% White; ECOG performance status of 0 (29%) and 1 (71%); and 8% with treated brain metastases at baseline. Thirty-five percent had tumor PD-L1 expression TPS <1% [negative]; 19% were from the East Asian region; and 60% received paclitaxel.
In KEYNOTE-407, there was a statistically significant improvement in OS, PFS and ORR in patients randomized to Pembrolizumab (KEYTRUDA) in combination with carboplatin and either paclitaxel or nab-paclitaxel compared with patients randomized to placebo with carboplatin and either paclitaxel or nab-paclitaxel (see Table 7).
Click on icon to see table/diagram/image
The final OS analysis was performed at a median duration of follow-up of 14.3 months after 365 patient events (168 for the Pembrolizumab (KEYTRUDA) combination arm and 197 for the placebo plus chemotherapy arm). Median OS was 17.1 months (95% CI: 14.4, 19.9) for the Pembrolizumab (KEYTRUDA) combination arm and 11.6 months (95% CI: 10.1, 13.7) for the placebo plus chemotherapy arm. The OS HR was 0.71 (95% CI: 0.58, 0.88; p=0.0006). At final analysis, a PFS analysis was performed based on 469 patient events [217 for the Pembrolizumab (KEYTRUDA) combination arm and 252 for the placebo plus chemotherapy arm]. The median PFS was 8.0 months (95% CI: 6.3, 8.4) for the Pembrolizumab (KEYTRUDA) combination arm and 5.1 months (95% CI: 4.3, 6.0) for the placebo plus chemotherapy arm. The PFS HR was 0.57 (95% CI: 0.47, 0.69, p<0.0001). (See Figures 9 and 10.)
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
KEYNOTE-042: Controlled trial of NSCLC patients naïve to treatment: The efficacy of Pembrolizumab (KEYTRUDA) was investigated in KEYNOTE-042, a multicenter, randomized, controlled trial. Key eligibility criteria were locally advanced or metastatic NSCLC, PD-L1 expression TPS of 1% or greater by an immunohistochemistry assay using the PD-L1 IHC 22C3 pharmDx Kit, and no prior systemic treatment for metastatic NSCLC. Patients with EGFR or ALK genomic tumor aberrations; autoimmune disease that required systemic therapy within 2 years of treatment; a medical condition that required immunosuppression; or who had received more than 30 Gy of thoracic radiation within the prior 26 weeks were ineligible. Patients were randomized (1:1) to receive Pembrolizumab (KEYTRUDA) 200 mg every 3 weeks (n=637) or investigator's choice platinum-containing chemotherapy (n=637; including pemetrexed+carboplatin or paclitaxel+carboplatin. Patients with non-squamous NSCLC could receive pemetrexed maintenance). Patients were treated with Pembrolizumab (KEYTRUDA) until unacceptable toxicity or disease progression. Treatment could continue beyond disease progression if the patient was clinically stable and was considered to be deriving clinical benefit by the investigator. Patients without disease progression could be treated for up to 24 months. Treatment with Pembrolizumab (KEYTRUDA) could be reinitiated for subsequent disease progression and administered for up to 1 additional year. Assessment of tumor status was performed every 9 weeks for the first 45 weeks, and every 12 weeks thereafter.
Among the 1274 patients in KEYNOTE-042, baseline characteristics were: median age 63 years (45% age 65 or older); 71% male; 64% White and 30% Asian: 19% Hispanic or Latino; and 31% and 69%with an ECOG performance status 0 and 1, respectively. Disease characteristics were squamous (39%) and non-squamous (61%); M0 (13%), M1 (87%); and treated brain metastases (6%). Forty-seven percent of patients had TPS ≥50%, and 53% had TPS 1 to 49%.
The primary efficacy outcome measure was OS. Secondary efficacy outcome measures were PFS and ORR as assessed by blinded independent central review (BICR) using RECIST 1.1. Table 8 summarizes key efficacy measures for the entire ITT population (TPS ≥ 1%). (See Table 8 and Figure 11.)
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
KEYNOTE-024: Controlled trial of NSCLC patients naïve to treatment: The efficacy of Pembrolizumab (KEYTRUDA) in previously untreated patients with NSCLC was also investigated in KEYNOTE-024, a multicenter, randomized, controlled trial. The study design was similar to that of KEYNOTE-042, except that only patients with metastatic NSCLC whose tumors expressed PD-L1 with TPS of 50% or greater by an immunohistochemistry assay using the PD-L1 IHC 22C3 pharmDx Kit were eligible. Patients were randomized (1:1) to receive Pembrolizumab (KEYTRUDA) 200 mg every 3 weeks (n=154) or investigator's choice platinum-containing chemotherapy (n=151); including pemetrexed+carboplatin, pemetrexed+cisplatin, gemcitabine+cisplatin, gemcitabine+carboplatin, or paclitaxel+carboplatin. Patients with non-squamous NSCLC could receive pemetrexed maintenance). Patients on chemotherapy who experienced independently-verified progression of disease were able to crossover and receive Pembrolizumab (KEYTRUDA). Assessment of tumor status was performed every 9 weeks.
Among the 305 patients in KEYNOTE-024, baseline characteristics were: median age 65 years (54% age 65 or older); 61% male; 82% White and 15% Asian; and 35% and 65% with an ECOG performance status 0 and 1, respectively. Disease characteristics were squamous (18%) and non-squamous (82%); M1 (99%); and brain metastases (9%).
The primary efficacy outcome measure was PFS as assessed by blinded independent central review (BICR) using RECIST 1.1. Secondary efficacy outcome measures were OS and ORR (as assessed by BICR using RECIST 1.1). Table 9 summarizes key efficacy measures for the entire ITT population. (See Table 9.)
Click on icon to see table/diagram/image
The final OS analysis was performed at a median follow-up of 25 months after 169 patient events [73 for Pembrolizumab (KEYTRUDA) and 96 for chemotherapy]. Median OS was 30.0 months (95% CI: 18.3, NA) for Pembrolizumab (KEYTRUDA) and 14.2 months (95% CI: 9.8, 19.0) for chemotherapy. The OS HR was 0.63 (95% CI: 0.47, 0.86; p=0.002) (see Figure 13). (See Figures 12 and 13.)
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
The improved benefit as assessed by PFS, OS, ORR, and response duration for Pembrolizumab (KEYTRUDA) as compared to chemotherapy in the population studied was associated with improvements in health-related quality of life (HRQoL). The change from baseline to Week 15 showed a meaningful improvement in the European Organization for Research and Treatment of Cancer Quality of Life Questionnaire (EORTC QLQ) C30 global health status/QoL score for patients receiving Pembrolizumab (KEYTRUDA) compared to chemotherapy (difference in LS means = 7.82; 95% CI: 2.85, 12.79; two-sided p=0.002). The time to deterioration in the EORTC QLQ-LC13 composite endpoint of cough, dyspnea, and chest pain was prolonged for patients receiving Pembrolizumab (KEYTRUDA) compared to chemotherapy (HR = 0.66; 95% CI: 0.44, 0.97; two-sided p=0.029), where deterioration is defined as a confirmed 10-point or greater score decrease from baseline in any one of these three symptoms.
KEYNOTE-010: Controlled trial of NSCLC patients previously treated with chemotherapy: The efficacy of Pembrolizumab (KEYTRUDA) was investigated in KEYNOTE-010, a multicenter, randomized, controlled trial. Key eligibility criteria were advanced NSCLC that had progressed following platinum-containing chemotherapy, and if appropriate, targeted therapy for ALK or EGFR mutations, and PD-L1 expression TPS of 1% or greater by a clinical trial assay version of the PD-L1 IHC 22C3 pharmDx kit. Patients with autoimmune disease; a medical condition that required immunosuppression; or who had received more than 30 Gy of thoracic radiation within the prior 26 weeks were ineligible. Patients were randomized (1:1:1) to receive 2 mg/kg (n=344) or 10 mg/kg (n=346) of Pembrolizumab (KEYTRUDA) every 3 weeks or 75 mg/m
2 of docetaxel every 3 weeks (n=343). Patients were treated with Pembrolizumab (KEYTRUDA) until disease progression or unacceptable toxicity. Assessment of tumor status was performed every 9 weeks.
Among the 1033 patients in KEYNOTE-010, baseline characteristics were: median age 63 years (42% age 65 or older); 61% male; 72% White and 21% Asian; and 34% and 66% with an ECOG performance status 0 and 1, respectively. Disease characteristics were squamous (21%) and non-squamous (70%); M1 (91%); brain metastases (15%); and the incidence of genomic aberrations was EGFR (8%) or ALK (1%). Prior therapy included platinum-doublet regimen (100%); patients received one (69%), or two or more (29%) prior therapies.
The primary efficacy outcome measures were OS and PFS as assessed by an independent review committee using RECIST 1.1. Secondary efficacy outcome measures were ORR and response duration. Table 10 summarizes key efficacy measures for the entire ITT population (TPS ≥ 1%) and for the subgroup of patients with TPS ≥ 50%. Kaplan-Meier curves for OS (TPS ≥ 1% and TPS ≥ 50%) are shown in Figures 14 and 15. (See Table 10, Figures 14 and 15.)
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Efficacy results were similar for the 2 mg/kg and 10 mg/kg Pembrolizumab (KEYTRUDA) arms. Efficacy results for OS were consistent regardless of the age of tumor specimen (new versus archival).
KEYNOTE-001: Open-label study in NSCLC patients previously treated with chemotherapy: The efficacy of Pembrolizumab (KEYTRUDA) was also investigated in a multicenter, open-label, randomized, dose-comparative cohort of KEYNOTE-001. Patients had advanced NSCLC that was PDL1 positive, with progression of disease following treatment with platinum-containing chemotherapy. Patients with EGFR or ALK genomic tumor aberrations had disease progression on approved therapy for these aberrations prior to receiving Pembrolizumab (KEYTRUDA). The trial excluded patients with autoimmune disease; a medical condition that required immunosuppression; or who had received more than 30 Gy of thoracic radiation within the prior 26 weeks. Patients were randomized to receive 10 mg/kg of Pembrolizumab (KEYTRUDA) every 2 (n=69) or 3 (n=87) weeks until disease progression or unacceptable toxicity. Assessment of tumor status was performed every 9 weeks. The major efficacy outcome measures were ORR (according to RECIST 1.1 as assessed by blinded independent central review) and duration of response.
The prevalence of patients with a PD-L1 expression TPS greater than or equal to 50% among screened patients with NSCLC as ascertained retrospectively by the companion diagnostic PD-L1 IHC 22C3 pharmDx kit was 26%. Among the randomized patients with tumor samples evaluable for PD-L1 expression, 61 had TPS greater than or equal to 50%. The baseline characteristics for this population included: median age 60 years (34% age 65 or older); 61% male; 79% White; and 34% and 64% with an ECOG performance status 0 and 1, respectively. Disease characteristics were squamous and non-squamous (21% and 75%, respectively); M1 (98%); brain metastases (11%); and one (25%), two (31%), or three or more (44%) prior therapies. The mutation status among patients was EGFR (10%), ALK (0%), or Kras (16%).
Efficacy results for NSCLC patients treated with 10 mg/kg every 2 or 3 weeks in KEYNOTE-001 are summarized in Table 11. (See Table 11.)
Click on icon to see table/diagram/image
Similar ORR results were observed in another group of patients (n=25) with TPS greater than or equal to 50% receiving Pembrolizumab (KEYTRUDA) at a dose of 2 mg/kg every 3 weeks in KEYNOTE-001.
Small Cell Lung Cancer: KEYNOTE-028 and KEYNOTE-158: Open-label studies in patients with SCLC, who have received prior therapy: The efficacy of Pembrolizumab (KEYTRUDA) was investigated in 82 patients with SCLC who have received two or more prior lines of therapy enrolled in one of two multicenter, multi-cohort, nonrandomized, open-label trials, Study KEYNOTE-028, Cohort C1, or Study KEYNOTE-158, Cohort G. The trials excluded patients with autoimmune disease or a medical condition that required immunosuppression.
Patients received Pembrolizumab (KEYTRUDA) 10 mg/kg every 2 weeks (n=19) or 200 mg every 3 weeks (n=63) until unacceptable toxicity or documented disease progression. Clinically stable patients with initial evidence of disease progression were permitted to remain on treatment until disease progression was confirmed. Patients without disease progression could be treated for up to 24 months.
Assessment of tumor status in KEYNOTE-028 was performed every 8 weeks for the first 6 months, and in KEYNOTE-158 every 9 weeks for the first 12 months, and every 12 weeks thereafter. The major efficacy outcome measures were ORR and duration of response, as assessed by blinded independent central review (BICR) using RECIST 1.1.
The baseline characteristics of these 82 patients were: median age of 63 years (range: 24 to 84 years); 40% age 65 or older; 63% male; 62% White, 26% Asian, 2% Black; ECOG performance status of 0 (30%) or 1 (68%); 6% had M0 disease and 94% had M1 disease; 16% had a history of brain metastases. Sixty-three percent received two prior lines of therapy and 37% received three or more lines of therapy; 80% received prior radiation therapy.
The median follow-up time for 82 patients treated with Pembrolizumab (KEYTRUDA) was 7.7 months. Efficacy results are summarized in Table 12. (See Table 12.)
Click on icon to see table/diagram/image
Head and Neck Cancer: KEYNOTE-048: Controlled trial of first-line monotherapy or combination therapy in HNSCC: The efficacy of Pembrolizumab (KEYTRUDA) was investigated in Study KEYNOTE-048, a multicenter, randomized, open-label, active-controlled study in patients with metastatic or recurrent HNSCC who had not previously received systemic therapy for recurrent or metastatic disease and who were considered incurable by local therapies. Patients with active autoimmune disease that required systemic therapy within two years of treatment or a medical condition that required immunosuppression were ineligible for the study. Randomization was stratified by tumor PD-L1 expression (TPS≥50% or <50%) based on the PD-L1 IHC 22C3 pharmDx kit, HPV status (positive or negative), and ECOG PS (0 vs. 1). Patients were randomized 1:1:1 to one of the following treatment arms: Pembrolizumab (KEYTRUDA) 200 mg every 3 weeks; Pembrolizumab (KEYTRUDA) 200 mg every 3 weeks, carboplatin AUC 5 mg/ml/min every 3 weeks or cisplatin 100 mg/m
2 every 3 weeks, and 5-FU 1000 mg/m
2/d 4 days continuous every 3 weeks (maximum of 6 cycles of platinum and 5-FU); Cetuximab 400 mg/m
2 load then 250 mg/m
2 once weekly, carboplatin AUC 5 mg/ml/min every 3 weeks or cisplatin 100 mg/m
2 every 3 weeks, and 5-FU 1000 mg/m
2/d 4 days continuous every 3 weeks (maximum of 6 cycles of platinum and 5-FU).
Treatment with Pembrolizumab (KEYTRUDA) continued until RECIST 1.1-defined progression of disease as determined by the investigator, unacceptable toxicity, or a maximum of 24 months. Administration of Pembrolizumab (KEYTRUDA) was permitted beyond RECIST-defined disease progression if the patient was clinically stable and considered to be deriving clinical benefit by the investigator. Assessment of tumor status was performed at Week 9 and then every 6 weeks for the first year, followed by every 9 weeks through 24 months.
A total of 882 patients were randomized; 301 patients to the Pembrolizumab (KEYTRUDA) monotherapy arm, 281 patients to the Pembrolizumab (KEYTRUDA) plus chemotherapy arm, and 300 patients to the standard treatment arm. The study population characteristics were: median age of 61 years (range: 20 to 94); 36% age 65 or older; 83% male; 73% White and 20% Asian; 61% ECOG PS of 1; and 79% were former/current smokers. Disease characteristics were: 22% HPV positive, 85%, 43%, and 23% had PD-L1 expression defined as CPS ≥1, CPS ≥20, and TPS ≥50%, respectively, and 95% had Stage IV disease (Stage IVa 19%, Stage IVb 6%, and Stage IVc 70%).
The primary efficacy outcome measures were OS and PFS (assessed by BICR according to RECIST 1.1). ORR, as assessed by BICR according to RECIST 1.1, was a secondary outcome measure. The trial demonstrated a statistically significant improvement in OS for patients randomized to Pembrolizumab (KEYTRUDA) in combination with chemotherapy compared to standard treatment. OS for patients randomized to Pembrolizumab (KEYTRUDA) monotherapy was non-inferior compared to standard treatment. Tables 13 and 14 and Figures 16 and 17 describe key efficacy results for Pembrolizumab (KEYTRUDA) in KEYNOTE-048. (See Table 13.)
Click on icon to see table/diagram/image
In KEYNOTE-048, OS HRs for patients randomized to Pembrolizumab (KEYTRUDA) in combination with chemotherapy, compared with cetuximab in combination with chemotherapy, were similar for all populations regardless of PD-L1 expression in a pre-specified interim analysis: ITT (HR 0.77, 95% CI: 0.63, 0.93), CPS ≥1 (HR 0.71, 95% CI: 0.57, 0.88), CPS ≥20 (HR 0.69, 95% CI: 0.51, 0.94). The OS HRs at final analysis with a median follow-up of 11.4 months were similar to those obtained at the pre-specified interim analysis and in addition, demonstrated a statistically significant improvement in OS for the subgroup of patients with PD-L1 CPS ≥1 and CPS ≥20: ITT (0.72, 95% CI: 0.60, 0.87), CPS ≥1 (0.65, 95% CI: 0.53, 0.80), CPS ≥20 (0.60, 95% CI: 0.45, 0.82). (See Figure 16, Table 14 and Figure 17.)
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Additional OS analyses based on PD-L1 expression (CPS ≥1 and CPS ≥20) were performed in KEYNOTE048. The trial demonstrated a statistically significant improvement in OS for patients randomized to Pembrolizumab (KEYTRUDA) monotherapy compared to standard treatment for PD-L1 expression CPS ≥1 and CPS ≥20. OS for patients who had PD-L1 CPS ≥1 or CPS ≥20 for Pembrolizumab (KEYTRUDA) monotherapy compared to standard treatment is summarized in Table 15. (See Table 15.)
Click on icon to see table/diagram/image
The final OS analysis was performed for patients with CPS ≥1 with a median follow-up of 11.4 months from the pre-specified interim analysis. Median OS was 12.3 months (95% CI: 10.8, 14.3) for Pembrolizumab (KEYTRUDA) as a single agent and 10.3 months (95% CI: 9.0, 11.5) for cetuximab in combination with chemotherapy, with an HR of 0.74 (95% CI: 0.61, 0.90).
The final OS analysis was performed for patients with CPS ≥20 with a median follow-up of 12.2 months from the pre-specified interim analysis. Median OS was 14.8 months (95% CI: 11.5, 20.6) for Pembrolizumab (KEYTRUDA) as a single agent and 10.7 months (95% CI: 8.8, 12.8) for cetuximab in combination with chemotherapy, with an HR of 0.58 (95% CI: 0.44, 0.78).
In an exploratory subgroup analysis for patients with CPS 1-19 HNSCC, the median OS was 10.8 months (95% CI: 9.0, 12.6) for Pembrolizumab (KEYTRUDA) as a single agent and 10.1 months (95% CI: 8.7, 12.1) for cetuximab in combination with chemotherapy, with an HR of 0.90 (95% CI: 0.68, 1.18). The final OS analysis was performed for patients with CPS 1-19 with a median follow-up of 10.3 months. At the final analysis, the median OS was 10.8 months (95% CI: 9.0, 12.6) for Pembrolizumab (KEYTRUDA) as a single agent and 10.1 months (95% CI: 8.7, 12.1) for cetuximab in combination with chemotherapy, with an HR of 0.86 (95% CI: 0.66, 1.12).
KEYNOTE-040: Controlled trial in HNSCC patients previously treated with platinum-containing chemotherapy: The efficacy of Pembrolizumab (KEYTRUDA) was investigated in KEYNOTE-040, a multicenter, open-label, randomized, active-controlled study for the treatment of recurrent or metastatic HNSCC in patients with disease progression who received prior platinum-containing chemotherapy. The study excluded patients with active autoimmune disease that required systemic therapy within 2 years of treatment, a medical condition that required immunosuppression, or who were previously treated with 3 or more systemic regimens for recurrent and/or metastatic HNSCC.
Patients were stratified by PD-L1 expression, HPV status and ECOG performance status and then randomized (1:1) to receive either Pembrolizumab (KEYTRUDA) 200 mg every 3 weeks (n=247) or one of three standard treatments (n=248): methotrexate 40 mg/m
2 once weekly (n=64), docetaxel 75 mg/m
2 once every 3 weeks (n=99), or cetuximab 400 mg/m
2 loading dose and then 250 mg/m
2 once weekly (n=71). Patients were treated with Pembrolizumab (KEYTRUDA) for up to 24 months or until unacceptable toxicity or disease progression. Treatment could continue beyond progression if the patient was clinically stable and was considered to be deriving clinical benefit by the investigator. Assessment of tumor status was performed at 9 weeks, then every 6 weeks through week 52, followed by every 9 weeks through 24 months.
Among the 495 randomized patients in KEYNOTE-040, the baseline characteristics included: median age 60 years (33% age 65 or older); 83% male; 84% White, 6% Asian, and 2% Black; and 28% and 72% with an ECOG performance status 0 or 1, respectively. Disease characteristics were: HPV positive (24%) and PD-L1 expression defined as CPS ≥1 (78%) and TPS ≥50% (26%). Seventy-one percent (71%) of patients had M1 disease and the majority had Stage IV disease (Stage IV 33%, Stage IVa 11%, Stage IVb 5%, and Stage IVc 45%). Fifteen percent (15%) had disease progression following platinum-containing neoadjuvant or adjuvant chemotherapy, and 84% had received 1-2 prior systemic regimens for metastatic disease.
The primary efficacy outcome was OS. Secondary efficacy outcome measures were PFS, ORR, and duration of response (as assessed by BICR using RECIST 1.1) and OS (PD-L1 CPS ≥1). Efficacy measures for KEYNOTE-040 are summarized in Table 16, and the Kaplan-Meier curve for OS is shown in Figure 18. (See Table 16 and Figure 18.)
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
KEYNOTE-012: Open-label study in HNSCC patients previously treated with chemotherapy: The efficacy of Pembrolizumab (KEYTRUDA) was investigated in 192 patients with recurrent and/or metastatic HNSCC, regardless of tumor human papilloma virus (HPV) status (33% positive), enrolled in a multicenter, non-randomized, open-label multi-cohort study (KEYNOTE-012). One cohort (n=132) was included regardless of PD-L1 tumor status. Efficacy is reported for a subgroup of 110 patients with recurrent and/or metastatic HNSCC that progressed on or after treatment with platinum-containing chemotherapy and cetuximab, and for a subgroup of 64 patients with recurrent and/or metastatic HNSCC that progressed on or after treatment with platinum-containing chemotherapy without prior cetuximab. Patients with active autoimmune disease or a medical condition that required immunosuppression were ineligible.
Patients received Pembrolizumab (KEYTRUDA) 10 mg/kg every 2 weeks (n=53), or 200 mg every 3 weeks (n=121) until disease progression or unacceptable toxicity. Assessment of tumor status was performed every 8 weeks. The major efficacy outcome measures were ORR according to RECIST 1.1, as assessed by blinded independent central review, and duration of response.
Among the 64 patients with disease progression after platinum-containing chemotherapy without prior cetuximab, the baseline characteristics were median age 60 years (28% age 65 or older); 77% male; 75% White, 20% Asian, and 3% Black; 88% had M1 stage disease; and 33% and 67% had an ECOG performance status 0 and 1, respectively. Thirty-six percent of patients had two or more lines of therapy in the recurrent and/or metastatic setting.
Among the 110 patients with disease progression after platinum-containing chemotherapy and cetuximab, the baseline characteristics were median age 60 years (34% age 65 or older); 85% male; 75% White, 14% Asian, and 7% Black; 87% had M1 stage disease; and 27% and 73% had an ECOG performance status 0 and 1, respectively. Eighty percent of patients had two or more lines of therapy in the recurrent and/or metastatic setting.
Efficacy results are summarized in Table 17. (See Table 17.)
Click on icon to see table/diagram/image
There were objective responses in patients regardless of HPV tumor status.
Classical Hodgkin Lymphoma: KEYNOTE-204: Controlled study in patients with relapsed or refractory classical Hodgkin Lymphoma (cHL): KEYNOTE-204 was a randomized, open-label, active-controlled trial conducted in 304 patients with relapsed or refractory cHL. Patients with active, non-infectious pneumonitis, an allogeneic HSCT within the past 5 years (or >5 years but with symptoms of GVHD), active autoimmune disease, a medical condition that required immunosuppression, or an active infection requiring systemic therapy were ineligible for the trial. Randomization was stratified by prior auto-SCT (yes vs. no) and disease status after frontline therapy (primary refractory vs. relapse less than 12 months after completion vs. relapse 12 months or more after completion). Patients were randomized (1:1) to one of the following treatment arms: Pembrolizumab (KEYTRUDA) 200 mg intravenously every 3 weeks; Brentuximab vedotin (BV) 1.8 mg/kg intravenously every 3 weeks.
Patients received Pembrolizumab (KEYTRUDA) 200 mg intravenously every 3 weeks until unacceptable toxicity or documented disease progression. Disease assessment was performed every 12 weeks. The major efficacy outcome measures were PFS and ORR as assessed by BICR according to the 2007 revised International Working Group (IWG) criteria.
Among KEYNOTE-204 patients, the baseline characteristics were median age 35 years (16% age 65 or older); 57% male; 77% White; and 61% and 38% had an ECOG performance status 0 and 1, respectively. The median number of prior lines of therapy administered for the treatment of cHL was 2 (range 1 to 11). Forty-two percent were refractory to the last prior therapy and 29% had primary refractory disease. Thirty-seven percent had undergone prior auto-HSCT, 5% had received prior BV, and 39% had prior radiation therapy.
The median follow-up time for 151 patients treated with Pembrolizumab (KEYTRUDA) was 24.9 months (range: 1.8 to 42.0 months). Efficacy results are summarized in Table 18. (See Table 18 and Figure 19.)
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Patient-reported outcomes (PROs) were assessed using EORTC QLQ-C30. A prolonged time to deterioration in EORTC QLQ C30 global health status/QoL was observed for patients treated with pembrolizumab compared to BV (HR 0.40; 95% CI: 0.22-0.74). Over 24 weeks of follow-up, patients treated with pembrolizumab had an improvement in global health status/QoL compared to BV which showed a decline (difference in Least Square (LS) means = 8.60; 95% CI: 3.89, 13.31; nominal two-sided p=0.0004). These results should be interpreted in the context of the open-label study design and therefore taken cautiously.
KEYNOTE-013 and KEYNOTE-087: Open-label studies in patients with refractory classical Hodgkin Lymphoma, or those who have relapsed after greater than or equal to 3 prior lines of therapy: The efficacy of Pembrolizumab (KEYTRUDA) was investigated in 241 patients with refractory classical Hodgkin Lymphoma, or who have relapsed after 3 or more prior lines of therapy, enrolled in two multicenter, non-randomized, open-label studies (KEYNOTE-013 and KEYNOTE-087). Both studies included patients regardless of PD-L1 expression. Patients with active, non-infectious pneumonitis, an allogeneic hematopoietic stem cell transplant within the past 5 years (or greater than 5 years but with GVHD), active autoimmune disease or a medical condition that required immunosuppression were ineligible for either trial. Patients received Pembrolizumab (KEYTRUDA) 10 mg/kg every 2 weeks (n=31) or 200 mg every 3 weeks (n=210) until unacceptable toxicity or documented disease progression. Response was assessed using the revised lymphoma criteria by PET CT scans, with the first planned post-baseline assessment at Week 12. The major efficacy outcome measures (ORR, CRR, and duration of response) were assessed by blinded independent central review according to the 2007 revised International Working Group (IWG) criteria. Secondary efficacy outcome measures were PFS and OS.
Among KEYNOTE-013 patients, the baseline characteristics were median age 32 years (6% age 65 or older), 58% male, 94% White; and 45% and 55% had an ECOG performance status 0 and 1, respectively. The median number of prior lines of therapy administered for the treatment of cHL was 5 (range 2 to 15). Eighty-seven percent were refractory to at least one prior therapy, including 39% who were refractory to first-line therapy. Seventy-four percent of patients had received Auto-SCT, 26% were transplant ineligible; and 42% of patients had prior radiation therapy.
Among KEYNOTE-087 patients, the baseline characteristics were median age 35 years (9% age 65 or older); 54% male; 88% White; and 49% and 51% had an ECOG performance status 0 and 1, respectively. The median number of prior lines of therapy administered for the treatment of cHL was 4 (range 1 to 12). Eighty-one percent were refractory to at least one prior therapy, including 34% who were refractory to first-line therapy. Sixty-one percent of patients had received Auto-SCT, 38% were transplant ineligible; 17% had no prior brentuximab vedotin use; and 37% of patients had prior radiation therapy.
Efficacy results are summarized in Table 19. (See Table 19.)
Click on icon to see table/diagram/image
The improved benefit as assessed by ORR, CRR, and response duration in the KEYNOTE-087 population was accompanied by overall improvements in health-related quality of life (HRQoL) as assessed using the European Organization for Research and Treatment of Cancer Quality of Life Questionnaire Core 30 (EORTC QLQ-C30) and the European Quality of Life Five Dimensions Questionnaire (EQ-5D). Relative to subjects with stable disease or progressive disease, subjects with a complete or partial response had the largest improvement and the highest proportion with a 10 point or greater increase in their EORTC QLQ-C30 global health status/QoL score, as well as, had the largest improvement in their EQ-5D utility and VAS scores from baseline to Week 12.
Urothelial Carcinoma: KEYNOTE-052: Open-label trial in urothelial carcinoma patients ineligible for cisplatin-containing chemotherapy: The efficacy of Pembrolizumab (KEYTRUDA) was investigated in KEYNOTE-052, a multicenter, open-label trial of patients with locally advanced or metastatic urothelial carcinoma who were not eligible for cisplatin-containing chemotherapy. The trial excluded patients with autoimmune disease or a medical condition that required immunosuppression.
Patients received Pembrolizumab (KEYTRUDA) 200 mg every 3 weeks until unacceptable toxicity or disease progression. Clinically stable patients with initial evidence of disease progression were permitted to remain on treatment until disease progression was confirmed. Patients without disease progression were treated for up to 24 months. Treatment with pembrolizumab could be reinitiated for subsequent disease progression and administered for up to 1 additional year. Assessment of tumor status was performed at 9 weeks after the first dose, then every 6 weeks through the first year, followed by every 12 weeks thereafter. The major efficacy outcome measures were ORR according to RECIST 1.1 and duration of response. Efficacy is reported for patients who had the opportunity for at least 2 postbaseline scans representing at least 4 months of follow-up.
Among 370 patients with urothelial carcinoma who were not eligible for cisplatin-containing chemotherapy, baseline characteristics were: median age 74 years (82% age 65 or older); 77% male; and 89% White and 7% Asian. Eighty-eight percent had M1 disease, 12% had M0 disease. Eighty-five percent of patients had visceral metastases, including 21% with liver metastases. Reasons for cisplatin ineligibility included: baseline creatinine clearance of <60 mL/min (50%), ECOG performance status of 2 (32%), ECOG performance status of 2 and baseline creatinine clearance of <60 mL/min (9%), and other (Class III heart failure, Grade 2 or greater peripheral neuropathy, and Grade 2 or greater hearing loss; 9%). Ninety percent of patients were treatment naïve, and 10% received prior adjuvant or neoadjuvant platinum-based chemotherapy. Eighty-one percent had a primary tumor in the lower tract, and 19% of patients had a primary tumor in the upper tract.
Among the 370 patients, 30% (n = 110) had tumors that expressed PD-L1 with a combined positive score (CPS) of greater than or equal to 10. PD-L1 status was determined using the PD-L1 IHC 22C3 pharmDx Kit. The baseline characteristics of these 110 patients were: median age 73 years, 68% male, and 87% White. Eighty-two percent had M1 disease, and 18% had M0 disease. Eighty-one percent had a primary tumor in the lower tract, and 18% of patients had a primary tumor in the upper tract. Seventy-six percent of patients had visceral metastases, including 11% with liver metastases. Reasons for cisplatin ineligibility included: 45% with baseline creatinine clearance of <60 mL/min, 37% with ECOG performance status of 2, 10% with ECOG 2 and baseline creatinine clearance of <60 mL/min, and 8% with other reasons (Class III heart failure, Grade 2 or greater peripheral neuropathy, and Grade 2 or greater hearing loss). Ninety percent of patients were treatment naïve, and 10% received prior adjuvant or neoadjuvant platinum-based chemotherapy.
At a pre-specified interim analysis, the median follow-up time for 370 patients treated with Pembrolizumab (KEYTRUDA) was 11.5 months. Efficacy results are summarized in Table 20. The data presented for subjects with PD-L1 CPS ≥10 are based on a subgroup analysis in a single-arm trial. A randomized, controlled confirmatory trial is ongoing. (See Table 20.)
Click on icon to see table/diagram/image
The final ORR analysis was performed 9.9 months after the interim analysis with 106 ORR events for all patients [median follow-up of 11.4 months (range: 0.1, 41.2 months)]. ORR was 29% (95% CI: 24, 34) and 47% (95% CI: 38, 57), respectively for all subjects and subjects with CPS ≥10. The complete and partial response rates were 9% and 20%, respectively in all subjects and 20% and 27%, respectively in subjects with CPS ≥10. At the final analysis among the responding patients, the median response duration was 30.1 months (range 1.4+ to 35.9+ months) in all subjects (n=106) and not reached (range 1.4+ to 35.4+ months) in subjects with CPS ≥10 (n=52). Responses of 6 months or longer (based on Kaplan-Meier estimation) were 81% and 82%, respectively for all subjects and subjects with CPS ≥10.
KEYNOTE-045: Controlled trial in urothelial carcinoma patients previously treated with platinum-containing chemotherapy: The efficacy of Pembrolizumab (KEYTRUDA) was evaluated in KEYNOTE-045, a multicenter, randomized (1:1), active-controlled trial in patients with locally advanced or metastatic urothelial carcinoma with disease progression on or after platinum-containing chemotherapy. The trial excluded patients with autoimmune disease or a medical condition that required immunosuppression.
Patients were randomized to receive either Pembrolizumab (KEYTRUDA) 200 mg every 3 weeks (n=270) or investigator's choice of any of the following chemotherapy regimens all given intravenously every 3 weeks (n=272): paclitaxel 175 mg/m
2 (n=84), docetaxel 75 mg/m
2 (n=84), or vinflunine 320 mg/m
2 (n=87). Patients received Pembrolizumab (KEYTRUDA) until unacceptable toxicity or disease progression. Clinically stable patients with initial evidence of disease progression were permitted to remain on treatment until disease progression was confirmed. Patients without disease progression were treated for up to 24 months. Treatment with pembrolizumab could be reinitiated for subsequent disease progression and administered for up to 1 additional year. Assessment of tumor status was performed at 9 weeks after randomization, then every 6 weeks through the first year, followed by every 12 weeks thereafter. The major efficacy outcomes were OS and PFS as assessed by BICR per RECIST v1.1. Additional efficacy outcome measures were ORR as assessed by BICR per RECIST v1.1 and duration of response.
Among the 542 randomized patients, the study population characteristics were: median age 66 years (range: 26 to 88), 58% age 65 or older; 74% male; 72% White and 23% Asian; 57% ECOG performance status of 1 or greater; and 96% M1 disease and 4% M0 disease. Eighty-seven percent of patients had visceral metastases, including 34% with liver metastases. Eighty-six percent had a primary tumor in the lower tract and 14% had a primary tumor in the upper tract. Fifteen percent of patients had disease progression following prior platinum-containing neoadjuvant or adjuvant chemotherapy as the most recent line of therapy. Twenty-one percent had received 2 or more prior systemic regimens in the metastatic setting. Seventy-six percent of patients received prior cisplatin, 23% had prior carboplatin, and 1% were treated with other platinum-based regimens.
At a pre-specified interim analysis, the median follow-up time for 270 patients treated with Pembrolizumab (KEYTRUDA) was 10.3 months. The study demonstrated statistically significant improvements in OS and ORR for patients randomized to Pembrolizumab (KEYTRUDA) as compared to chemotherapy (see Table 21). There was no statistically significant difference between Pembrolizumab (KEYTRUDA) and chemotherapy with respect to PFS. Efficacy results are summarized in Table 21. (See Table 21.)
Click on icon to see table/diagram/image
The final OS analysis was performed 13.6 months after the interim analysis with 419 patient events [200 for Pembrolizumab (KEYTRUDA) and 219 for chemotherapy]. Median OS was 10.1 months (95% CI: 8.0, 12.3) for Pembrolizumab (KEYTRUDA) and 7.3 months (95% CI: 6.1, 8.1) for chemotherapy. The OS HR was 0.70 (95% CI: 0.57, 0.85; p<0.001). See Figure 20 In the final analysis there was no statistically significant difference between Pembrolizumab (KEYTRUDA) and chemotherapy with respect to PFS.
At the final analysis, among the 57 responding patients who received Pembrolizumab (KEYTRUDA) vs. 30 responding patients who received chemotherapy, the median response duration was not reached (range 1.6+ to 30.0+ months) in patients who received Pembrolizumab (KEYTRUDA), vs. 4.4 months (range 1.4+ to 29.9+ months) in patients who received chemotherapy. In patients who received Pembrolizumab (KEYTRUDA), 84% had responses of 6 months or longer and 68% had responses of 12 months or longer (based on Kaplan-Meier estimation) vs. 47% who had responses of 6 months or longer and 35% who had responses of 12 months or longer (based on Kaplan-Meier estimation) in patients who received chemotherapy. The complete and partial response rates were 9% and 12%, respectively in patients who received Pembrolizumab (KEYTRUDA) vs. 3% and 8%, respectively in patients who received chemotherapy. (See Figure 20.)
Click on icon to see table/diagram/image
Patient-reported outcomes (PROs) were assessed using the EORTC QLQ-C30. A prolonged time to deterioration in the EORTC QLQ-C30 global health status/QoL score was observed for patients treated with pembrolizumab compared to investigator's choice chemotherapy (HR 0.70; 95% CI 0.55-0.90). Over 15 weeks of follow-up, patients treated with pembrolizumab had stable global health status/QoL scores, while those treated with investigator's choice chemotherapy had a decline in global health status/QoL scores. These results should be interpreted in the context of the open-label study design and therefore taken cautiously.
KEYNOTE-057: BCG-unresponsive High-Risk Non-Muscle Invasive Bladder Cancer: The efficacy of Pembrolizumab (KEYTRUDA) was investigated in KEYNOTE-057, a multicenter, open-label, single-arm trial in 96 patients with Bacillus Calmette-Guerin (BCG)-unresponsive, high-risk, non-muscle invasive bladder cancer (NMIBC) with carcinoma in-situ (CIS) with or without papillary tumors who are ineligible for or have elected not to undergo cystectomy. BCG-unresponsive high-risk NMIBC is defined as persistent disease despite adequate BCG therapy, disease recurrence after an initial tumor-free state following adequate BCG therapy, or T1 disease following a single induction course of BCG. Prior to treatment, all patients had received adequate BCG therapy, had undergone recent cystoscopic procedure(s) and transurethral resection of bladder tumor (TURBT) to remove all resectable disease (Ta and T1 components) and assure the absence of muscle invasive disease. Residual CIS (Tis components) not amenable to complete resection was acceptable. The trial excluded patients with muscle invasive (i.e., T2, T3, T4) locally advanced non-resectable or metastatic urothelial carcinoma, concurrent extra-vesical (i.e., urethra, ureter or renal pelvis) non-muscle invasive transitional cell carcinoma of the urothelium, autoimmune disease or a medical condition that required immunosuppression.
Patients received Pembrolizumab (KEYTRUDA) 200 mg every 3 weeks until unacceptable toxicity, persistent or recurrent high-risk NMIBC, or progressive disease. Assessment of tumor status was performed every 12 weeks, and patients without disease progression could be treated for up to 24 months. The major efficacy outcome measures were complete response (as defined by negative results for cystoscopy [with TURBT/biopsies as applicable], urine cytology, and computed tomography urography [CTU] imaging) and duration of response.
The study population characteristics were: median age 73 years (69% age 65 or older); 84% male; 67% White; and 73% and 27% with an ECOG performance status of 0 or 1, respectively. Tumor pattern at study entry was CIS with T1 (13%), CIS with high grade TA (25%), and CIS (63%). Baseline high-risk NMIBC disease status was 27% persistent and 73% recurrent. The median number of prior instillations of BCG was 12.
The median follow-up time was 28.0 months (range: 4.6 to 40.5 months). Efficacy results are summarized in Table 22. (See Table 22.)
Click on icon to see table/diagram/image
At the time of analysis, among the 96 patients there were no occurrences of progression to muscle-invasive disease (T2) or metastatic bladder cancer while on Pembrolizumab (KEYTRUDA).
Patients who had a complete response to pembrolizumab in the KEYNOTE-057 maintained their health-related quality of life (HRQoL), as assessed by the Functional Assessment of Cancer Therapy-Bladder Cancer (FACT-Bl), the Core Lower Urinary Tract Symptom Score (CLSS), and the European Quality of Life Five Dimensions Questionnaire (EQ-5D).
Gastric Cancer: KEYNOTE-811: Controlled trial of combination therapy in HER2-positive gastric cancer patients naïve to treatment: The efficacy of Pembrolizumab (KEYTRUDA) in combination with trastuzumab plus fluoropyrimidine and platinum chemotherapy was investigated in KEYNOTE-811, a multicenter, randomized, double-blind, placebo-controlled trial that was designed to enroll 692 patients with HER2-positive advanced gastric or gastroesophageal junction (GEJ) adenocarcinoma regardless of PD-L1 expression status, who had not previously received systemic therapy for metastatic disease. Patients with an autoimmune disease that required systemic therapy within 2 years of treatment or a medical condition that required immunosuppression were ineligible. Randomization was stratified by PD-L1 expression (CPS ≥1 or <1), chemotherapy regimen (5-FU plus cisplatin [FP] or capecitabine plus oxaliplatin [CAPOX]), and geographic region (Europe/Israel/North America/Australia, Asia or Rest of the World). Patients were randomized (1:1) to one of the following treatment arms; all study medications, except oral capecitabine, were administered as an intravenous infusion for every 3-week cycle: Pembrolizumab (KEYTRUDA) 200 mg, trastuzumab 8 mg/kg on first infusion and 6 mg/kg in subsequent cycles, followed by investigator's choice of combination chemotherapy of cisplatin 80 mg/m
2 for up to 6 cycles and 5-FU 800 mg/m
2/day for 5 days (FP) or oxaliplatin 130 mg/m
2 up to 6-8 cycles and capecitabine 1000 mg/m
2 bid for 14 days (CAPOX). Pembrolizumab (KEYTRUDA) was administered prior to trastuzumab and chemotherapy on Day 1 of each cycle.
Placebo, trastuzumab 8 mg/kg on first infusion and 6 mg/kg in subsequent cycles, followed by investigator's choice of combination chemotherapy of cisplatin 80 mg/m
2 for up to 6 cycles and 5-FU 800 mg/m
2/day for 5 days (FP) or oxaliplatin 130 mg/m
2 up to 6-8 cycles and capecitabine 1000 mg/m
2 bid for 14 days (CAPOX). Placebo was administered prior to trastuzumab and chemotherapy on Day 1 of each cycle.
Treatment with Pembrolizumab (KEYTRUDA), trastuzumab and chemotherapy or placebo, trastuzumab and chemotherapy continued until RECIST v1.1defined progression of disease as determined by BICR, unacceptable toxicity, or a maximum of 24 months. Treatment was permitted beyond RECIST-defined disease progression if the patient was clinically stable and deriving clinical benefit as determined by the investigator. Assessment of tumor status was performed every 6 weeks. The efficacy outcome measures assessed were ORR and DoR by BICR using RECIST v1.1, modified to follow a maximum of 10 target lesions and a maximum of 5 target lesions per organ.
At the time of analysis, ORR and DoR were assessed for the first 264 patients among a total of 434 patients randomized, including 133 patients in the Pembrolizumab (KEYTRUDA) arm and 131 in the placebo arm. According to the statistical design of the study, OS and PFS were not evaluated at this interim analysis. Among the 264 patients, the population characteristics were: median age of 62 years (range: 19 to 84), 41% age 65 or older; 82% male; 63% White, 31% Asian, and 0.8 % Black; 47% ECOG PS of 0 and 53% ECOG PS of 1. Ninety-seven percent of patients had metastatic disease (stage IV) and 3% had locally advanced unresectable disease. Eighty-seven percent had tumors that expressed PD-L1 with a CPS ≥1. Ninety-one percent (n=240) had tumors that were not MSI-H, 1% (n=2) had tumors that were MSI-H, and in 8% (n=22) the status was not known. Eighty-seven percent of patients received CAPOX.
A statistically significant improvement in ORR was demonstrated in patients randomized to Pembrolizumab (KEYTRUDA) in combination with trastuzumab and chemotherapy compared with placebo in combination with trastuzumab and chemotherapy. Efficacy results are summarized in Table 23. (See Table 23.)
Click on icon to see table/diagram/image
KEYNOTE-059: Open-label study in gastric cancer patients previously treated with chemotherapy: The efficacy of Pembrolizumab (KEYTRUDA) was investigated in KEYNOTE059, a multicenter, non-randomized, open-label multi-cohort trial that enrolled 259 patients with gastric or gastroesophageal junction (GEJ) adenocarcinoma who progressed on at least two prior systemic treatments for advanced disease. Previous treatment must have included a fluoropyrimidine and platinum doublet. HER2/neu-positive patients must have previously received treatment with approved HER2/neu-targeted therapy. Patients with active autoimmune disease or a medical condition that required immunosuppression or with clinical evidence of ascites by physical exam were ineligible.
Patients received Pembrolizumab (KEYTRUDA) 200 mg every 3 weeks until unacceptable toxicity or disease progression that was symptomatic, rapidly progressive, required urgent intervention, occurred with a decline in performance status, or was confirmed at least 4 weeks later with repeat imaging. Patients without disease progression were treated for up to 24 months. Assessment of tumor status was performed every 6 to 9 weeks. The major efficacy outcome measures were ORR according to RECIST 1.1, as assessed by blinded independent central review, and duration of response.
Among the 259 patients, 57% (n=148) had tumors that expressed PD-L1 with a combined positive score (CPS) of greater than or equal to 1. PD-L1 status was determined using the PD-L1 IHC 22C3 pharmDx Kit. The baseline characteristics of these 148 patients were: median age 64 years (47% age 65 or older); 77% male; 82% White, 12% Asian; and ECOG PS of 0 (43%) and 1 (57%). Eighty-five percent had M1 disease and 7% had M0 disease. Fifty-one percent had two and 49% had three or more prior lines of therapy in the recurrent or metastatic setting. (See Table 24.)
Click on icon to see table/diagram/image
Esophageal Cancer: KEYNOTE-590: First-line treatment of locally advanced unresectable or metastatic Esophageal Cancer/Gastroesophageal Junction: The efficacy of Pembrolizumab (KEYTRUDA) was investigated in KEYNOTE-590, a multicenter, randomized, placebo-controlled trial that enrolled 749 patients as a first-line treatment in patients with locally advanced unresectable or metastatic carcinoma of the esophagus and gastroesophageal junction. All patients were required to have tumor specimens for PD-L1 testing at a central laboratory; PD-L1 status was determined using the PD-L1 IHC 22C3 pharmDx kit. Patients with active autoimmune disease, a medical condition that required immunosuppression, or known HER-2 positive GEJ adenocarcinoma patients were ineligible. Randomization was stratified by tumor histology (squamous cell carcinoma vs. adenocarcinoma), geographic region (Asia vs. ex-Asia), and ECOG performance status (0 vs. 1).
Patients were randomized (1:1) to one of the following treatment arms; all study medications were administered via intravenous infusion: Pembrolizumab (KEYTRUDA) 200 mg on Day 1 of each three-week cycle in combination with cisplatin 80 mg/m
2 IV on Day 1 of each three-week cycle for up to six cycles and 5-FU 800 mg/m
2 IV per day on Day 1 to Day 5 of each three-week cycle, or per local standard for 5-FU administration, for up to 24 months.
Placebo on Day 1 of each three-week cycle in combination with cisplatin 80 mg/m
2 IV on Day 1 of each three-week cycle for up to six cycles and 5-FU 800 mg/m
2 IV per day on Day 1 to Day 5 of each three-week cycle, or per local standard for 5-FU administration, for up to 24 months.
Treatment with Pembrolizumab (KEYTRUDA) or chemotherapy continued until unacceptable toxicity or disease progression. Patients randomized to Pembrolizumab (KEYTRUDA) were permitted to continue beyond the first RECIST v1.1-defined disease progression if clinically stable until the first radiographic evidence of disease progression was confirmed at least 4 weeks later with repeat imaging. Patients treated with Pembrolizumab (KEYTRUDA) without disease progression could be treated for up to 24 months. Assessment of tumor status was performed every 9 weeks. The major efficacy outcome measures were OS and PFS as assessed by the investigator according to RECIST v1.1. Secondary efficacy outcome measures were ORR and DoR, according to RECIST v1.1, as assessed by the investigator.
The baseline characteristics were: median age of 63 years (range: 27 to 94), 43% age 65 or older; 83% male; 37% White and 53% Asian; 40% had an ECOG PS of 0 and 60% had an ECOG PS of 1. Ninety-one percent had M1 disease and 9% had M0 disease. Seventy-three percent had a tumor histology of squamous cell carcinoma, and 27% had adenocarcinoma.
Pembrolizumab (KEYTRUDA), in combination with chemotherapy, demonstrated a statistically significant and clinically meaningful improvement in OS and PFS when compared to chemotherapy (cisplatin and 5-FU) in previously untreated participants with locally advanced unresectable or metastatic carcinoma of the esophagus or gastroesophageal junction. The investigator-assessed results were consistent with BICR.
Table 25 summarizes the key efficacy measures for KEYNOTE-590. The Kaplan-Meier curves for OS and PFS are shown in Figures 21 and 22. (See Table 25, Figures 21 and 22.)
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Previously treated recurrent locally advanced or metastatic Esophageal Cancer: KEYNOTE-181: Controlled trial in esophageal cancer patients previously treated with systemic therapy: The efficacy of Pembrolizumab (KEYTRUDA) was investigated in Study KEYNOTE-181, a multicenter, randomized, open-label, active-controlled trial that enrolled 628 patients with esophageal cancer who progressed on or after prior systemic treatment for advanced disease. Patients with active autoimmune disease or a medical condition that required immunosuppression were ineligible.
Patients were randomized to receive either Pembrolizumab (KEYTRUDA) 200 mg every 3 weeks (N=314) or investigator's choice of any of the following chemotherapy regimens given intravenously: paclitaxel 80-100 mg/m
2 on Days 1, 8, and 15 of every 4-week cycle (N=145), docetaxel 75 mg/m
2 every 3 weeks (N=78), or irinotecan 180 mg/m
2 every 2 weeks (N=73). Treatment continued until unacceptable toxicity or disease progression. Clinically stable patients with initial evidence of disease progression were permitted to remain on treatment until disease progression was confirmed. Patients without disease progression were treated for up to 24 months. Treatment with pembrolizumab could be reinitiated for subsequent disease progression and administered for up to 1 additional year. Assessment of tumor status was performed every 9 weeks. The major efficacy outcome measure was OS. Additional efficacy outcome measures were PFS, ORR, and duration of response according to RECIST 1.1, as assessed by blinded independent central review.
Among the 628 patients, 35.4% (n = 222) had tumors that expressed PD-L1 with a combined positive score (CPS) of greater than or equal to 10. PD-L1 status was determined using the PD-L1 IHC 22C3 pharmDx Kit. The baseline characteristics of these 222 patients were: median age of 64 years (range: 33 to 81), 48% age 65 or older; 86% male; 45% White; 52% Asian; 36% had an ECOG PS of 0 and 64% had an ECOG PS of 1; 75% had squamous cell and 25% had adenocarcinoma histology; and 1% had a history of brain metastases. Ninety-one percent had M1 disease and 9% had M0 disease.
The trial demonstrated a statistically significant improvement in OS for patients whose tumors express PD-L1 with CPS ≥10 randomized to Pembrolizumab (KEYTRUDA) monotherapy as compared with chemotherapy. Table 26 summarizes the key efficacy measures for the CPS ≥10 population. The Kaplan-Meier curves for OS and PFS for the CPS ≥10 population are shown in Figures 23 and 24. (See Table 26, Figures 23 and 24.)
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
KEYNOTE-180: Open-label trial in esophageal cancer patients previously treated with chemotherapy: The efficacy of Pembrolizumab (KEYTRUDA) was investigated in KEYNOTE-180, a multicenter, nonrandomized, open-label trial that enrolled 121 patients with esophageal cancer who progressed on at least 2 prior systemic treatments for advanced disease. Patients with active autoimmune disease or a medical condition that required immunosuppression were ineligible.
Patients received Pembrolizumab (KEYTRUDA) 200 mg every 3 weeks until unacceptable toxicity or disease progression. Clinically stable patients with initial evidence of disease progression were permitted to remain on treatment until disease progression was confirmed. Patients without disease progression were treated for up to 24 months. Treatment with pembrolizumab could be reinitiated for subsequent disease progression and administered for up to 1 additional year. Assessment of tumor status was performed every 9 weeks. The major efficacy outcome measures were ORR and duration of response according to RECIST 1.1, as assessed by blinded independent central review.
Among the 121 patients, the baseline characteristics were: median age of 65 years (range: 33 to 87), 53% age 65 or older; 83% male; 59% White; 35% Asian; 36% had an ECOG PS of 0 and 64% had an ECOG PS of 1; 52% had squamous cancer and 48% had adenocarcinoma histology (of which 31% had GEJ tumors) and 4% had history of brain metastases. Ninety-nine percent had M1 disease and 1% had M0 disease. Eighty-eight percent had two and 12% had three or more prior lines of therapy in the recurrent or metastatic setting.
Efficacy results for KEYNOTE-180 are summarized in Table 27. (See Table 27.)
Click on icon to see table/diagram/image
Microsatellite Instability-High Cancer: KEYNOTE-164 and KEYNOTE-158 Open-label studies in patients with MSI-H, including mismatch repair deficient (dMMR), cancer who have received prior therapy: The efficacy of Pembrolizumab (KEYTRUDA) was investigated in 155 patients with MSI-H or dMMR cancer enrolled in two multicenter, non-randomized, open-label, multi-cohort Phase II studies (KEYNOTE-164 and KEYNOTE-158). Regardless of histology, MSI or MMR tumor status was determined using polymerase chain reaction (PCR) or immunohistochemistry (IHC), respectively. Efficacy was evaluated in 61 patients enrolled in KEYNOTE-164 with advanced MSI-H or dMMR colorectal cancer (CRC) that progressed following treatment with a fluoropyrimidine, oxaliplatin, and irinotecan. Efficacy was also evaluated in 94 patients enrolled in KEYNOTE-158 with advanced MSI-H or dMMR non-colorectal cancer (non-CRC) who had disease progression following prior therapy. Patients with autoimmune disease or a medical condition that required immunosuppression were ineligible for either trial.
Patients received Pembrolizumab (KEYTRUDA) 200 mg every 3 weeks until unacceptable toxicity or disease progression. Clinically stable patients with initial evidence of disease progression were permitted to remain on treatment until disease progression was confirmed. Patients without disease progression were treated for up to 24 months. Treatment with pembrolizumab could be reinitiated for subsequent disease progression and administered for up to 1 additional year. Assessment of tumor status in KEYNOTE-164 was performed every 9 weeks and in KEYNOTE-158 every 9 weeks through the first year, then every 12 weeks thereafter. The major efficacy outcome measures were ORR and duration of response according to RECIST 1.1.
Among the 155 patients with MSI-H cancer, the baseline characteristics were: median age 60 years (40% age 65 or older); 55% male; 78% White, 20% Asian; and ECOG PS 0 (49%) and 1 (51%). Ninety-three percent of patients had M1 disease and 6% had M0 disease. Ninety percent of patients with CRC and 51% of patients with non-CRC received two or more prior lines of therapy.
The median follow-up time for 155 patients treated with Pembrolizumab (KEYTRUDA) was 9.7 months. Efficacy results are summarized in Table 28 and Table 29. (See Tables 28 and 29.)
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Colorectal Cancer: KEYNOTE-177: Controlled trial for first-line treatment of patients with MSI-H or dMMR CRC: The efficacy of Pembrolizumab (KEYTRUDA) was investigated in KEYNOTE-177, a multicenter, randomized, open-label, active-controlled trial that enrolled 307 patients with previously untreated unresectable or metastatic MSI-H or dMMR CRC. MSI or MMR tumor status was determined locally using polymerase chain reaction (PCR) or immunohistochemistry (IHC), respectively. Patients with autoimmune disease or a medical condition that required immunosuppression were ineligible.
Patients were randomized (1:1) to receive Pembrolizumab (KEYTRUDA) 200 mg intravenously every 3 weeks or investigator's choice of the following chemotherapy regimens given intravenously every 2 weeks: mFOLFOX6 (oxaliplatin, leucovorin, and FU) or mFOLFOX6 in combination with either bevacizumab or cetuximab: Oxaliplatin 85 mg/m
2, leucovorin 400 mg/m
2 (or levoleucovorin 200 mg/m
2), and FU 400 mg/m
2 bolus on Day 1, then FU 2400 mg/m
2 over 46-48 hours. Bevacizumab 5 mg/kg on Day 1 or cetuximab 400 mg/m
2 on first infusion, then 250 mg/m
2 weekly.
FOLFIRI (irinotecan, leucovorin, and FU) or FOLFIRI in combination with either bevacizumab or cetuximab: Irinotecan 180 mg/m
2, leucovorin 400 mg/m
2 (or levoleucovorin 200 mg/m
2), and FU 400 mg/m
2 bolus on Day 1, then FU 2400 mg/m
2 over 46-48 hours. Bevacizumab 5 mg/kg on Day 1 or cetuximab 400 mg/m
2 on first infusion, then 250 mg/m
2 weekly.
Treatment with Pembrolizumab (KEYTRUDA) or chemotherapy continued until RECIST v1.1-defined progression of disease as determined by the investigator or unacceptable toxicity. Patients treated with Pembrolizumab (KEYTRUDA) without disease progression could be treated for up to 24 months.
Assessment of tumor status was performed every 9 weeks. Patients randomized to chemotherapy were offered Pembrolizumab (KEYTRUDA) at the time of disease progression. The primary efficacy outcome measures included PFS assessed by BICR according to RECIST v1.1. Secondary outcome measures were ORR and DoR.
A total of 307 patients were enrolled and randomized to Pembrolizumab (KEYTRUDA) (n=153) or chemotherapy (n=154). The baseline characteristics of these 307 patients were: median age of 63 years (range: 24 to 93), 47% age 65 or older; 50% male; 75% White and 16% Asian; 52% had an ECOG PS of 0 and 48% had an ECOG PS of 1. Mutation status: 25% BRAF V600E, 24% KRAS/NRAS. For 143 patients treated with chemotherapy, 56% received mFOLFOX6 with or without bevacizumab or cetuximab and 44% received FOLFIRI with or without bevacizumab or cetuximab.
The trial demonstrated a statistically significant improvement in PFS for patients randomized to Pembrolizumab (KEYTRUDA) compared with chemotherapy. The median follow-up time was 27.6 months (range: 0.2 to 48.3 months). Table 30 and Figure 25 summarize the key efficacy measures for KEYNOTE-177. (See Table 30 and Figure 25.)
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Exploratory analyses of patient-reported outcomes (PROs) using EORTC QLQ-C30 show improvement in global health status/quality of life, functioning (i.e., physical, role, social) and fatigue in patients treated with Pembrolizumab (KEYTRUDA) compared to a decline for patients treated with chemotherapy at pre-specified Week 18. Improvements from baseline in global health status/quality of life continued through Week 45 for patients treated with Pembrolizumab (KEYTRUDA). In addition, a prolonged time to deterioration in global health status/QoL (HR 0.61; 95% CI 0.38-0.98), physical (HR 0.50; 95% CI 0.32-0.81) and social functioning (HR 0.53; 95% CI 0.32-0.87), and fatigue (HR 0.48; 95% CI 0.33-0.69) was observed for patients treated with Pembrolizumab (KEYTRUDA) compared to chemotherapy. These results should be interpreted in the context of the open-label study design and therefore taken cautiously.
Hepatocellular Carcinoma: KEYNOTE-224 Open-label study in patients with HCC, previously treated with sorafenib, an antiangiogenic TKI: The efficacy of Pembrolizumab (KEYTRUDA) was investigated in KEYNOTE-224 a single-arm, open-label, multicenter trial in 104 patients with HCC who had disease progression on or after sorafenib, an anti-angiogenic TKI, or were intolerant to sorafenib. Additional eligibility included at least one measurable lesion confirmed by the central imaging vendor per RECIST 1.1 and Child Pugh class A.
Patients with active and inactive hepatitis B virus (HBV) as well as patients with past or ongoing hepatitis C virus (HCV) infection were eligible for the trial. Patients with active autoimmune disease, greater than one etiology of hepatitis, a medical condition that required immunosuppression, or clinical evidence of ascites by physical exam were ineligible for the trial.
Patients received Pembrolizumab (KEYTRUDA) 200 mg every 3 weeks until unacceptable toxicity or confirmed disease progression. Patients without disease progression were treated for up to 24 months. Assessment of tumor status was performed every 9 weeks. The major efficacy outcome measures were ORR according to RECIST 1.1, as assessed by BICR and duration of response.
Among the 104 patients treated, the baseline characteristics were: median age 68 years (67% age 65 or older); 83% male; 81% White, 14% Asian; ECOG PS of 0 (61%) or 1 (39%); Child Pugh class A (94%) and B (6%); 21% HBV positive (active or inactive) and 25% HCV positive (past or ongoing). Sixty-four percent (64%) of patients had extrahepatic disease, 17% had vascular invasion, and 41% had alfa-fetoprotein (AFP) levels greater than 200 ng/mL. Prior treatment history included surgery (33%), radiation (14%), or locoregional treatment (39%). All patients received prior sorafenib; reasons for discontinuation were intolerance in 21 patients (20%) and progressive disease in 83 patients (80%). Efficacy results are summarized in Table 31. (See Table 31.)
Click on icon to see table/diagram/image
Cervical Cancer: KEYNOTE-826: Controlled trial of combination therapy in patients with persistent, recurrent, or metastatic cervical cancer: The efficacy of Pembrolizumab (KEYTRUDA) in combination with paclitaxel and cisplatin or paclitaxel and carboplatin, with or without bevacizumab, was investigated in KEYNOTE826, a multicenter, randomized, double-blind, placebo-controlled trial that enrolled 617 patients with persistent, recurrent, or first-line metastatic cervical cancer who had not been treated with chemotherapy except when used concurrently as a radio-sensitizing agent. Patients with autoimmune disease that required systemic therapy within 2 years of treatment or a medical condition that required immunosuppression were ineligible. Randomization was stratified by metastatic status at initial diagnosis, investigator decision to use bevacizumab, and PD-L1 status (CPS <1 vs. CPS 1 to <10 vs. CPS ≥10). Patients were randomized (1:1) to one of the two treatment groups: Treatment Group 1: Pembrolizumab (KEYTRUDA) 200 mg plus chemotherapy; Treatment Group 2: Placebo plus chemotherapy.
The investigator selected one of the following four treatment regimens prior to randomization: Paclitaxel 175 mg/m
2 + cisplatin 50 mg/m
2; Paclitaxel 175 mg/m
2 + cisplatin 50 mg/m
2 + bevacizumab 15 mg/kg; Paclitaxel 175 mg/m
2; carboplatin AUC 5 mg/mL/min; Paclitaxel 175 mg/m
2 + carboplatin AUC 5 mg/mL/min + bevacizumab 15 mg/kg.
All study medications were administered as an intravenous infusion. All study treatments were administered on Day 1 of each 3-week treatment cycle. Cisplatin could be administered on Day 2 of each 3-week treatment cycle. The option to use bevacizumab was by investigator choice prior to randomization. Treatment with Pembrolizumab (KEYTRUDA) continued until RECIST v1.1-defined progression of disease, unacceptable toxicity, or a maximum of 24 months. Administration of Pembrolizumab (KEYTRUDA) was permitted beyond RECIST-defined disease progression if the patient was clinically stable and considered to be deriving clinical benefit by the investigator. Assessment of tumor status was performed at Week 9 and then every 9 weeks for the first year, followed by every 12 weeks thereafter. The primary efficacy outcome measures were OS and PFS as assessed by investigator according to RECIST v1.1. Secondary efficacy outcome measures were ORR and DoR, according to RECIST v1.1, as assessed by investigator.
The study population characteristics were: median age of 51 years (range: 22 to 82), 16% age 65 or older; 58% White,18% Asian, and 1% Black; 37% Hispanic or Latino; 56% and 43% ECOG performance status of 0 or 1, respectively; 89% with PD-L1 CPS ≥1; 63% received bevacizumab as study treatment; 23% with adenocarcinoma and 5% with adeno-squamous histology; for patients with persistent or recurrent disease with or without distant metastases, 39% had received prior chemoradiation only and 17% had received prior chemoradiation plus surgery.
The study demonstrated statistically significant improvements in OS and PFS for patients randomized to Pembrolizumab (KEYTRUDA) in combination with chemotherapy with or without bevacizumab compared to placebo in combination with chemotherapy with or without bevacizumab at a pre-specified interim analysis in the overall population. The median follow-up time was 17.2 months (range: 0.3 to 29.4 months).
Efficacy results are summarized in Table 32, Figure 26, and Figure 27. (See Table 32, Figures 26 and 27.)
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Patient reported outcomes (PROs) were assessed using EQ-5D-5L. A prolonged time to deterioration in EQ-5D-5L was observed for patients treated with pembrolizumab plus chemotherapy compared to placebo plus chemotherapy (HR 0.75; 95% CI 0.580.97). Over 30 weeks of follow-up, more patients treated with pembrolizumab plus chemotherapy had improved or stable health status/QoL (78.3% vs. 71.1%).
KEYNOTE-158: Open-label study in recurrent or metastatic cervical cancer patients previously treated with chemotherapy: The efficacy of Pembrolizumab (KEYTRUDA) was investigated in 98 patients with recurrent or metastatic cervical cancer enrolled in a single cohort in KEYNOTE-158, a multicenter, non-randomized, open-label, multi-cohort trial. The trial excluded patients with autoimmune disease or a medical condition that required immunosuppression.
Patients received Pembrolizumab (KEYTRUDA) at a dose of 200 mg every 3 weeks until unacceptable toxicity or documented disease progression. Clinically stable patients with initial evidence of disease progression were permitted to remain on treatment until disease progression was confirmed. Patients without disease progression could be treated for up to 24 months. Assessment of tumor status was performed every 9 weeks for the first 12 months, and every 12 weeks thereafter. The major efficacy outcome measures were ORR according to RECIST 1.1, as assessed by blinded independent central review, and duration of response.
Among the 98 patients with cervical cancer, 77 (79%) had tumors that expressed PD-L1 with a CPS ≥1 and received at least one line of chemotherapy for recurrent or metastatic disease. PD-L1 status was determined using the PD-L1 IHC 22C3 pharmDx Kit. The baseline characteristics of these 77 patients were: median age 45 years (range: 27 to 75 years); 81% White, 14% Asian, 3% Black; ECOG PS 0 (32%) and 1 (68%); 92% had squamous cell carcinoma, 6% adenocarcinoma, and 1% adeno-squamous histology; 95% had M1 disease and 5% had recurrent disease; 35% had one and 65% had two or more prior lines of therapy in the recurrent or metastatic setting.
No responses were observed in patients whose tumors did not have PD-L1 expression (CPS <1) (n=15).
The median follow-up time in patients with PD-L1 (CPS ≥1) and who received at least one line of chemotherapy for recurrent or metastatic disease was 11.7 months. Efficacy results are summarized in Table 33. (See Table 33.)
Click on icon to see table/diagram/image
Renal Cell Carcinoma: KEYNOTE-426: Controlled trial of combination therapy with axitinib for first-line treatment of patients with advanced RCC: The efficacy of Pembrolizumab (KEYTRUDA) in combination with axitinib was investigated in a randomized, multicenter, open-label, active-controlled trial KEYNOTE-426, conducted in patients with advanced RCC, regardless of PD-L1 tumor status and International Metastatic RCC Database Consortium (IMDC) risk group categories. The trial excluded patients with autoimmune disease or a medical condition that required immunosuppression. Randomization was stratified by risk categories (favorable versus intermediate versus poor) and geographic region (North America versus Western Europe versus "Rest of the World"). Patients were randomized (1:1) to one of the following treatment arms: Pembrolizumab (KEYTRUDA) 200 mg intravenously every 3 weeks in combination with axitinib 5 mg orally, twice daily. Patients who tolerated axitinib 5 mg twice daily for 2 consecutive treatment cycles (i.e., 6 weeks) with no > Grade 2 treatment-related adverse events to axitinib and with blood pressure well controlled to ≤ 150/90 mm Hg were permitted dose escalation of axitinib to 7 mg twice daily. Dose escalation of axitinib to 10 mg twice daily was permitted using the same criteria. Axitinib could be interrupted or reduced to 3 mg twice daily and subsequently to 2 mg twice daily to manage toxicity.
Sunitinib 50 mg orally, once daily for 4 weeks and then off treatment for 2 weeks.
Treatment with Pembrolizumab (KEYTRUDA) and axitinib continued until RECIST 1.1-defined progression of disease as verified by BICR or confirmed by the investigator, unacceptable toxicity, or for Pembrolizumab (KEYTRUDA), a maximum of 24 months. Administration of Pembrolizumab (KEYTRUDA) and axitinib was permitted beyond RECIST-defined disease progression if the patient was clinically stable and considered to be deriving clinical benefit by the investigator. Assessment of tumor status was performed at baseline, after randomization at Week 12, then every 6 weeks thereafter until Week 54, and then every 12 weeks thereafter. Chemistry and hematology laboratory tests were performed at each cycle.
Among the 861 patients in KEYNOTE-426 (432 patients in the Pembrolizumab (KEYTRUDA) combination arm and 429 in the sunitinib arm), baseline characteristics were: median age of 62 years (range: 26 to 90); 38% age 65 or older; 73% male; 79% White and 16% Asian; 99.9% had a Karnofsky Performance Score (KPS) of ≥70%; patient distribution by IMDC risk categories was 31% favorable, 56% intermediate and 13% poor.
The primary efficacy outcome measures were OS and PFS (as assessed by BICR according to RECIST 1.1). Secondary efficacy outcome measures were ORR and response duration, as assessed by BICR using RECIST 1.1. The median follow-up time for 432 patients treated with Pembrolizumab (KEYTRUDA) and axitinib was 13.2 months (range: 0.1 - 21.5 months). Table 34 summarizes key efficacy measures. Improvements in OS, PFS and ORR were shown consistently across all tested subgroups, including subgroups by IMDC risk category and PD-L1 tumor expression status. (See Table 34, Figures 28 and 29.)
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
KEYNOTE 581: Controlled trial of combination therapy with lenvatinib for first-line treatment of patients with advanced RCC: The efficacy of Pembrolizumab (KEYTRUDA) in combination with lenvatinib was investigated in KEYNOTE-581, a multicenter, open-label, randomized trial conducted in 1069 patients with advanced RCC in the first-line setting. Patients were enrolled regardless of PD-L1 tumor expression status. Patients with active autoimmune disease or a medical condition that required immunosuppression were ineligible. Randomization was stratified by geographic region (North America versus Western Europe versus "Rest of the World") and Memorial Sloan Kettering Cancer Center (MSKCC) prognostic groups (favorable versus intermediate versus poor).
Patients were randomized (1:1:1) to one of the following treatment arms: Pembrolizumab (KEYTRUDA) 200 mg intravenously every 3 weeks up to 24 months in combination with lenvatinib 20 mg orally once daily.
Lenvatinib 18 mg orally once daily in combination with everolimus 5 mg orally once daily.
Sunitinib 50 mg orally once daily for 4 weeks then off treatment for 2 weeks.
Treatment continued until unacceptable toxicity or disease progression as determined by the investigator and confirmed by BICR using RECIST 1.1. Administration of Pembrolizumab (KEYTRUDA) with lenvatinib was permitted beyond RECIST-defined disease progression if the patient was clinically stable and considered by the investigator to be deriving clinical benefit. Pembrolizumab (KEYTRUDA) was continued for a maximum of 24 months; however, treatment with lenvatinib could be continued beyond 24 months. Assessment of tumor status was performed at baseline and then every 8 weeks.
Among the 1069 patients in KEYNOTE 581 (355 patients in the Pembrolizumab (KEYTRUDA) with lenvatinib arm, 357 patients in the lenvatinib with everolimus arm, and 357 patients in the sunitinib arm), the study population characteristics were: median age of 62 years (range: 29 to 88 years); 42% age 65 or older; 75% male; 74% White, 21% Asian, 1% Black, and 2% other races; 18% and 82% of patients had a baseline KPS of 70 to 80 and 90 to 100, respectively; patient distribution by IMDC risk categories was 33% favorable, 56% intermediate and 10% poor, and by MSKCC risk categories was 27% favorable, 64% intermediate and 9% poor. Common sites of metastases in patients were lung (68%), lymph node (45%), and bone (25%).
The primary efficacy outcome measure was PFS based on BICR using RECIST 1.1. Key secondary efficacy outcome measures included OS and ORR. The trial demonstrated statistically significant improvements in PFS, OS, and ORR in patients randomized to Pembrolizumab (KEYTRUDA) in combination with lenvatinib compared with sunitinib. The median overall survival follow-up time was 26.6 months. Efficacy results for KEYNOTE-581 are summarized in Table 35 and Figures 30 and 31. Consistent results were observed across pre-specified subgroups, MSKCC prognostic groups and PDL1 tumor expression status. (See Table 35, Figures 30 and 31.)
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Patient-reported outcomes (PROs) were assessed using the European Organization for the Research and Treatment of Cancer (EORTC) QLQ-30 and Kidney Cancer Symptom Index (FKSI-DRS). From baseline to a mean follow-up time of 46 weeks, patients treated with pembrolizumab in combination with lenvatinib had better physical functioning, fatigue, dyspnea, and constipation scores compared to the sunitinib group. Compared to sunitinib, pembrolizumab in combination with lenvatinib showed a more than 12 week delay in median time to worsening in global health status (GHS), physical functioning and patient reported symptoms with no subsequent recovery: EORTC QLQ-C30 GHS (114 vs. 75 weeks, HR=0.6 [95% CI: 0.47, 0.77]), physical functioning (134 vs 78 weeks, HR=0.52 [95% CI: 0.41, 0.67]), fatigue (110 vs. 59 weeks, HR=0.54 [95% CI: 0.43, 0.67]), insomnia (156 vs. 126 weeks, HR=0.63 [95% CI: 0.47. 0.85]), dyspnea (153 vs. 126 weeks, HR=0.56 [95% CI: 0.41, 0.76]), nausea and vomiting (147 vs 131 weeks, HR=0.53 [95% CI: 0.39, 0.74]), pain (119 vs. 105 weeks, HR=0.68 [95% CI: 0.53, 0.87]) and FKSI-DRS (134 vs. 117 weeks, HR=0.7 [95% CI: 0.53, 0.92]). These results should be interpreted in the context of the open-label study design and therefore taken cautiously.
KEYNOTE-564: Placebo-controlled study for the adjuvant treatment of patients with resected RCC: The efficacy of Pembrolizumab (KEYTRUDA) was investigated as adjuvant therapy for RCC in KEYNOTE--564, a multicenter, randomized, double-blind, placebo-controlled study in 994 patients with intermediate-high or high risk of recurrence of RCC, or M1 no evidence of disease (NED). The intermediate high-risk category included: pT2 with Grade 4 or sarcomatoid features; pT3, any Grade without nodal involvement (N0) or distant metastases (M0). The high-risk category included: pT4, any Grade N0 and M0; any pT, any Grade with nodal involvement and M0. The M1 NED category included patients with metastatic disease who had undergone complete resection of primary and metastatic lesions. Patients must have undergone a partial nephroprotective or radical complete nephrectomy (and complete resection of solid, isolated, soft tissue metastatic lesion(s) in M1 NED participants) with negative surgical margins ≥4 weeks prior to the time of screening. Patients with active autoimmune disease or a medical condition that required immunosuppression were ineligible. Patients were randomized (1:1) to receive Pembrolizumab (KEYTRUDA) 200 mg every 3 weeks (n=496) or placebo (n=498) for up to 1 year until disease recurrence or unacceptable toxicity. Randomization was stratified by metastasis status (M0, M1 NED), within M0 group, further stratified by ECOG PS (0,1), and geographic region (US, non-US). Patients underwent imaging every 12 weeks for the first 2 years from randomization, then every 16 weeks from year 3 to 5, and then every 24 weeks annually.
Among the 994 patients, the baseline characteristics were: median age of 60 years (range: 25 to 84), 33% age 65 or older; 71% male; and 85% ECOG PS of 0 and 15% ECOG PS of 1. Ninety-four percent were N0; 84% had no sarcomatoid features; 86% were pT2 with Grade 4 or sarcomatoid features or pT3; 8% were pT4 or with nodal involvement; and 6% were M1 NED. Baseline characteristics and demographics were generally comparable between the Pembrolizumab (KEYTRUDA) and placebo arms.
The primary efficacy outcome measure was investigator-assessed disease-free survival (DFS). The key secondary outcome measure was OS. The study demonstrated a statistically significant improvement in DFS for patients randomized to the Pembrolizumab (KEYTRUDA) arm compared with placebo. Consistent results were observed across pre-specified subgroups. At the time of analysis, OS results were not yet mature with 18 deaths out of 496 patients in the Pembrolizumab (KEYTRUDA) arm and 33 deaths out of 498 patients in the placebo arm. The median follow-up time was 23.9 months (range 2.5 to 41.5 months). Efficacy results are summarized in Table 36 and Figure 32. (See Table 36 and Figure 32.)
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Endometrial Carcinoma: KEYNOTE-775: Controlled trial of combination therapy in advanced endometrial carcinoma patients previously treated with systemic therapy: The efficacy of Pembrolizumab (KEYTRUDA) in combination with lenvatinib was investigated in a multicenter, randomized, active-controlled, open-label trial, KEYNOTE-775, conducted in 827 patients with advanced, endometrial carcinoma who had been previously treated with at least one prior platinum-based chemotherapy regimen in any setting, including in the neoadjuvant and adjuvant settings. The trial excluded patients with endometrial sarcoma, including carcinosarcoma, or patients who had active autoimmune disease or a medical condition that required immunosuppression. Randomization was stratified by MMR status (dMMR or pMMR [not dMMR]). The pMMR stratum was further stratified by ECOG performance status, geographic region, and history of pelvic radiation. Patients were randomized (1:1) to one of the following treatment arms: Pembrolizumab (KEYTRUDA) 200 mg intravenously every 3 weeks in combination with lenvatinib 20 mg orally once daily.
Investigator's choice consisting of either doxorubicin 60 mg/m
2 every 3 weeks, or paclitaxel 80 mg/m
2 given weekly, 3 weeks on/1 week off.
Treatment with Pembrolizumab (KEYTRUDA) and lenvatinib continued until RECIST 1.1-defined progression of disease as verified by BICR, unacceptable toxicity, or for Pembrolizumab (KEYTRUDA), a maximum of 24 months. Treatment was permitted beyond RECIST 1.1-defined disease progression if the treating investigator considered the patient to be deriving clinical benefit and the treatment was tolerated. Assessment of tumor status was performed every 8 weeks.
A total of 827 patients were enrolled and randomized to Pembrolizumab (KEYTRUDA) in combination with lenvatinib (n=411) or investigator's choice of doxorubicin (n=306) or paclitaxel (n=110). Baseline characteristics were: median age of 65 years (range: 30 to 86), 50% age 65 or older; 61% White, 21% Asian, and 4% Black; ECOG PS of 0 (59%) or 1 (41%); and 84% with pMMR tumor status. The histologic subtypes were endometrioid carcinoma (60%), serous (26%), clear cell carcinoma (6%), mixed (5%), and other (3%). All 827 of these patients received prior systemic therapy for endometrial carcinoma: 69% had one, 28% had two, and 3% had three or more prior systemic therapies. Thirty-seven percent of patients received only prior neoadjuvant or adjuvant therapy.
The primary efficacy outcome measures were OS and PFS as assessed by BICR according to RECIST 1.1. Secondary efficacy outcome measures included ORR, as assessed by BICR using RECIST 1.1. The median follow-up time for this trial was 11.4 months (range: 0.3 to 26.9 months). Efficacy measures are summarized in Table 37 and Kaplan-Meier curves for OS and PFS are shown in Figures 33 and 34 respectively. Improvements in OS, PFS, and ORR were consistently demonstrated across pre-specified subgroups, including histology, prior therapies, MMR status, and ECOG performance status. (See Table 37, Figures 33 and 34.)
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
KEYNOTE-146: Open-label study of combination therapy in patients with endometrial carcinoma: The efficacy of Pembrolizumab (KEYTRUDA) in combination with lenvatinib was investigated in a nonrandomized, multicenter, open-label, multi-cohort trial KEYNOTE-146, conducted in 108 patients with endometrial carcinoma that had progressed following at least one prior systemic therapy in any setting. The trial excluded patients with active autoimmune disease or medical conditions that required immunosuppression.
Patients received Pembrolizumab (KEYTRUDA) at a dose of 200 mg intravenously every 3 weeks in combination with lenvatinib 20 mg orally once daily until unacceptable toxicity or disease progression as determined by the investigator. Clinically stable patients who were considered by the investigator to be deriving clinical benefit were permitted to remain on treatment beyond RECIST-defined disease progression. Patients could be treated with Pembrolizumab (KEYTRUDA) for up to 24 months; however, treatment with lenvatinib could be continued beyond 24 months. Assessment of tumor status was performed at baseline and then every 6 weeks until week 24, followed by every 9 weeks thereafter. The major efficacy outcome measures were ORR and duration of response, as assessed by blinded independent central review (BICR) using RECIST 1.1.
Among the 108 patients, 87% (n= 94) had tumors that were not MSI-H or dMMR, 10% (n=11) had tumors that were MSI-H or dMMR, and in 3% (n=3) the status was not known. The baseline characteristics of the 94 patients with tumors that were not MSI-H or dMMR were: median age of 66 years with 62% age 65 or older; 86% White, 6% Black, 4% Asian, 3% other races; and ECOG PS of 0 (52%) or 1 (48%). All 94 of these patients received prior systemic therapy for endometrial carcinoma: 51% had one, 38% had two, and 11% had three or more prior systemic therapies.
Efficacy results are summarized in Table 38. (See Table 38.)
Click on icon to see table/diagram/image
Tumor Mutational Burden-High Cancer: KEYNOTE-158: Open-label study in patients with tumor mutational burden-high (TMB-H) cancer who have received prior therapy: The efficacy of Pembrolizumab (KEYTRUDA) was investigated in a prospectively-planned retrospective analysis of 10 cohorts (A through J) of patients with various previously treated unresectable or metastatic solid tumors with high tumor mutation burden (TMB-H) who were enrolled in a multicenter, non-randomized, open-label trial, KEYNOTE-158. The trial excluded patients who previously received an anti-PD-1 or other immune-modulating monoclonal antibody, or who had an autoimmune disease, or a medical condition that required immunosuppression. Patients received Pembrolizumab (KEYTRUDA) 200 mg intravenously every 3 weeks until unacceptable toxicity or documented disease progression. Assessment of tumor status was performed every 9 weeks for the first 12 months and every 12 weeks thereafter.
The statistical analysis plan pre-specified ≥10 and ≥13 mutations per megabase using the FoundationOne CDx assay as cutpoints to assess TMB. Testing of TMB was blinded with respect to clinical outcomes. The major efficacy outcome measures were ORR and DoR in patients who received at least one dose of Pembrolizumab (KEYTRUDA) as assessed by BICR according to RECIST v1.1.
In KEYNOTE-158, 1050 patients were included in the efficacy analysis population. TMB was analyzed in the subset of 790 patients with sufficient tissue for testing based on protocol-specified testing requirements. Of the 790 patients, 102 (13%) had tumors identified as TMB-H, defined as TMB ≥10 mutations per megabase. Among the 102 patients with TMB-H advanced solid tumors, the study population characteristics were: median age of 61 years (range: 27 to 80), 34% age 65 or older; 34% male; 81% White; and 41% ECOG PS of 0 and 58% ECOG PS of 1. Fifty-six percent of patients had at least two prior lines of therapy.
Efficacy results are summarized in Tables 39 and 40. (See Tables 39 and 40.)
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Triple Negative Breast Cancer: KEYNOTE 522: Controlled study of neoadjuvant and adjuvant treatment of patients with high risk early stage TNBC: The efficacy of Pembrolizumab (KEYTRUDA) in combination with carboplatin and paclitaxel followed by doxorubicin or epirubicin and cyclophosphamide, given as a neoadjuvant treatment and continued as monotherapy adjuvant treatment was investigated in Study KEYNOTE 522, a randomized, double-blind, multicenter, placebo-controlled study. The key eligibility criteria for this study were newly diagnosed previously untreated high-risk-early stage TNBC (tumor size >1 cm but ≤2 cm in diameter with nodal involvement or tumor size >2 cm in diameter regardless of nodal involvement), regardless of tumor PD-L1 expression. Patients with active autoimmune disease that required systemic therapy within 2 years of treatment or a medical condition that required immunosuppression were ineligible for the study. Randomization was stratified by nodal status (positive vs. negative), tumor size (T1/T2 vs. T3/T4), and choice of carboplatin (dosed every 3 weeks vs. weekly).
Patients were randomized (2:1) to one of the following treatment arms; all study medications were administered via intravenous infusion.
Arm 1: Four cycles of preoperative Pembrolizumab (KEYTRUDA) 200 mg every 3 weeks on Day 1 of cycles 1-4 of treatment regimen in combination with: Carboplatin: AUC 5 mg/mL/min every 3 weeks on Day 1 of cycles 1-4 of treatment regimen or AUC 1.5 mg/mL/min every week on Day 1, 8, and 15 of cycles 1-4 of treatment regimen and; Paclitaxel 80 mg/m
2 every week on Day 1, 8, and 15 of cycles 1-4 of treatment regimen.
Followed by four additional cycles of preoperative Pembrolizumab (KEYTRUDA) 200 mg every 3 weeks on Day 1 of cycles 5-8 of treatment regimen in combination with: Doxorubicin 60 mg/m
2 or epirubicin 90 mg/m
2 every 3 weeks on Day 1 of cycles 5-8 of treatment regimen and; Cyclophosphamide 600 mg/m
2 every 3 weeks on Day 1 of cycles 5-8 of treatment regimen.
Following surgery, 9 cycles of Pembrolizumab (KEYTRUDA) 200 mg every 3 weeks were administered.
Arm 2: Four cycles of preoperative placebo every 3 weeks on Day 1 of cycles 1-4 of treatment regimen in combination with: Carboplatin: AUC 5 mg/mL/min every 3 weeks on Day 1 of cycles 1-4 of treatment regimen or AUC 1.5 mg/mL/min every week on Day 1, 8, and 15 of cycles 1-4 of treatment regimen and; Paclitaxel 80 mg/m
2 every week on Day 1, 8, and 15 of cycles 1-4 of treatment regimen.
Followed by four additional cycles of preoperative placebo every 3 weeks on Day 1 of cycles 5-8 of treatment regimen in combination with: Doxorubicin 60 mg/m
2 or epirubicin 90 mg/m
2 every 3 weeks on Day 1 of cycles 5-8 of treatment regimen and; Cyclophosphamide 600 mg/m
2 every 3 weeks on Day 1 of cycles 5-8 of treatment regimen.
Following surgery, 9 cycles of placebo every 3 weeks were administered.
Treatment with Pembrolizumab (KEYTRUDA) or placebo continued until completion of the treatment (17 cycles), disease progression that precludes definitive surgery, disease recurrence in the adjuvant phase, or unacceptable toxicity.
The major efficacy outcome measures were pathological complete response (pCR) rate and event free survival (EFS). pCR was defined as absence of invasive cancer in the breast and lymph nodes (ypT0/Tis ypN0) and was assessed by the blinded local pathologist at the time of definitive surgery. EFS was defined as the time from randomization to the first occurrence of any of the following events: progression of disease that precludes definitive surgery, local or distant recurrence, second primary malignancy, or death due to any cause. An additional efficacy outcome measure was OS.
A total of 1174 patients were randomized: 784 patients to the Pembrolizumab (KEYTRUDA) arm and 390 patients to the placebo arm. The study population characteristics were: median age of 49 years (range: 22 to 80), 11% age 65 or older; 99.9% female; 64% White, 20% Asian, 5% Black, and 2% American Indian or Alaska Native; 87% ECOG PS of 0 and 13% ECOG PS of 1; 56% were premenopausal status and 44% were post-menopausal status; 7% were primary Tumor 1 (T1), 68% T2, 19% T3, and 7% T4; 49% were nodal involvement 0 (N0), 40% N1, 11% N2, and 0.2% N3; 75% of patients were overall stage II and 25% were stage III.
The trial demonstrated a statistically significant improvement in pCR and EFS at a pre-specified analysis for patients randomized to Pembrolizumab (KEYTRUDA) in combination with chemotherapy followed by Pembrolizumab (KEYTRUDA) monotherapy compared with patients randomized to placebo in combination with chemotherapy followed by placebo alone. At the time of EFS analysis, OS results were not yet mature (45% of the required events for final analysis). However, the data showed an improvement in OS that favored the Pembrolizumab (KEYTRUDA) arm over the placebo arm. At a pre specified interim analysis, the median follow-up time for 784 patients treated with Pembrolizumab (KEYTRUDA) was 37.8 months (range: 2.7-48 months). Efficacy results are summarized in Table 41 and Figure 35. (See Table 41 and Figure 35.)
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
The impact of the addition of Pembrolizumab (KEYTRUDA) to chemotherapy on health-related quality of life was assessed using the EORTC QLQ-C30. Over 21 weeks of follow up, the Least Square (LS) mean score change in the QLQ-C30 global health status/QoL scale was -11.24 (-12.82, -9.66) in patients treated with Pembrolizumab (KEYTRUDA) in combination with chemotherapy and -10.20 (-12.30, -8.10) in patients treated with placebo in combination with chemotherapy as neoadjuvant treatment [difference in LS means: -1.04; 95% CI: -3.46, 1.38]. Over 24 weeks of follow up, the LS mean score change in the global health status/QoL scale was 2.47 (1.05, 3.88) in patients treated with Pembrolizumab (KEYTRUDA) and 2.88 (1.05, 4.71) in patients treated with placebo as adjuvant treatment [difference in LS means: -0.41 (-2.60, 1.77)].
KEYNOTE 355: Controlled study of combination therapy in patients with locally recurrent unresectable or metastatic TNBC The efficacy of Pembrolizumab (KEYTRUDA) in combination with paclitaxel, nab-paclitaxel, or gemcitabine and carboplatin was investigated in Study KEYNOTE-355, a randomized, double-blind, multicenter, placebo-controlled study. The key eligibility criteria for this study were locally recurrent unresectable or metastatic TNBC, regardless of tumor PD-L1 expression, and which had not been previously treated with chemotherapy. Patients with active autoimmune disease that required systemic therapy within 2 years of treatment or a medical condition that required immunosuppression were ineligible for the study. Randomization was stratified by chemotherapy treatment (paclitaxel or nab-paclitaxel vs. gemcitabine and carboplatin), tumor PD--L1 expression (CPS ≥1 vs. CPS <1) based on the PD-L1 IHC 22C3 pharmDx kit, and prior treatment with the same class of chemotherapy in the neoadjuvant setting (yes vs. no).
Patients were randomized (2:1) to one of the following treatment arms; all study medications were administered via intravenous infusion.
Pembrolizumab (KEYTRUDA) 200 mg on Day 1 every 3 weeks in combination with nab-paclitaxel 100 mg/m
2 on Days 1, 8 and 15 every 28 days, or paclitaxel 90 mg/m
2 on Days 1, 8, and 15 every 28 days, or gemcitabine 1000 mg/m
2 and carboplatin AUC 2 mg/mL/min on Days 1 and 8 every 21 days.
Placebo on Day 1 every 3 weeks in combination with nab-paclitaxel 100 mg/m
2 on Days 1, 8 and 15 every 28 days, or paclitaxel 90 mg/m
2 on Days 1, 8, and 15 every 28 days, or gemcitabine 1000 mg/m
2 and carboplatin AUC 2 mg/mL/min on Days 1 and 8 every 21 days.
Treatment with Pembrolizumab (KEYTRUDA) or placebo continued until RECIST 1.1-defined progression of disease as determined by the investigator, unacceptable toxicity, or a maximum of 24 months. Administration of Pembrolizumab (KEYTRUDA) was permitted beyond RECIST-defined disease progression if the patient was clinically stable and considered to be deriving clinical benefit by the investigator. Assessment of tumor status was performed at Weeks 8, 16, and 24, then every 9 weeks for the first year, and every 12 weeks thereafter.
The major efficacy outcome measure was PFS in patients with tumor PD-L1 expression CPS ≥10, as assessed by BICR using RECIST 1.1. Additional efficacy outcome measures were ORR, DOR, and DCR (stable disease for at least 24 weeks, or complete response, or partial response) in patients with tumor PD-L1 expression CPS ≥10 as assessed by BICR using RECIST 1.1.
A total of 847 patients were randomized: 566 patients to the Pembrolizumab (KEYTRUDA) arm and 281 patients to the placebo arm. The study population characteristics were: median age of 53 years (range: 22 to 85), 21% age 65 or older; 100% female; 68% White, 21% Asian, and 4% Black; 60% ECOG PS of 0 and 40% ECOG PS of 1; and 68% were post-menopausal status. Seventy five percent of the patients had tumor PD-L1 expression defined as CPS ≥1 and 38% had tumor PD--L1 expression CPS ≥10.
In KEYNOTE 355, there was a statistically significant improvement in PFS in patients with tumor PD--L1 expression CPS ≥10 randomized to Pembrolizumab (KEYTRUDA) in combination with paclitaxel, nab-paclitaxel, or gemcitabine and carboplatin compared with patients randomized to placebo in combination with paclitaxel, nab-paclitaxel, or gemcitabine and carboplatin. The trial also demonstrated a clinically meaningful improvement in ORR and DoR.
Efficacy results are summarized in Table 42 and Figure 36. (See Table 42 and Figure 36.)
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
The impact of the addition of Pembrolizumab (KEYTRUDA) to chemotherapy on patient-reported outcomes were assessed using the EORTC QLQ-C30, EORTC QLQ-BR23 and EuroQol EQ 5D. Results from each measure showed that the addition of Pembrolizumab (KEYTRUDA) to chemotherapy did not result in a decrease in health related quality of life through 15 weeks of follow up.
Immunogenicity: In clinical studies in patients treated with pembrolizumab at a dose of 2 mg/kg every three weeks, 200 mg every three weeks, or 10 mg/kg every two or three weeks, 36 (1.8%) of 2034 evaluable patients tested positive for treatment-emergent antibodies against pembrolizumab of which 9 (0.4%) patients had neutralizing antibodies against pembrolizumab. There was no evidence of an altered pharmacokinetic or safety profile with anti-pembrolizumab binding or neutralizing antibody development.
Pharmacokinetics: The pharmacokinetics of pembrolizumab was studied in 2993 patients with various cancers who received doses in the range of 1 to 10 mg/kg every 2 weeks, 2 to 10 mg/kg every 3 weeks, or 200 mg every 3 weeks. There are no clinically meaningful differences in pharmacokinetics of pembrolizumab across indications.
Absorption: Pembrolizumab (KEYTRUDA) is dosed via the IV route and therefore is immediately and completely bioavailable.
Distribution: Consistent with a limited extravascular distribution, the volume of distribution of pembrolizumab at steady state is small (6.0 L; coefficient of variation [CV]: 20%). As expected for an antibody, pembrolizumab does not bind to plasma proteins in a specific manner.
Metabolism: Pembrolizumab is catabolized through non-specific pathways; metabolism does not contribute to its clearance.
Elimination: Pembrolizumab clearance (CV%) is approximately 23% lower [geometric mean, 195 mL/day (40%)] after achieving maximal change at steady state compared with the first dose (252 mL/day [CV%: 37%]); this decrease in clearance with time is not considered clinically important. The geometric mean value (CV%) for the terminal half-life (t½) is 22 days (32%).
Steady-state concentrations of pembrolizumab were reached by 16 weeks of repeated dosing with an every 3-week regimen and the systemic accumulation was 2.1-fold. The peak concentration (C
max), trough concentration (C
min), and area under the plasma concentration versus time curve at steady state (AUC
ss) of pembrolizumab increased dose proportionally in the dose range of 2 to 10 mg/kg every 3 weeks.
Special Populations: The effects of various covariates on the pharmacokinetics of pembrolizumab were assessed in population pharmacokinetic analyses. The following factors had no clinically important effect on the clearance of pembrolizumab: age (range 15-94 years), gender, race, mild or moderate renal impairment, mild hepatic impairment, and tumor burden. The relationship between body weight and clearance supports the use of either fixed dose or body weight-based dosing to provide adequate and similar control of exposure. Pembrolizumab concentrations with weight-based dosing at 2 mg/kg every 3 weeks in pediatric patients (2 to 17 years) are comparable to those of adults at the same dose.
Renal Impairment: The effect of renal impairment on the clearance of pembrolizumab was evaluated by population pharmacokinetic analysis in patients with mild (GFR <90 and ≥60 mL/min/1.73 m
2) or moderate (GFR <60 and ≥30 mL/min/1.73 m
2) renal impairment compared to patients with normal (GFR ≥90 mL/min/1.73 m
2) renal function. No clinically important differences in the clearance of pembrolizumab were found between patients with mild or moderate renal impairment and patients with normal renal function. Pembrolizumab (KEYTRUDA) has not been studied in patients with severe (GFR <30 and ≥15 mL/min/1.73 m
2) renal impairment. [See Renal Impairment under Dosage & Administration.]
Hepatic Impairment: The effect of hepatic impairment on the clearance of pembrolizumab was evaluated by population pharmacokinetic analysis in patients with mild hepatic impairment [total bilirubin (TB) 1.0 to 1.5 x ULN or AST >ULN as defined using the National Cancer Institute criteria of hepatic dysfunction] compared to patients with normal hepatic function (TB and AST ≤ULN). No clinically important differences in the clearance of pembrolizumab were found between patients with mild hepatic impairment and normal hepatic function. Pembrolizumab (KEYTRUDA) has not been studied in patients with moderate (TB >1.5 to 3 x ULN and any AST) or severe (TB >3 x ULN and any AST) hepatic impairment. [See Hepatic Impairment under Dosage & Administration.]
Toxicology: Animal Toxicology: Chronic Toxicity: The safety of pembrolizumab was evaluated in a 1-month and a 6-month repeat-dose toxicity study in Cynomolgus monkeys administered IV doses of 6, 40 or 200 mg/kg once a week in the 1-month study and once every two weeks in the 6-month study, followed by a 4-month treatment-free period. No findings of toxicological significance were observed and the no observed adverse effect level (NOAEL) in both studies was ≥200 mg/kg, which produced exposure multiples of 19 and 94 times the exposure in humans at doses of 10 and 2 mg/kg, respectively. The exposure multiple between the NOAEL and a human dose of 200 mg was 74.
Carcinogenesis: The carcinogenic potential of pembrolizumab has not been evaluated in long-term animal studies.
Mutagenesis: The genotoxic potential of pembrolizumab has not been evaluated.
Reproduction: Animal reproduction studies have not been conducted with Pembrolizumab (KEYTRUDA). The central function of the PD-1/PD-L1 pathway is to preserve pregnancy by maintaining immune tolerance to the fetus. Blockade of PD-L1 signaling has been shown in murine models of pregnancy to disrupt tolerance to the fetus and to result in an increase in fetal loss. These results indicate a potential risk that administration of Pembrolizumab (KEYTRUDA) during pregnancy could cause fetal harm, including increased rates of abortion or stillbirth.
Development: Developmental toxicity studies have not been conducted with pembrolizumab. There were no notable effects in the male and female reproductive organs in monkeys based on 1-month and 6-month repeat dose toxicity studies.



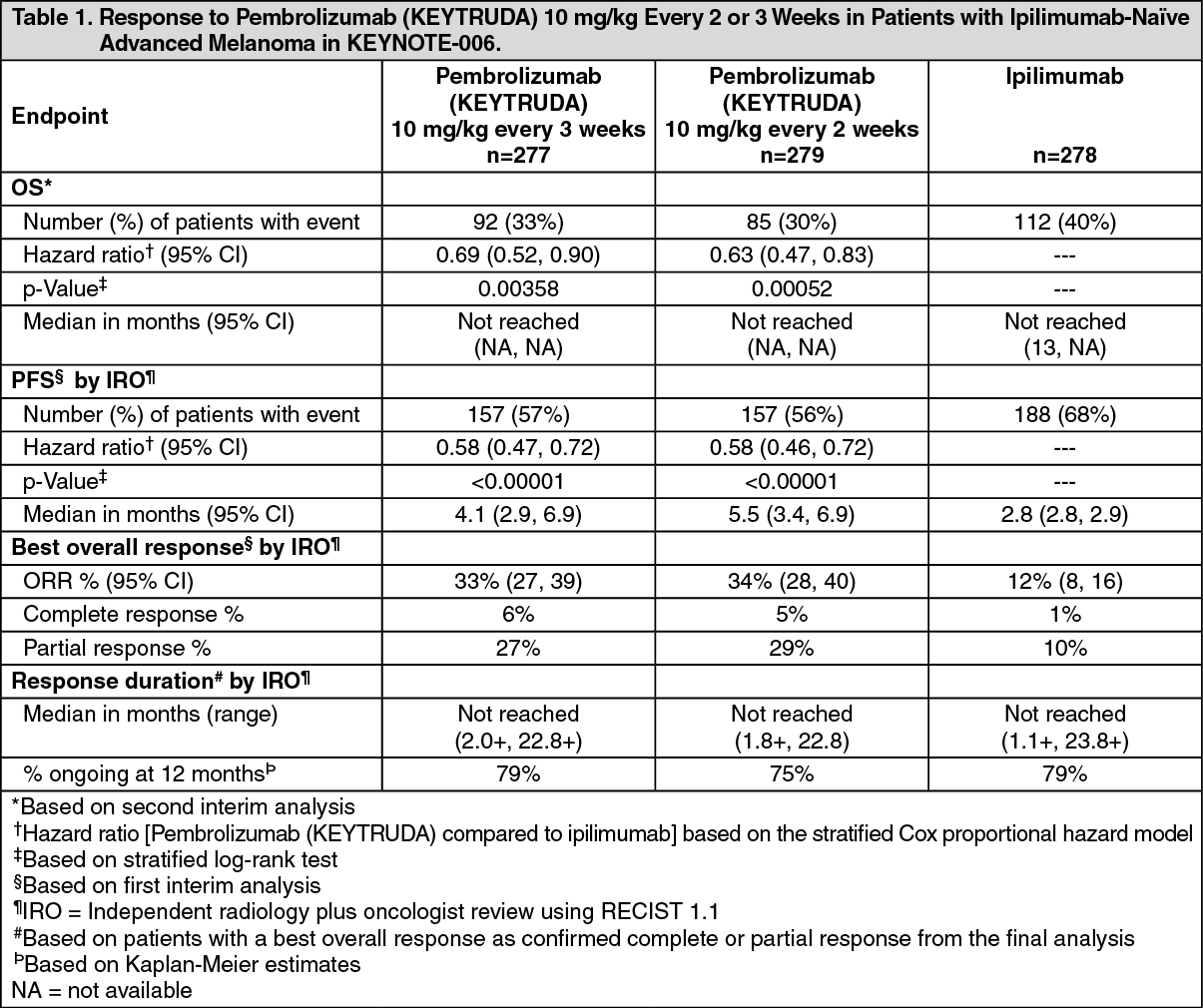 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image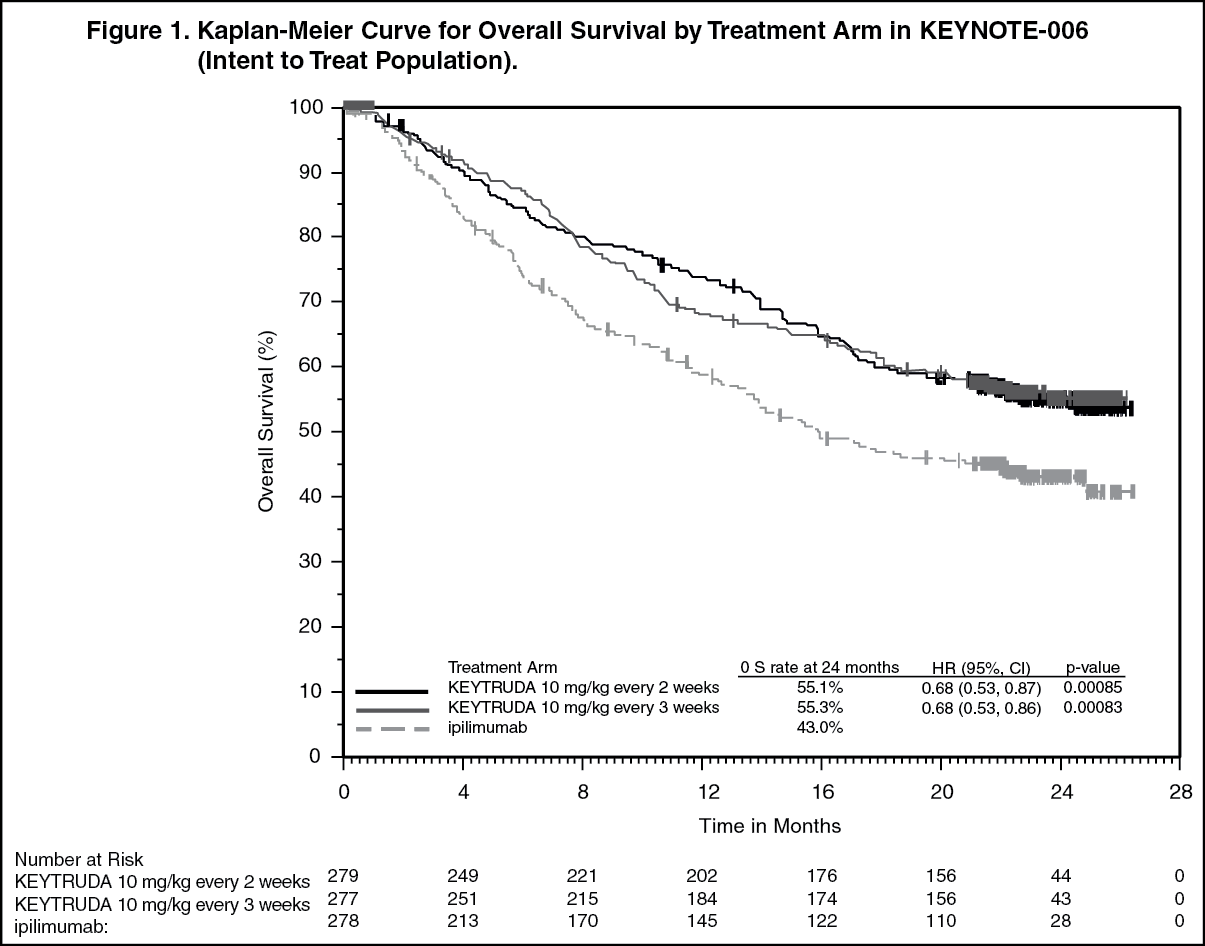 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image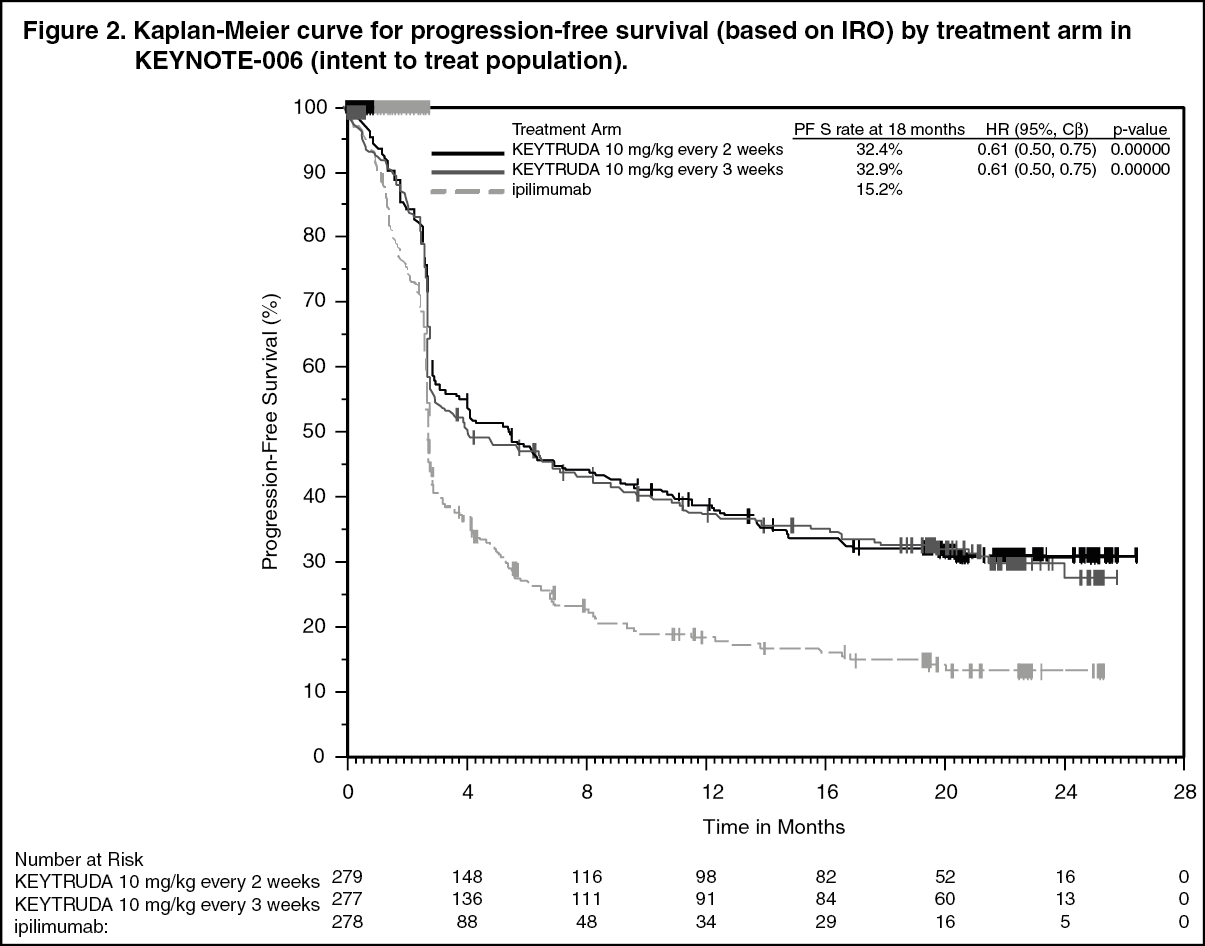 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image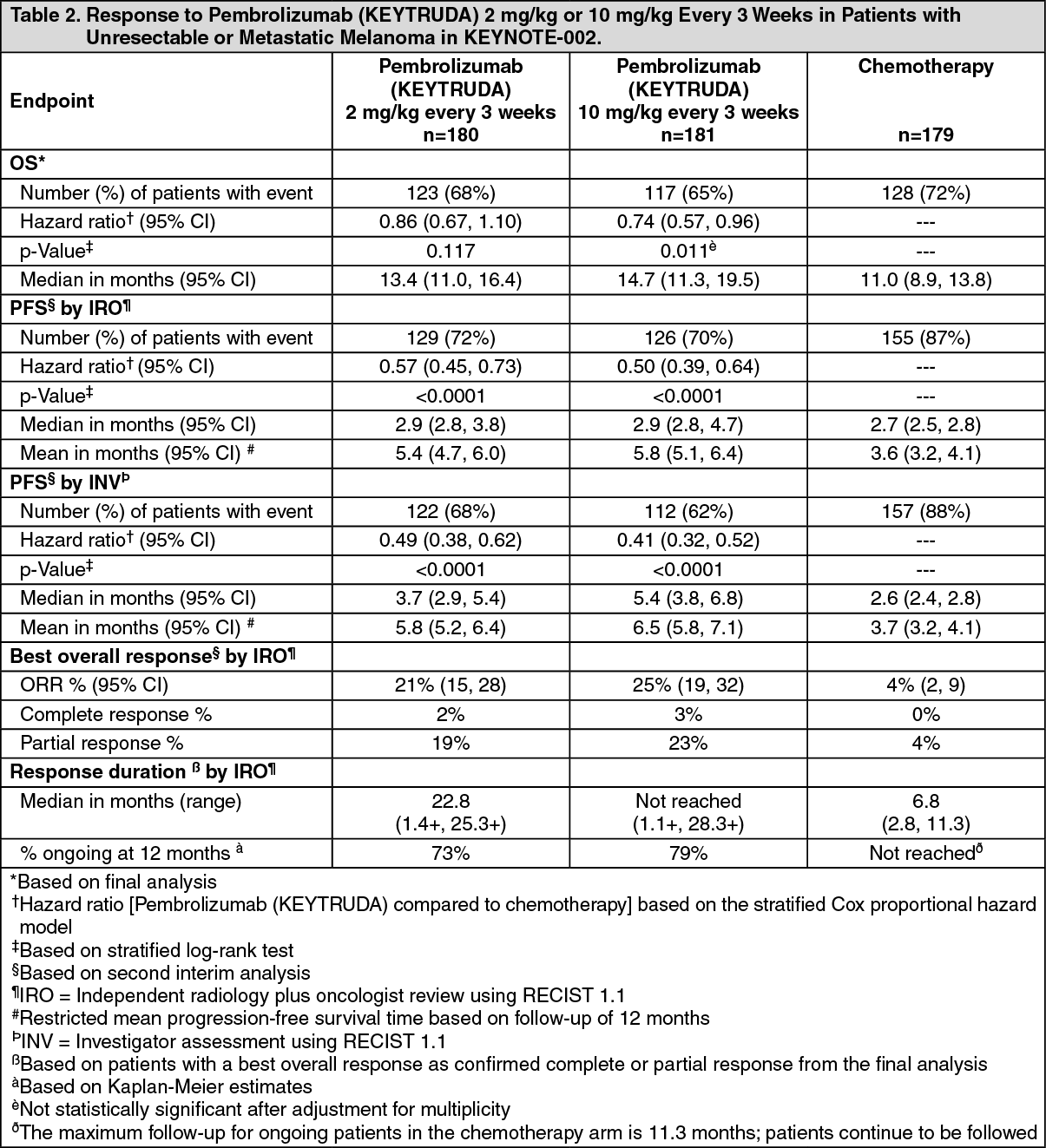 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image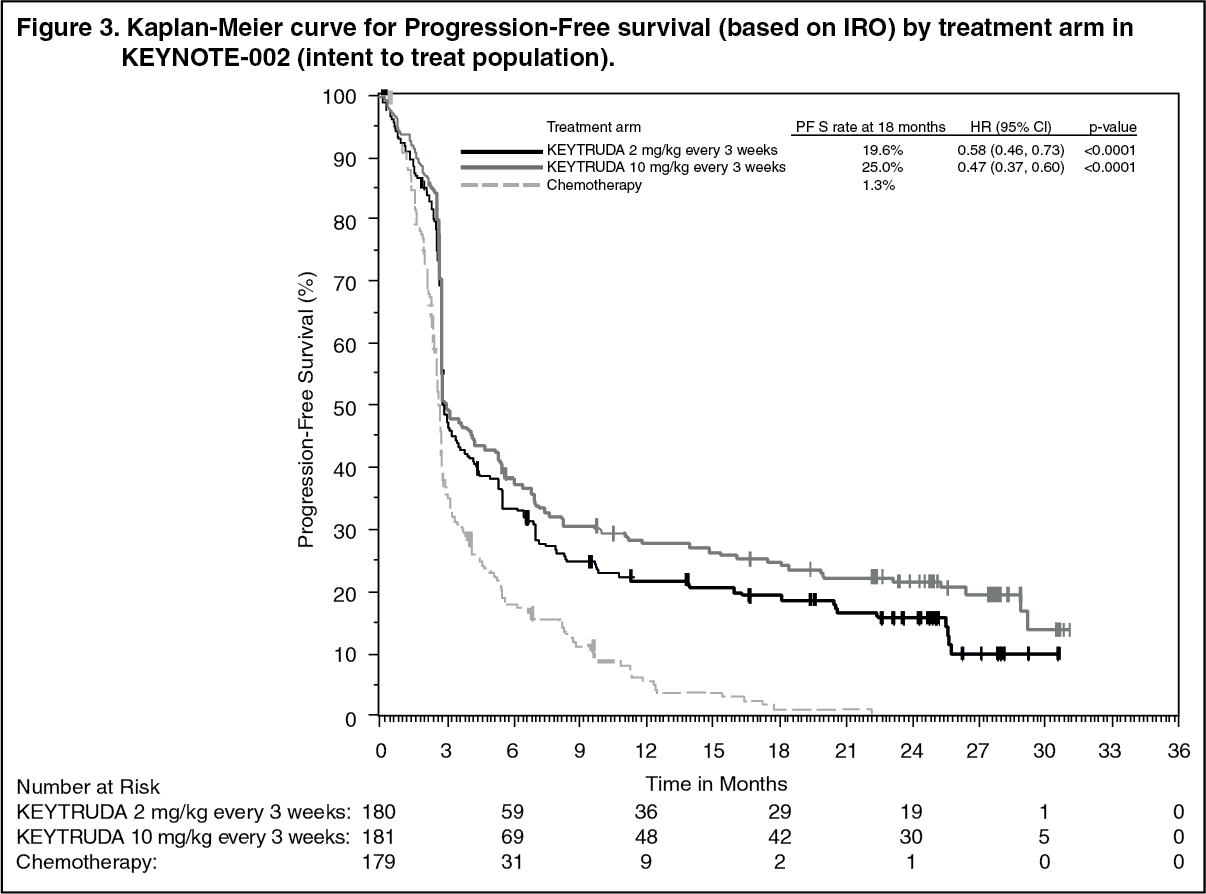 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image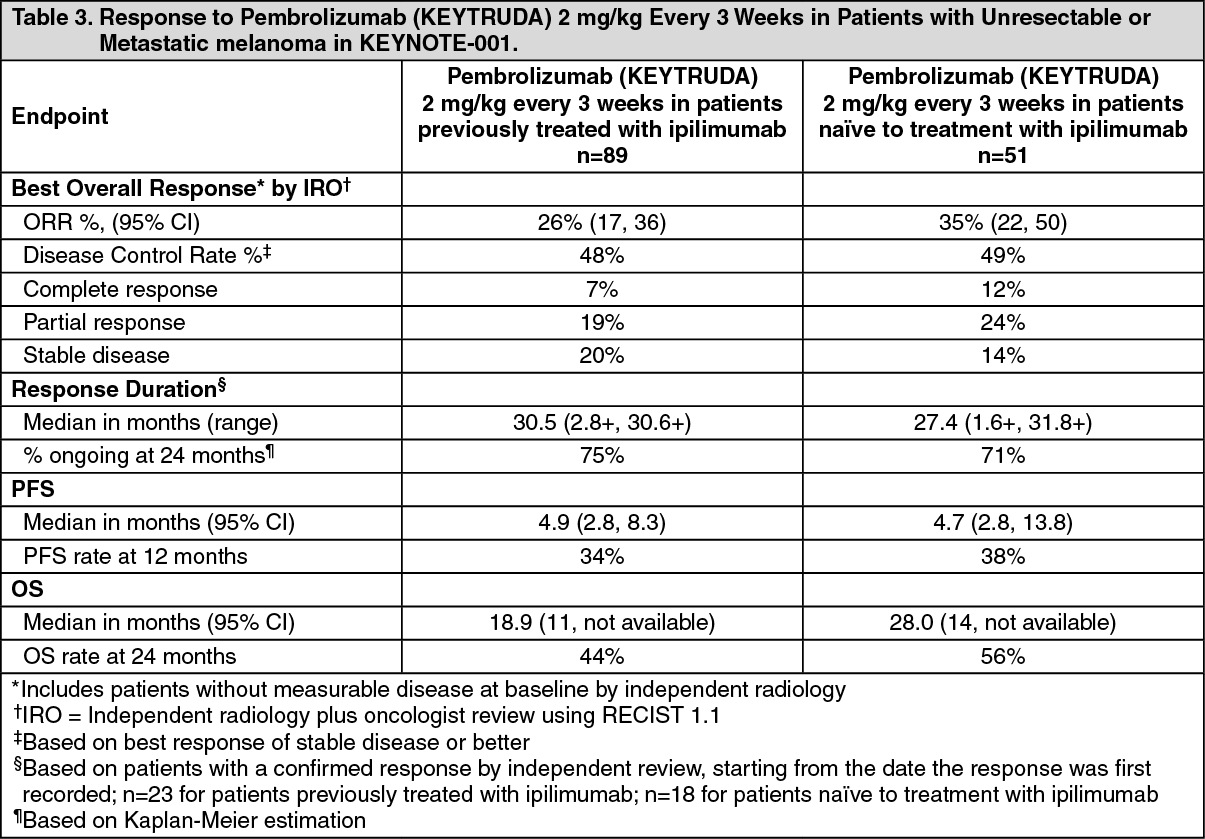 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image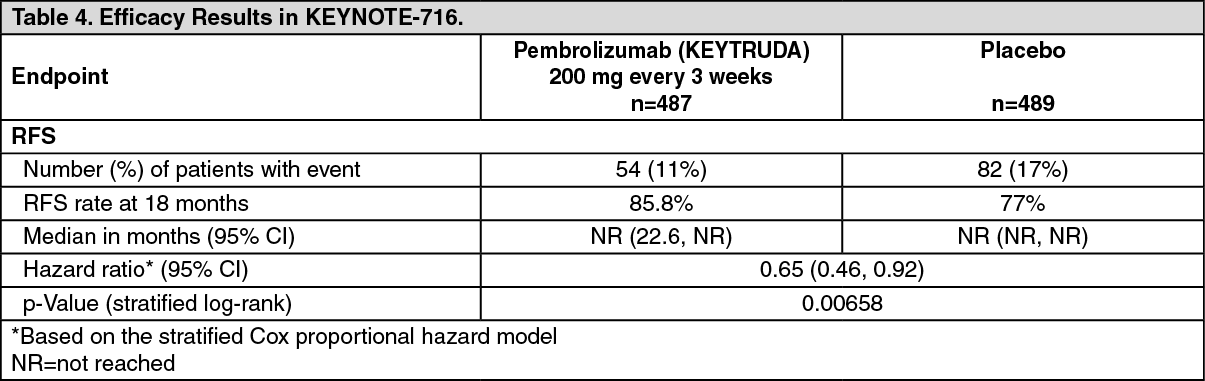 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image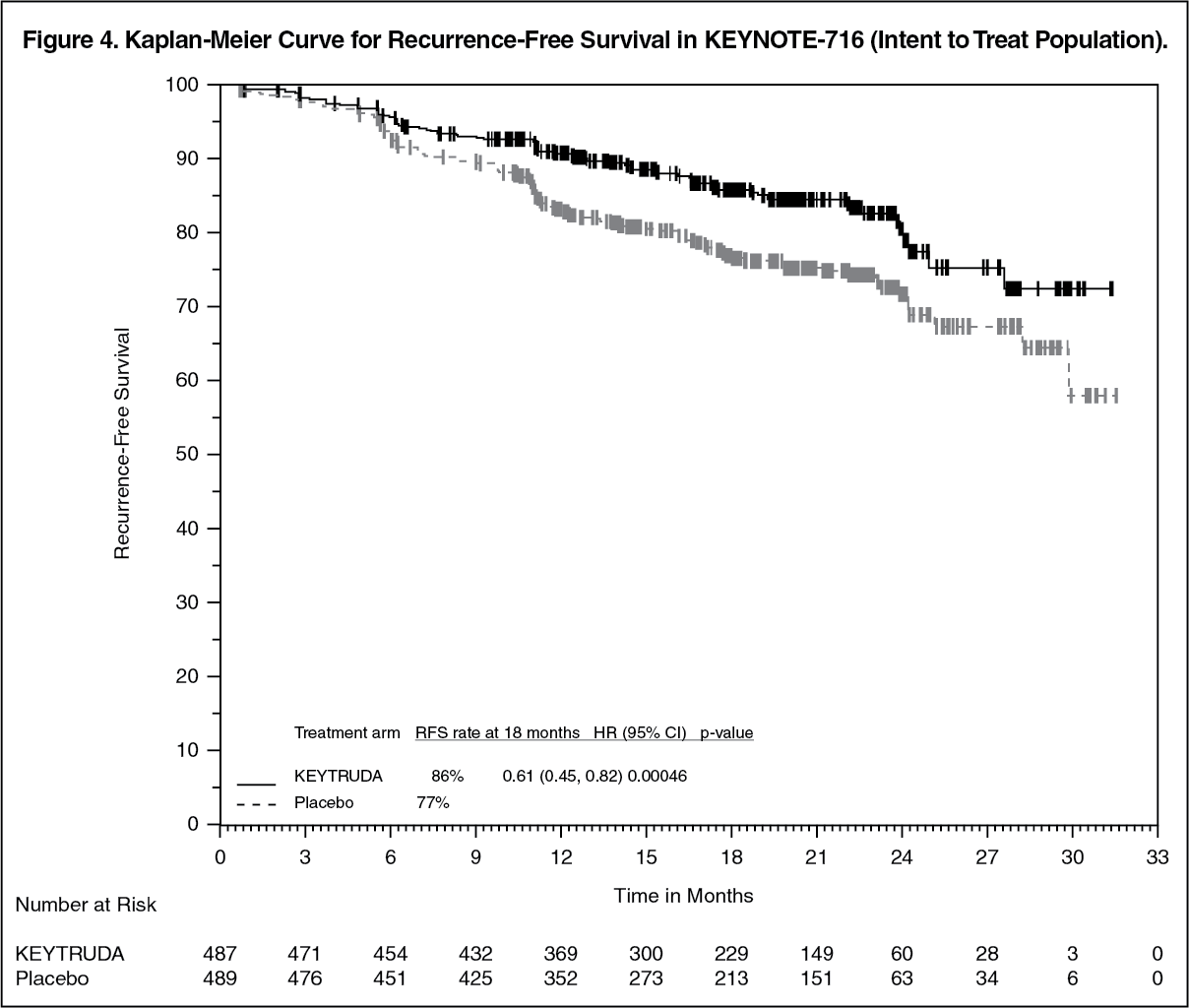 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image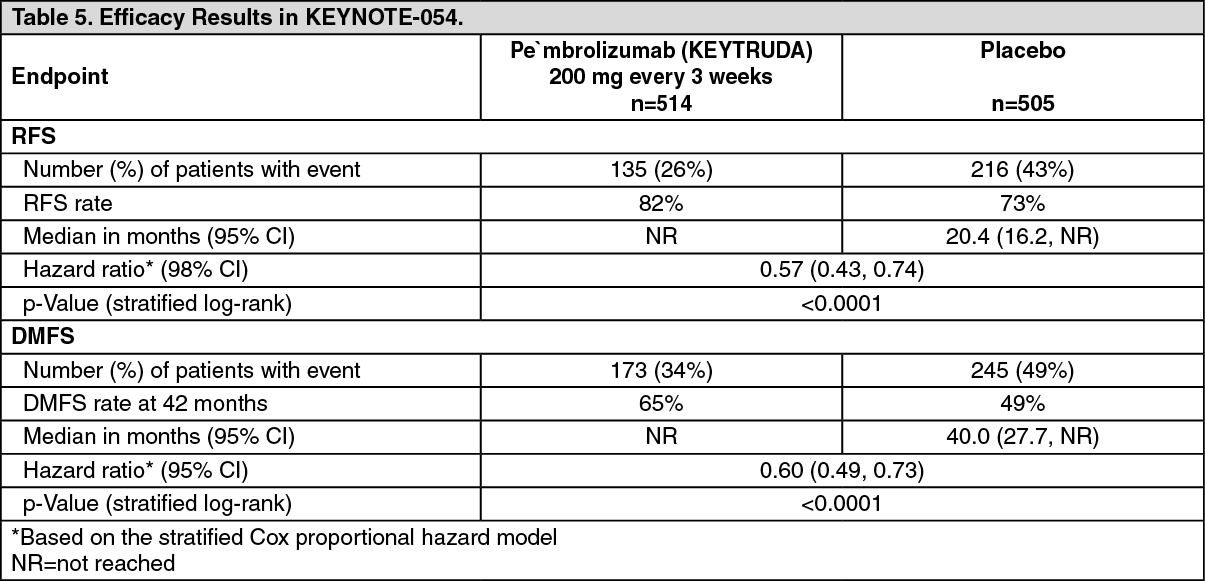 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image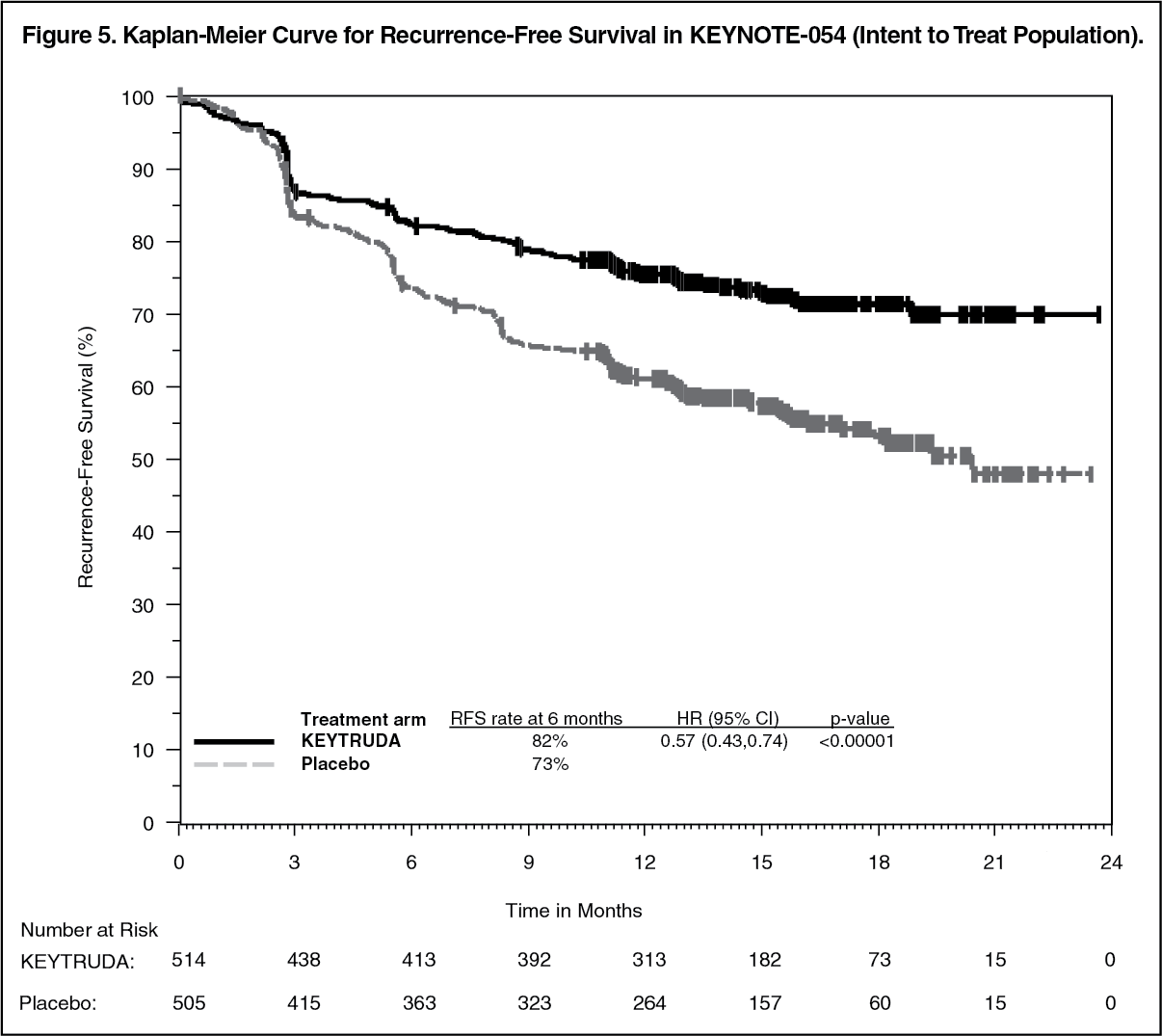 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image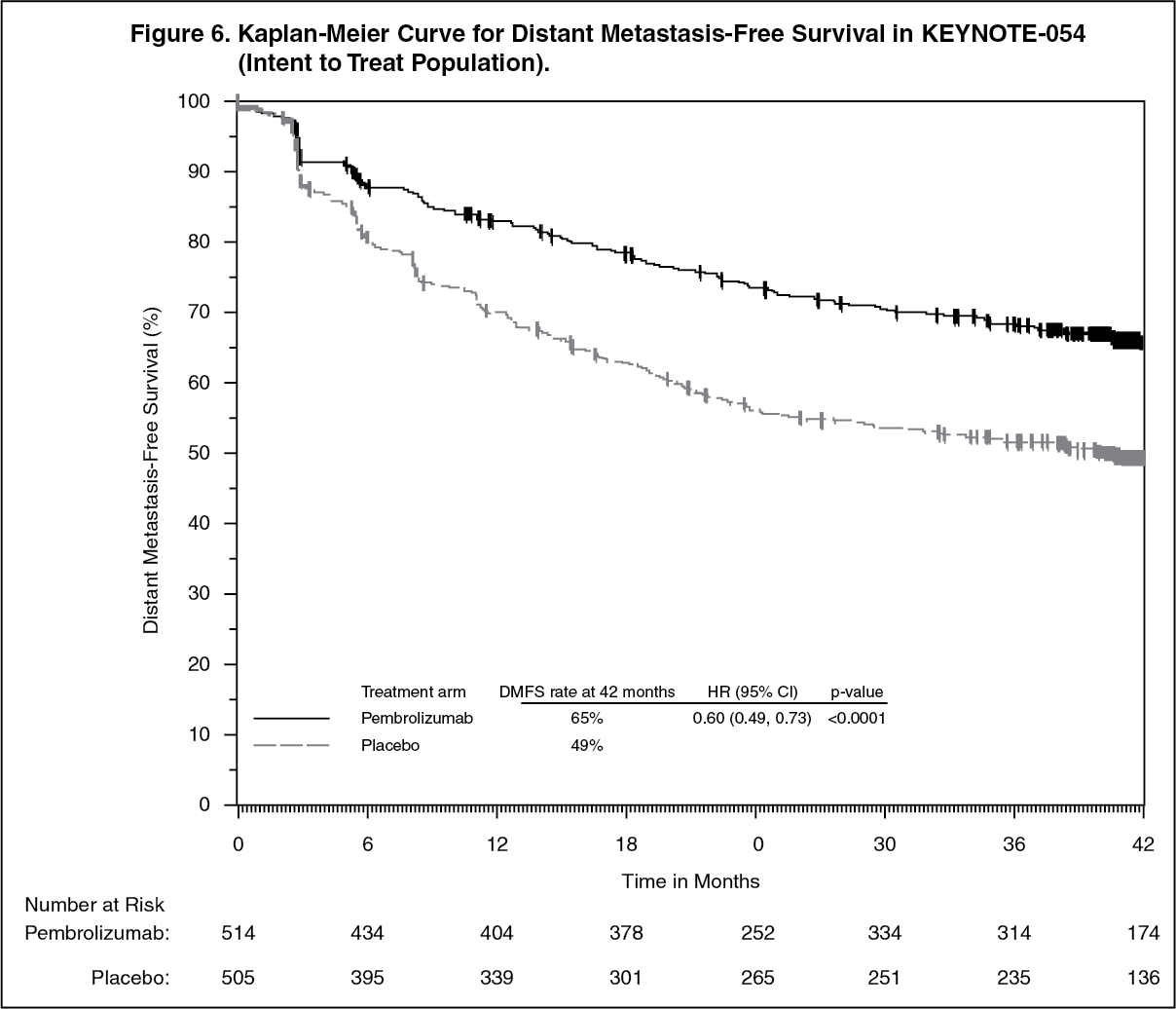 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image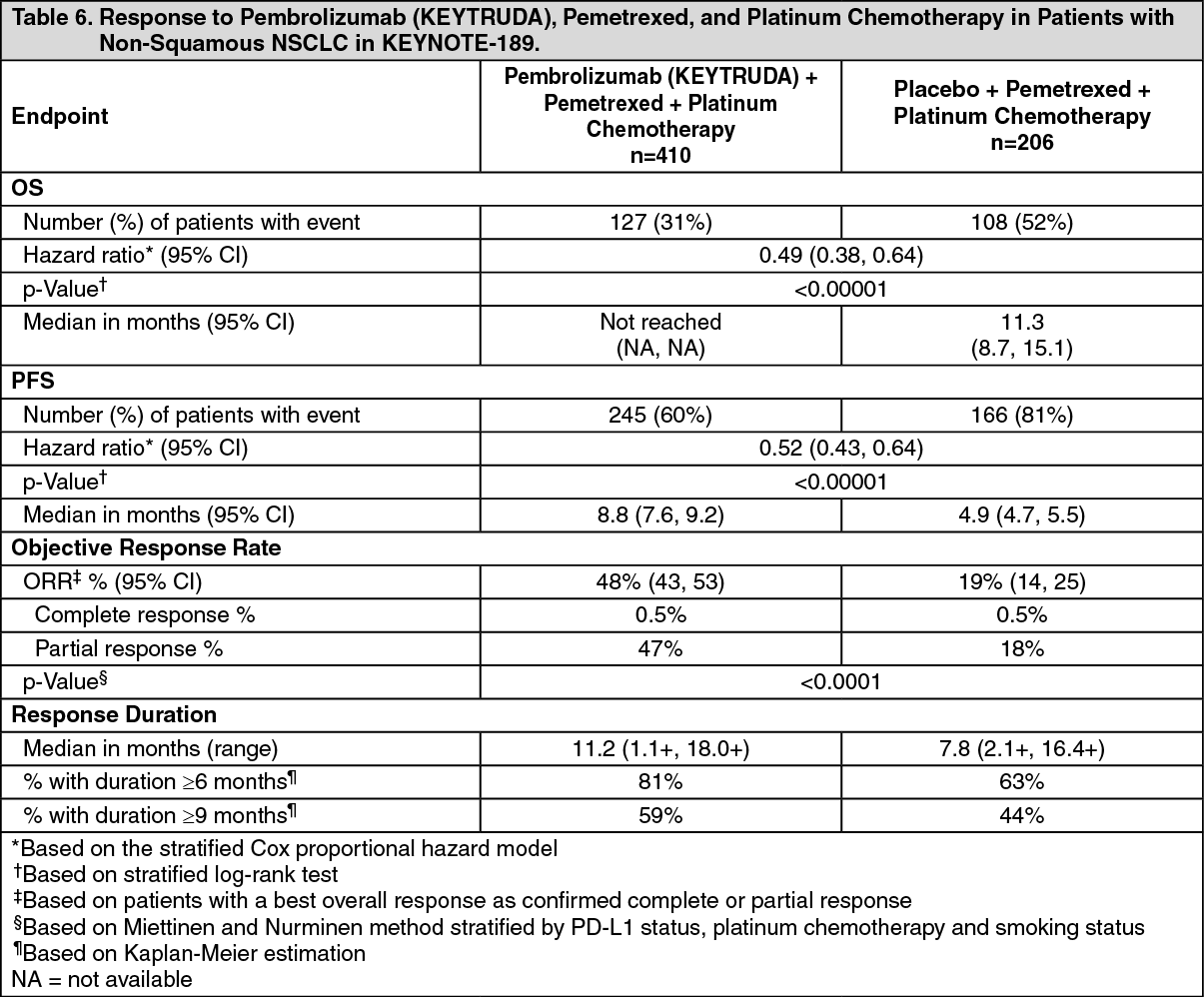 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image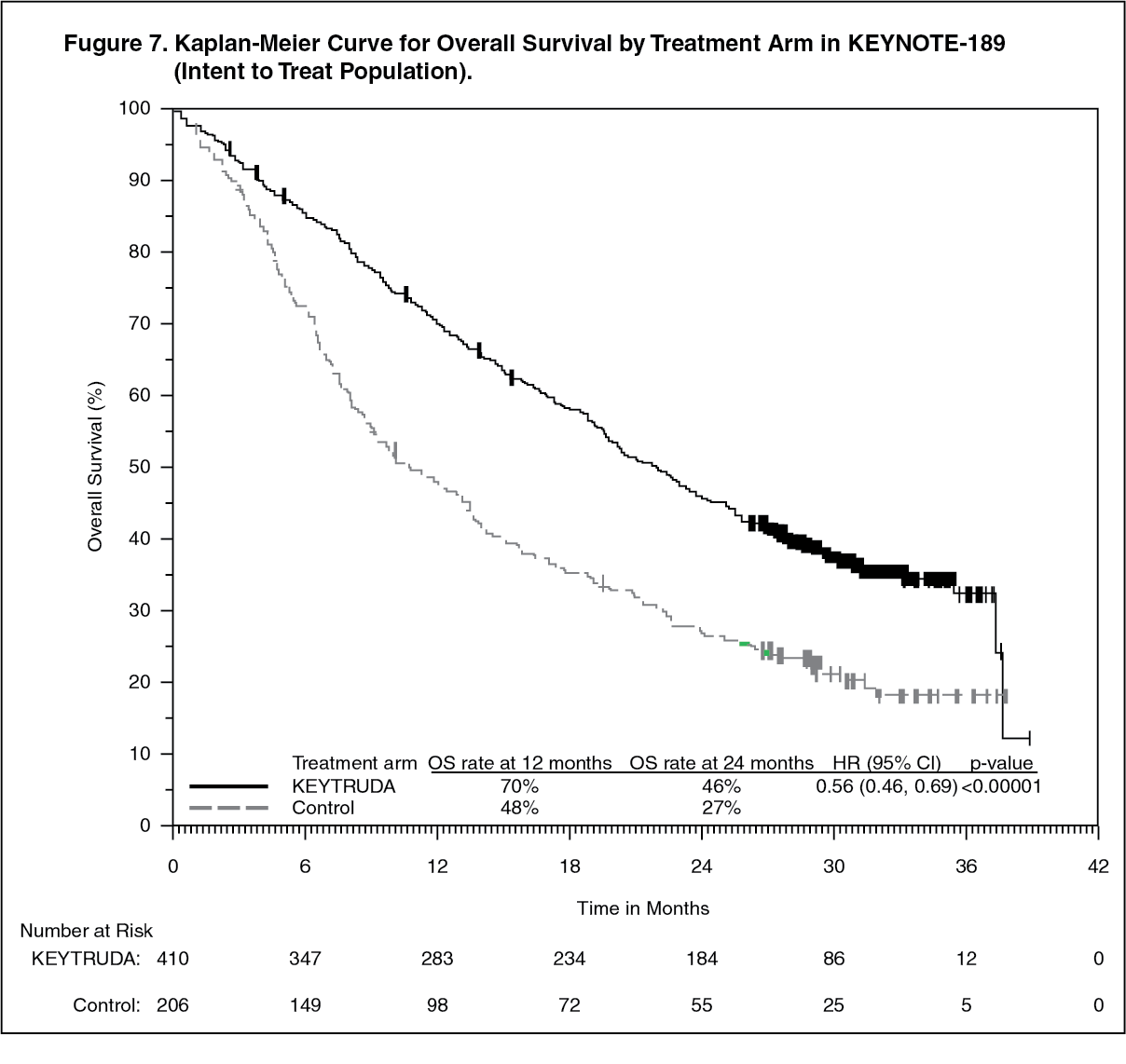 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image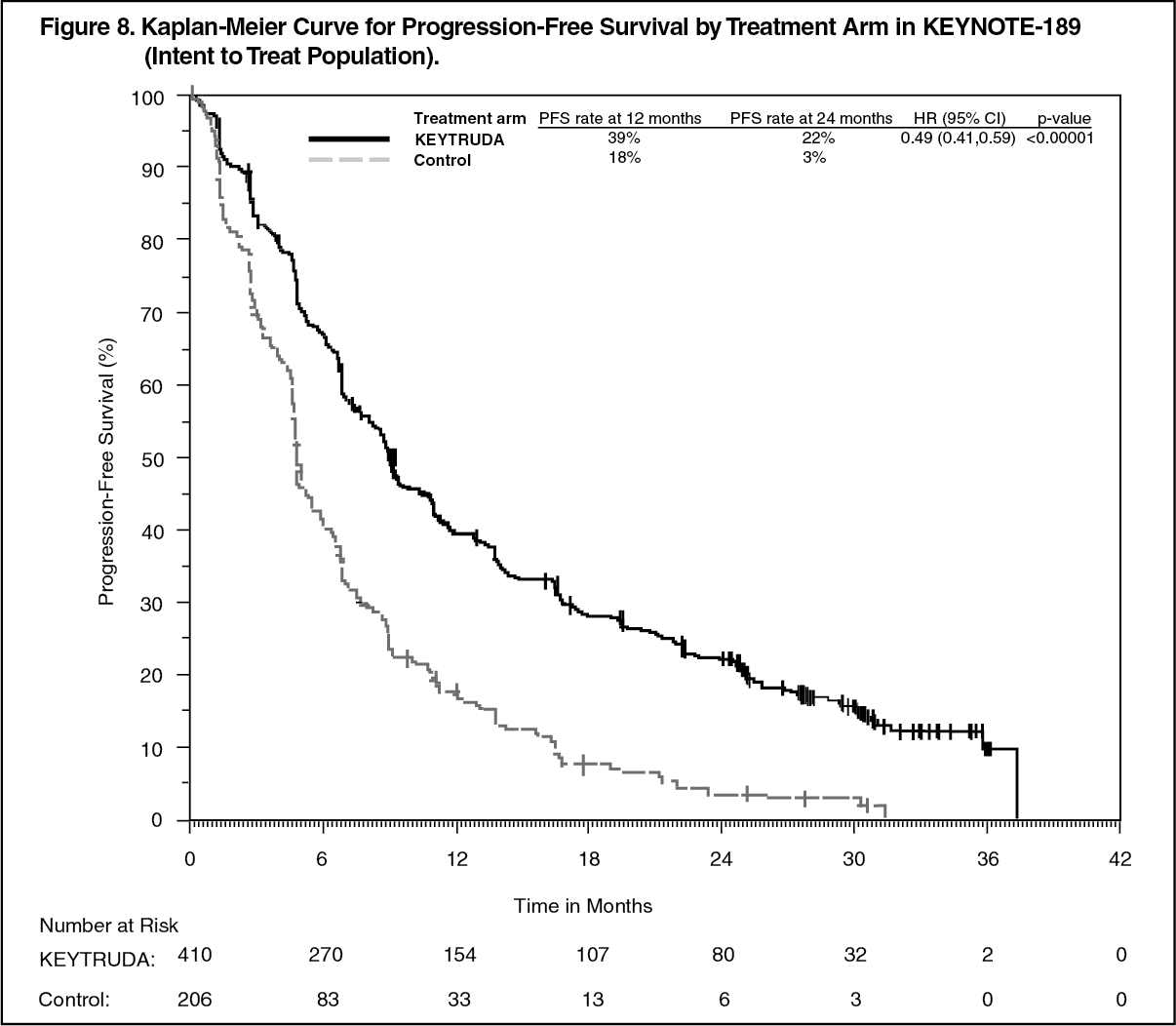 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image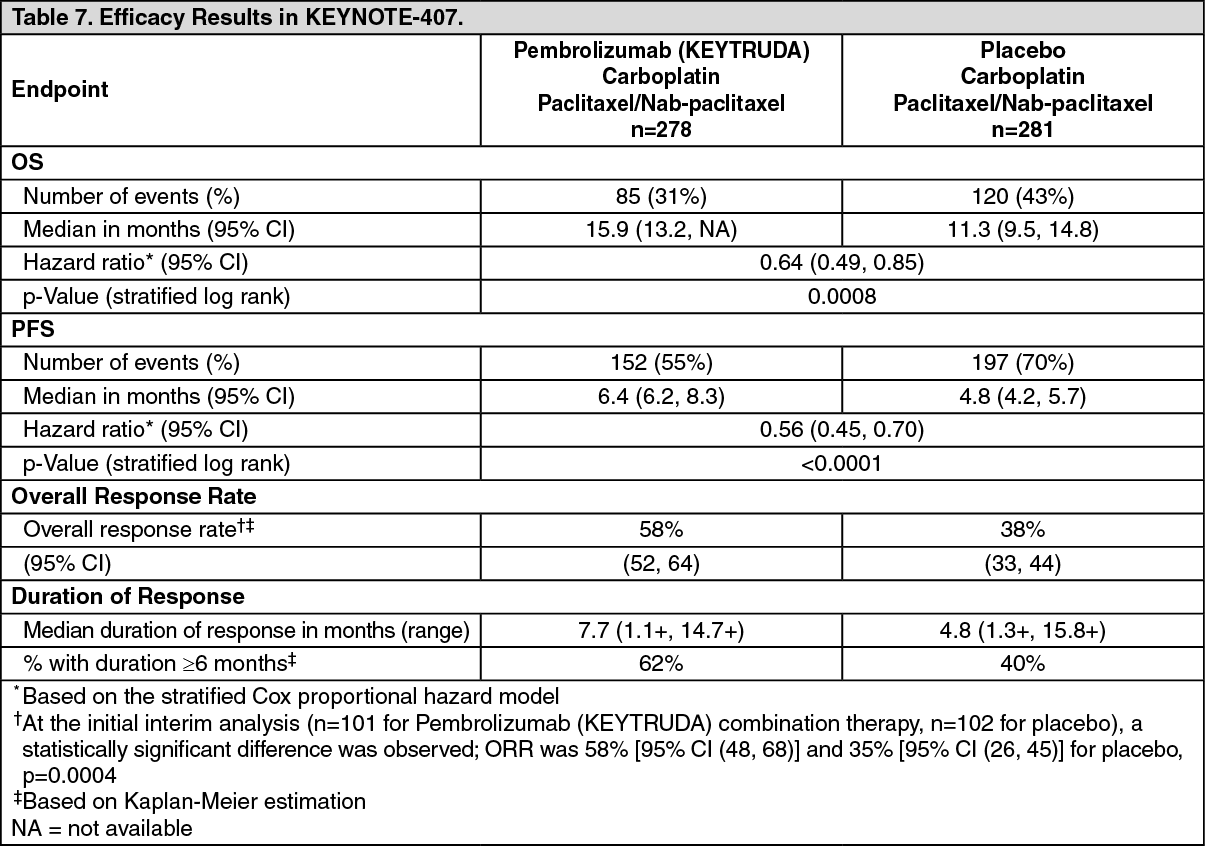 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image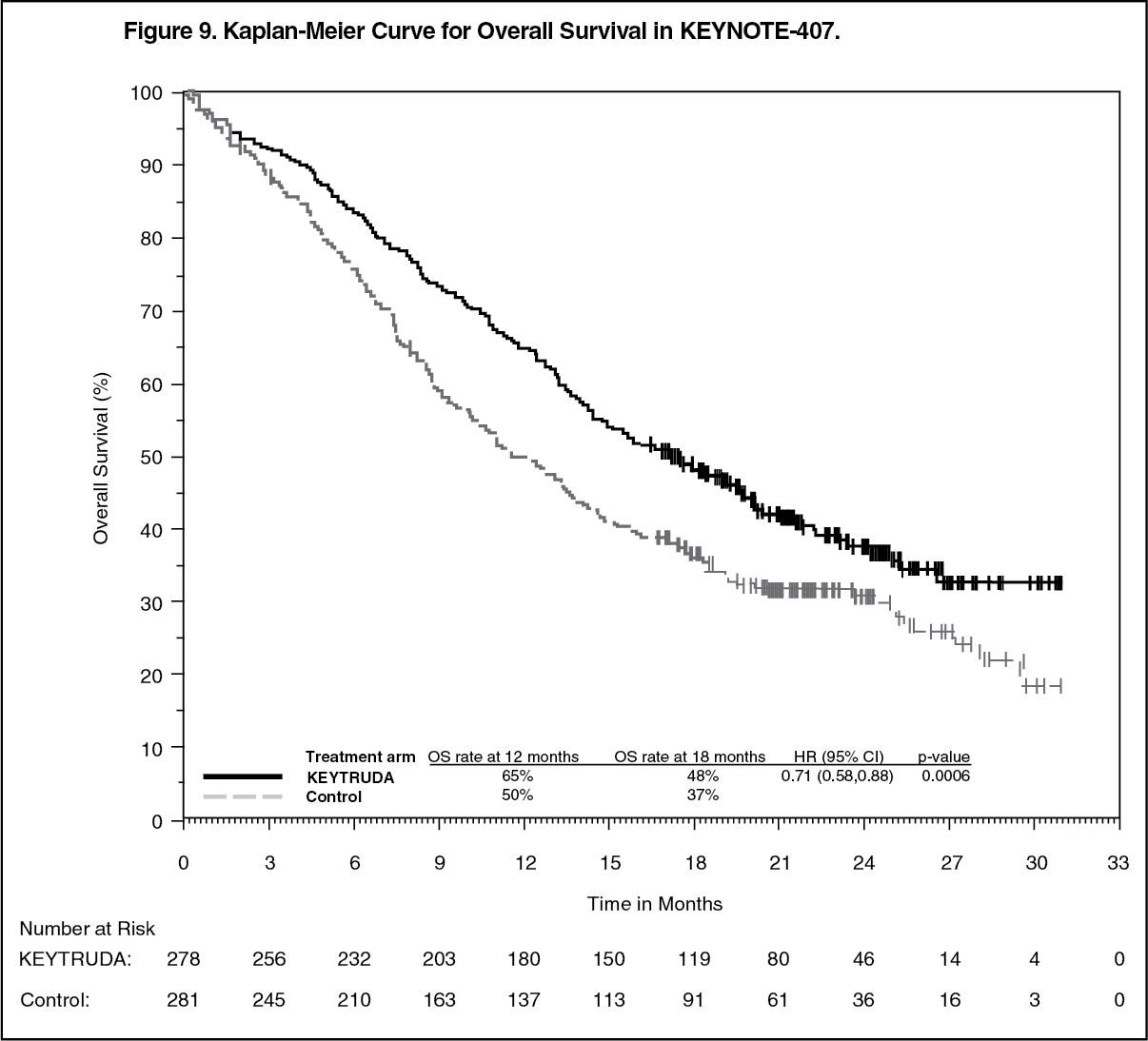 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image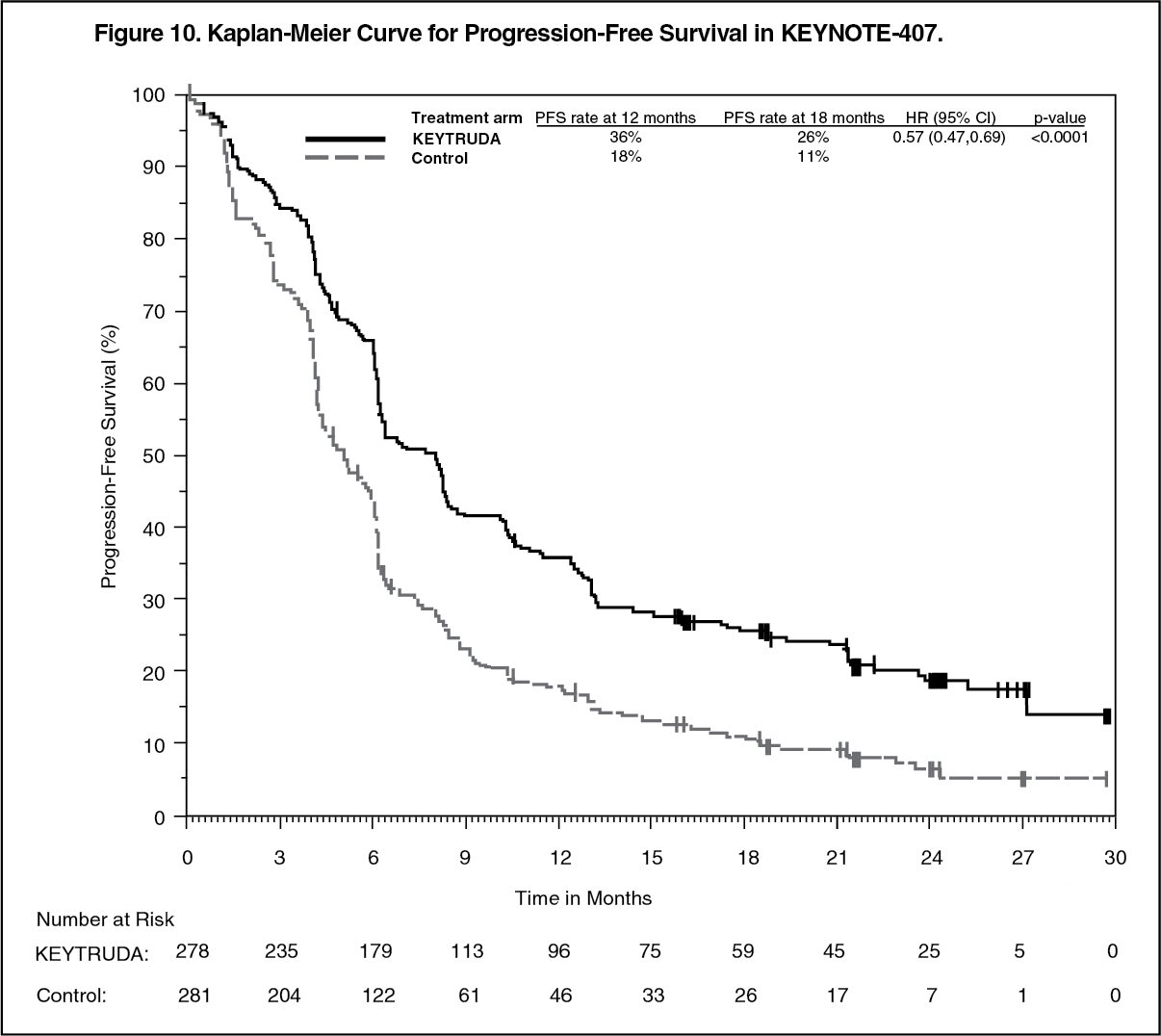 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image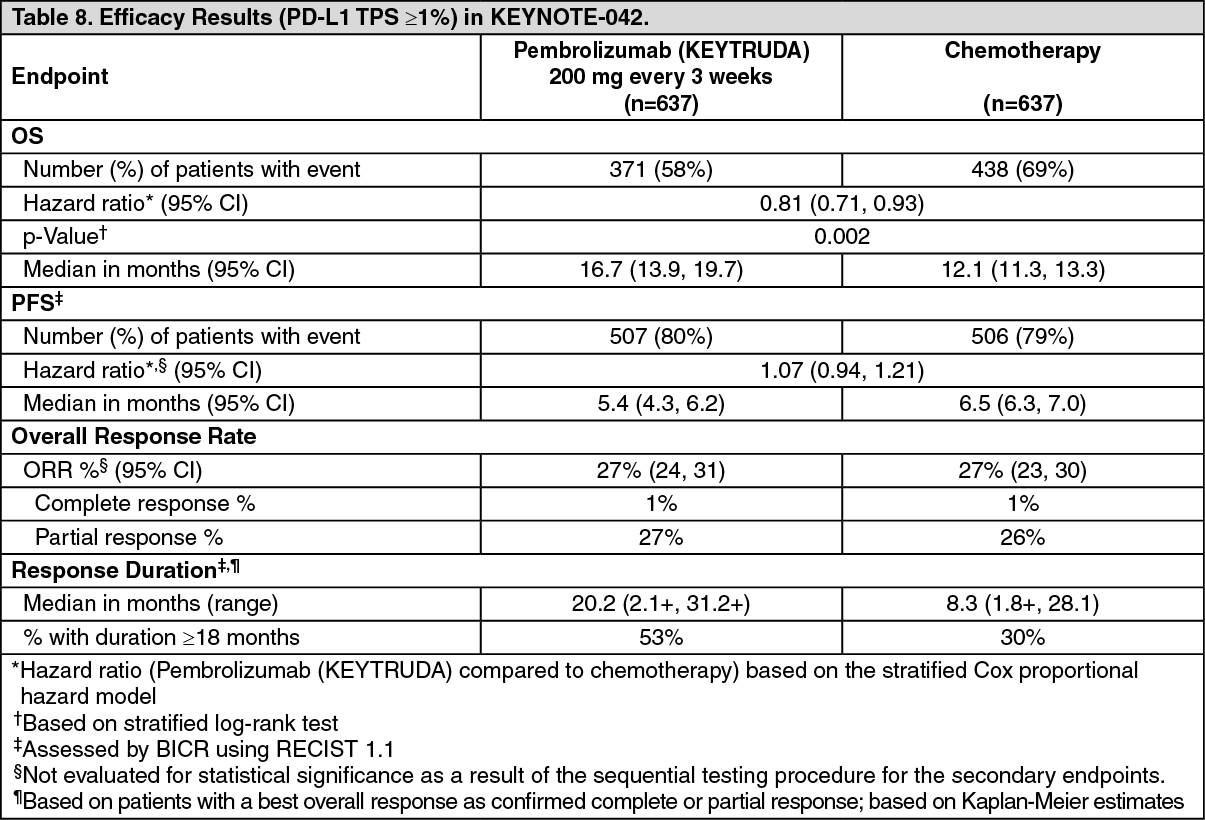 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image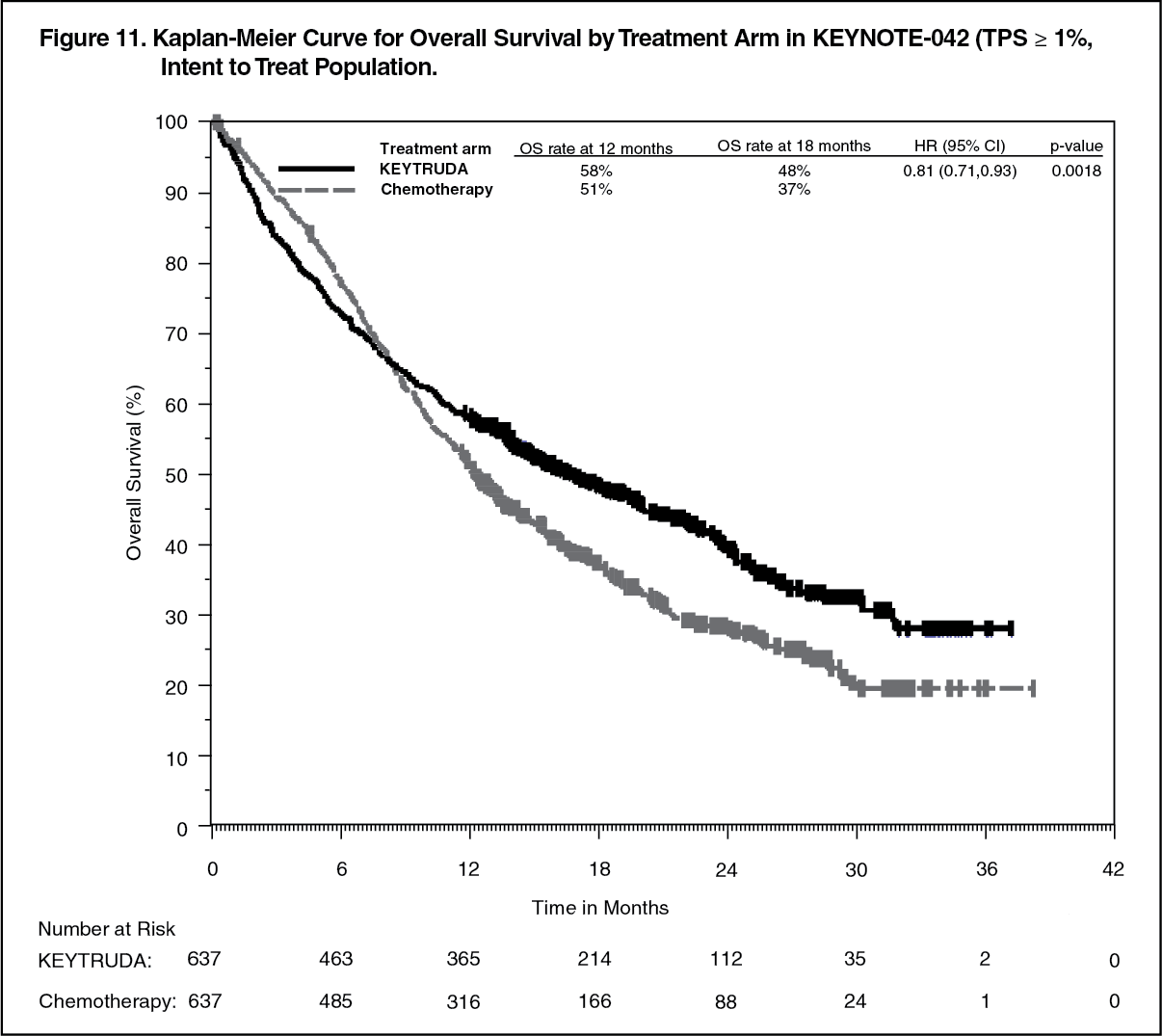 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image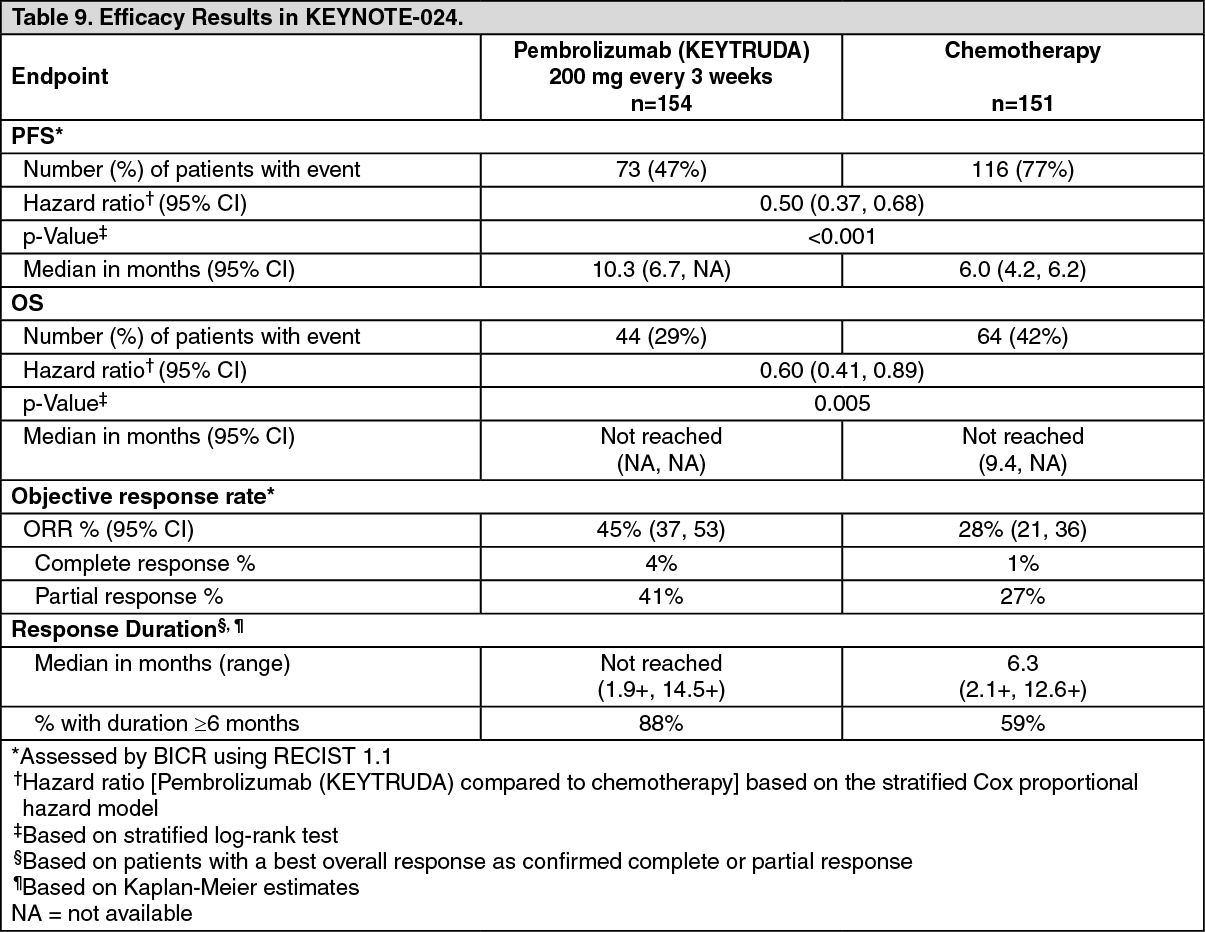 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image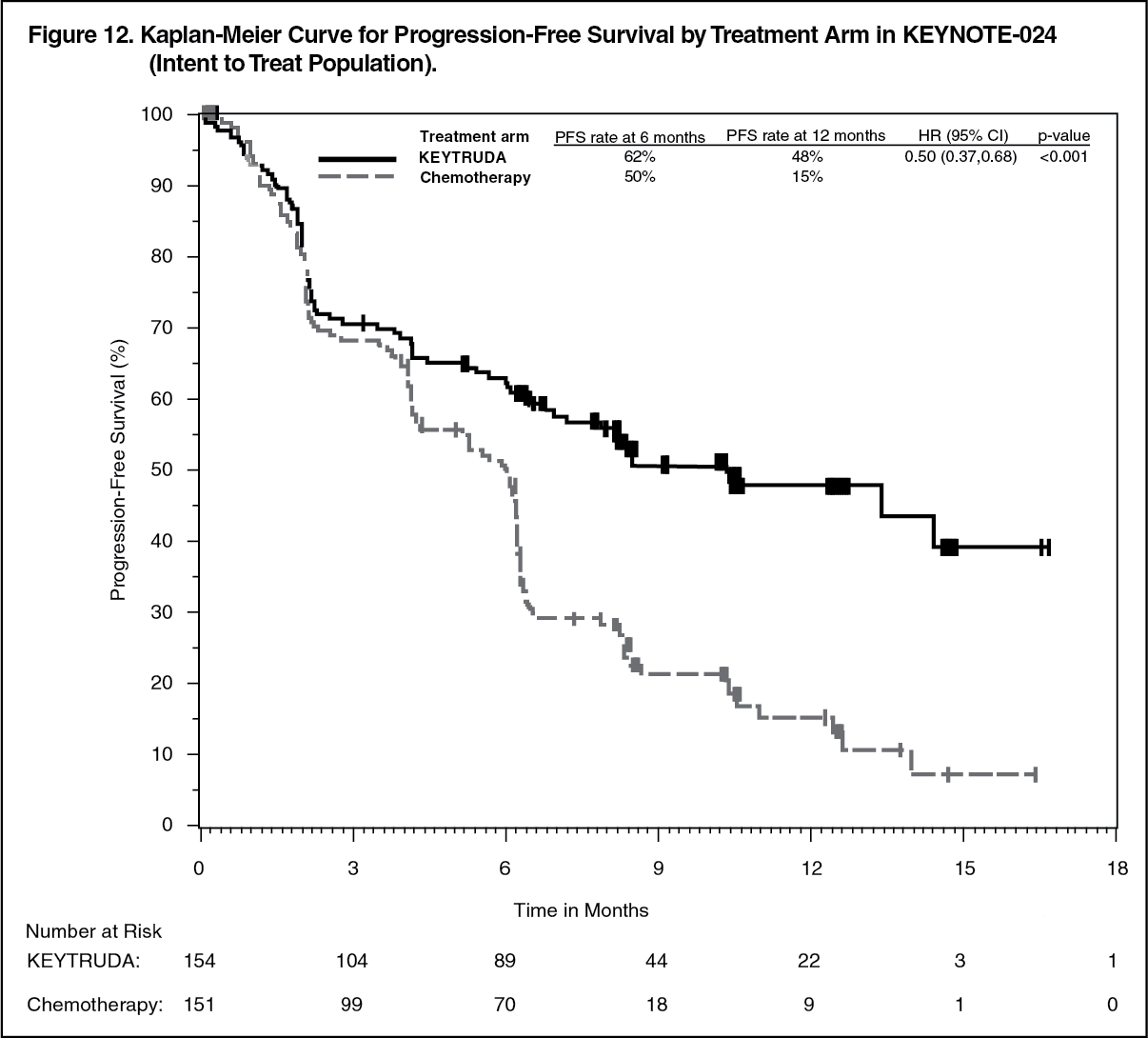 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image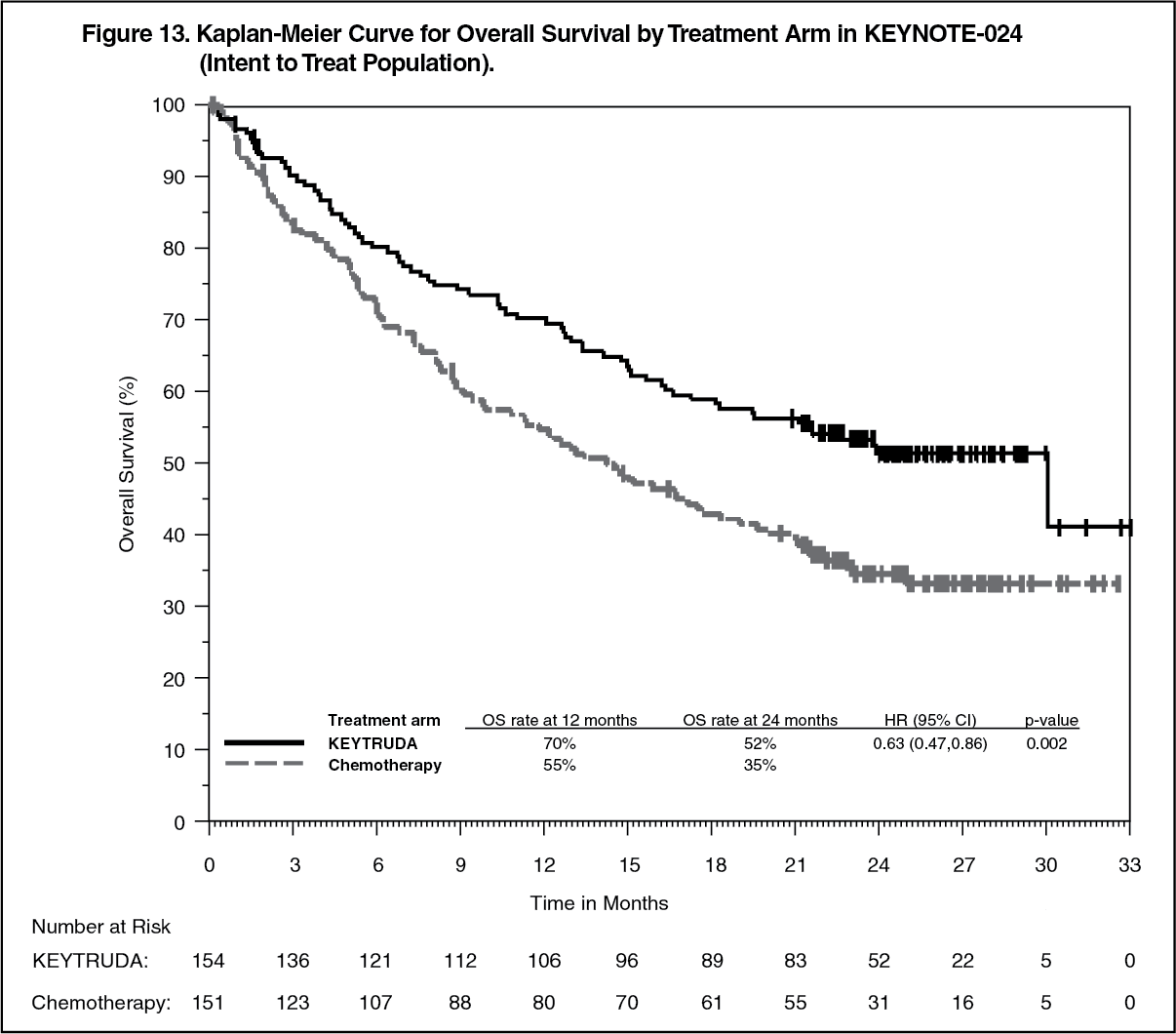 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image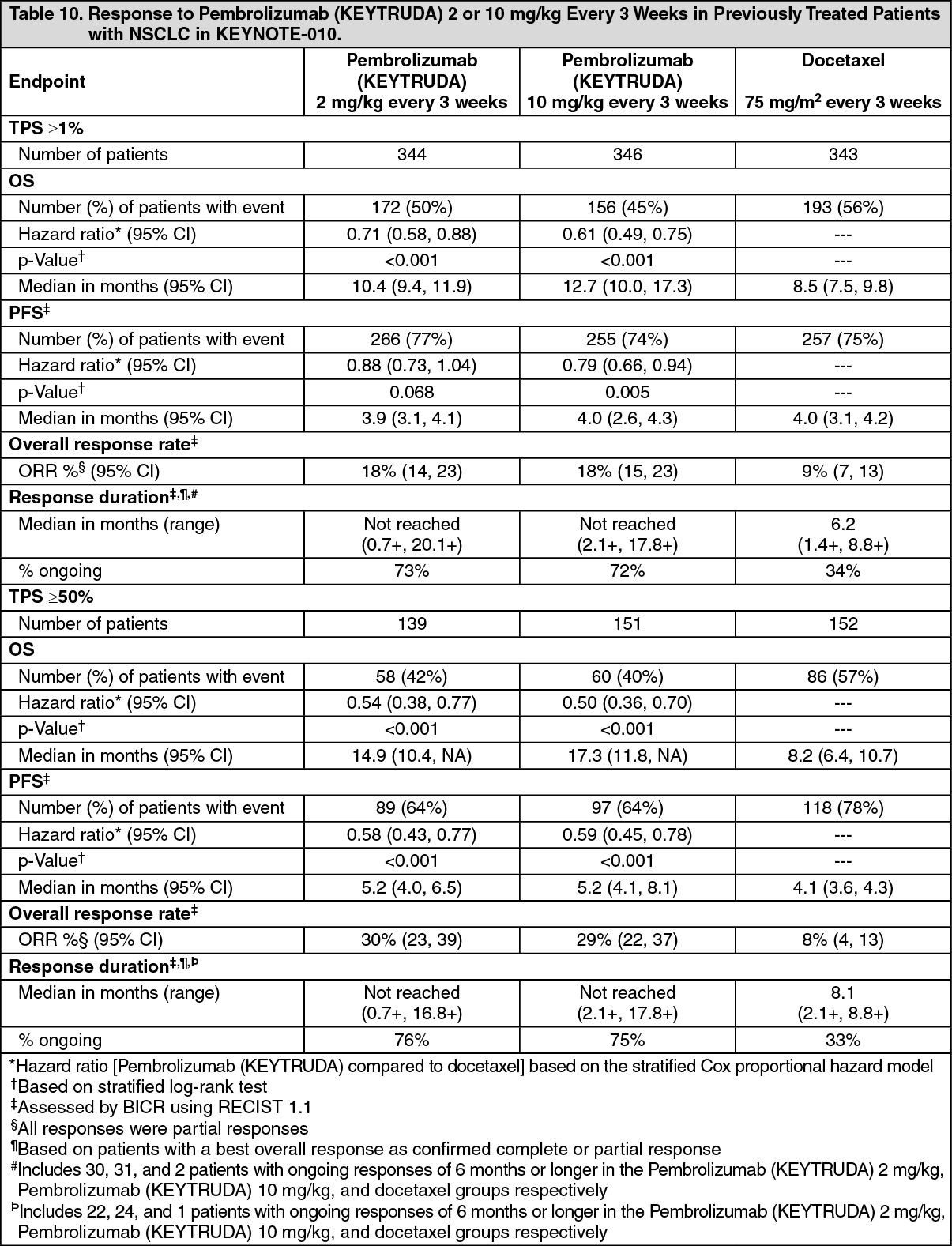 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image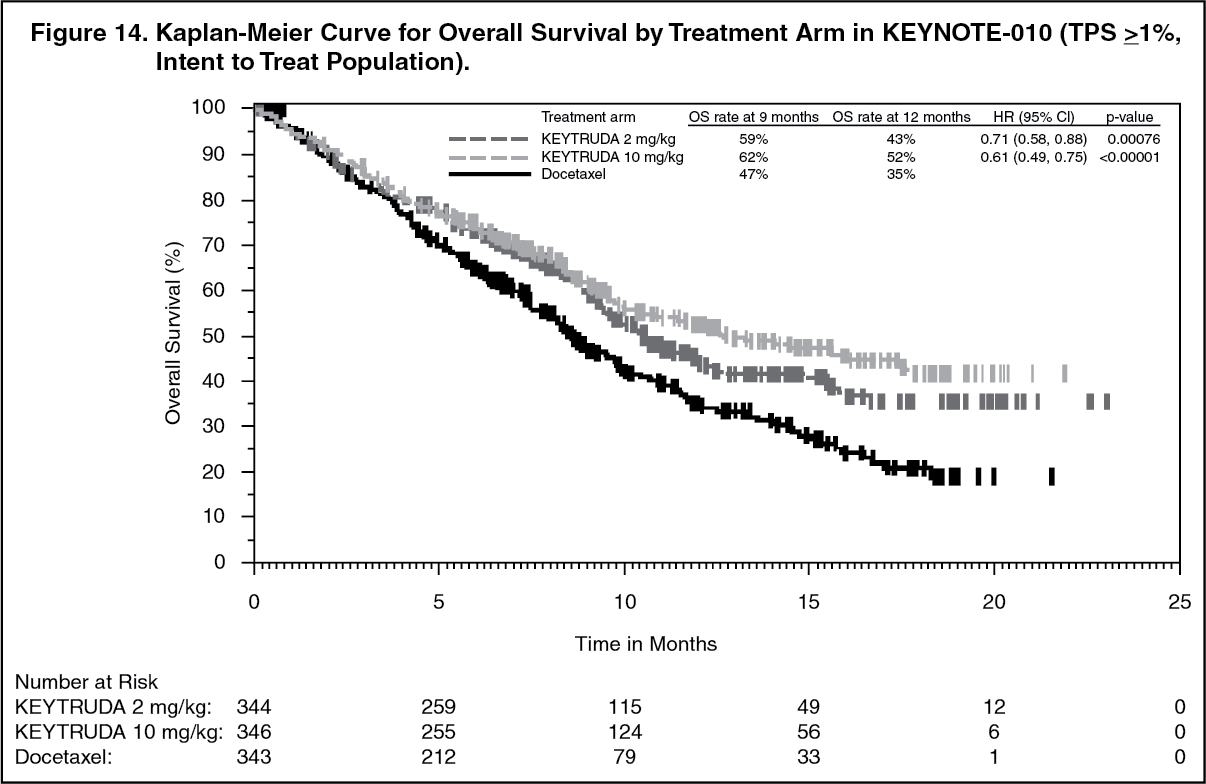 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image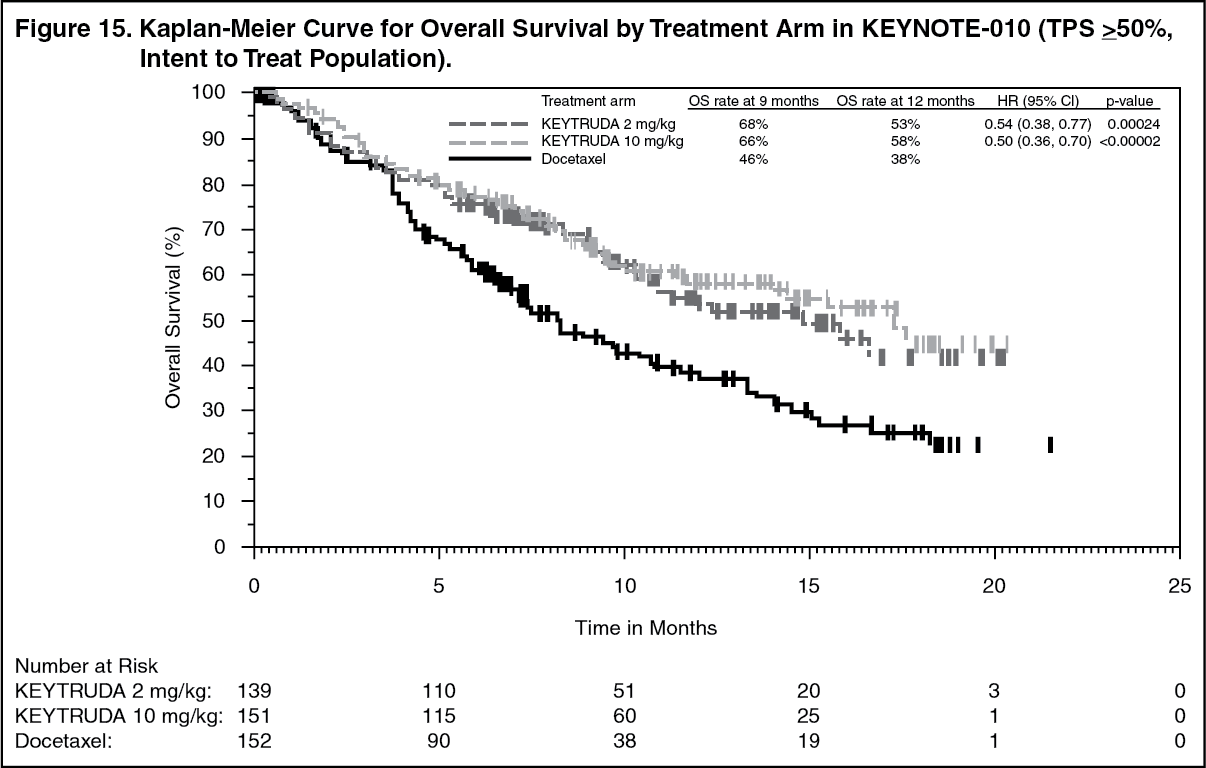 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image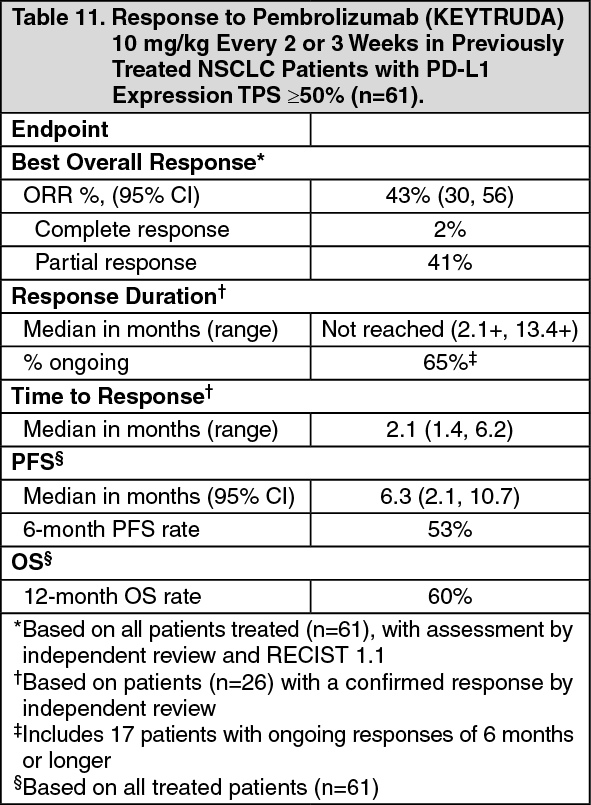 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image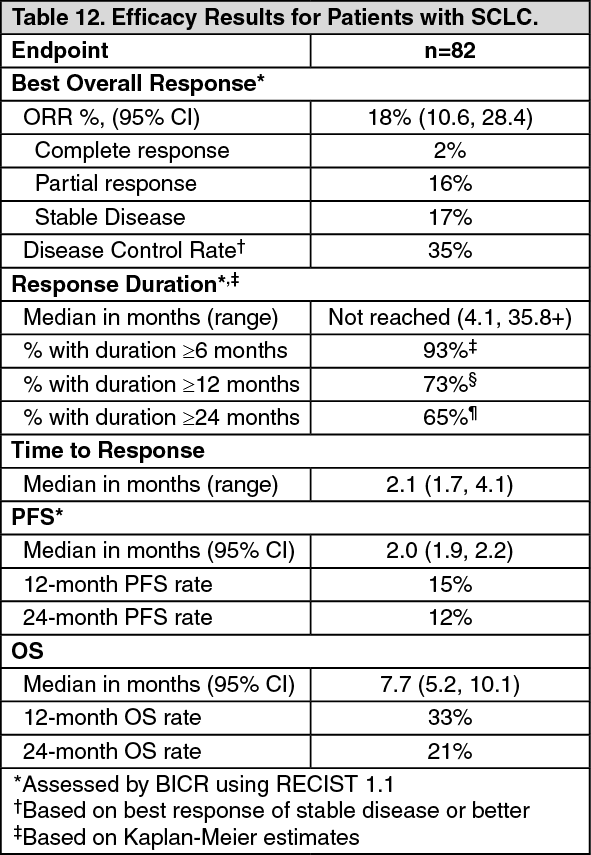 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image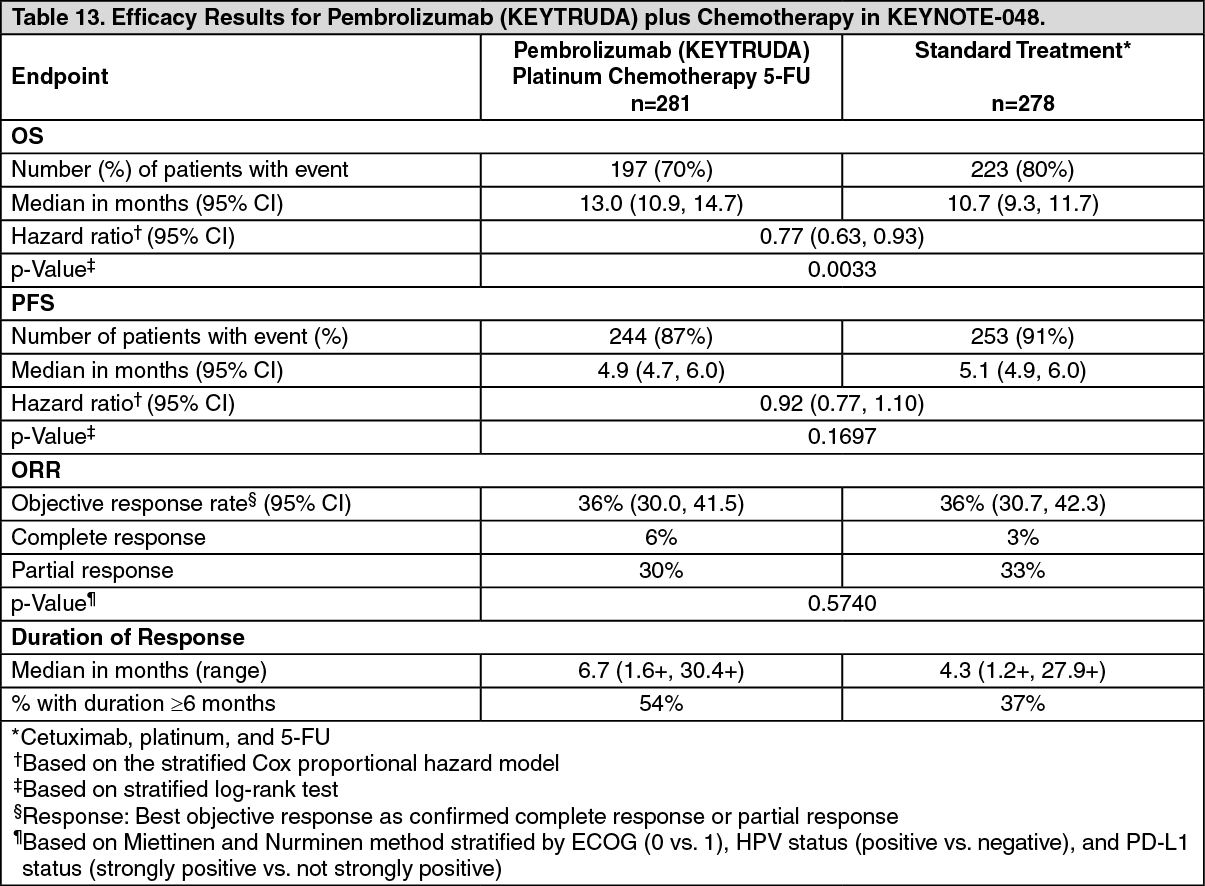 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image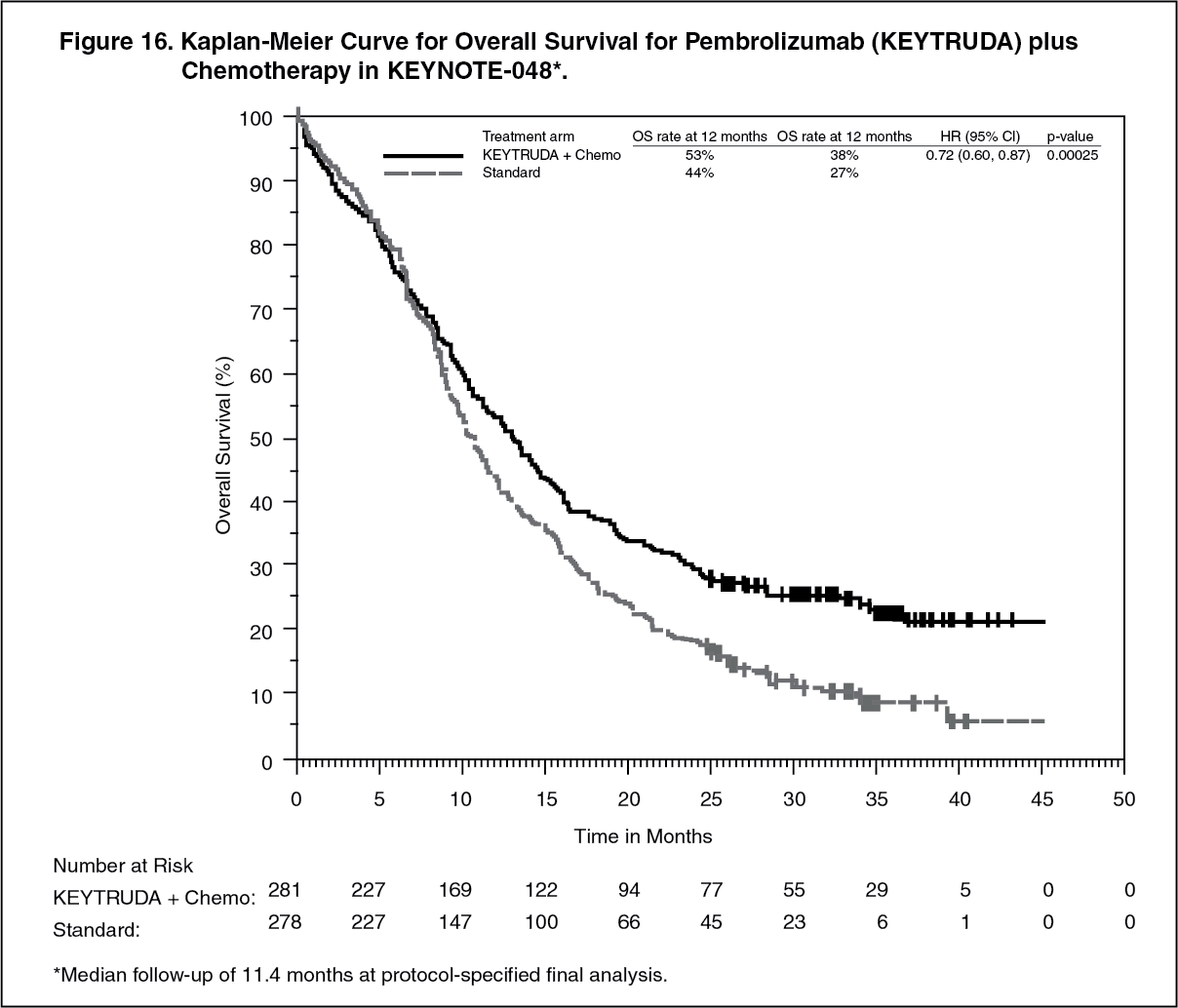 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image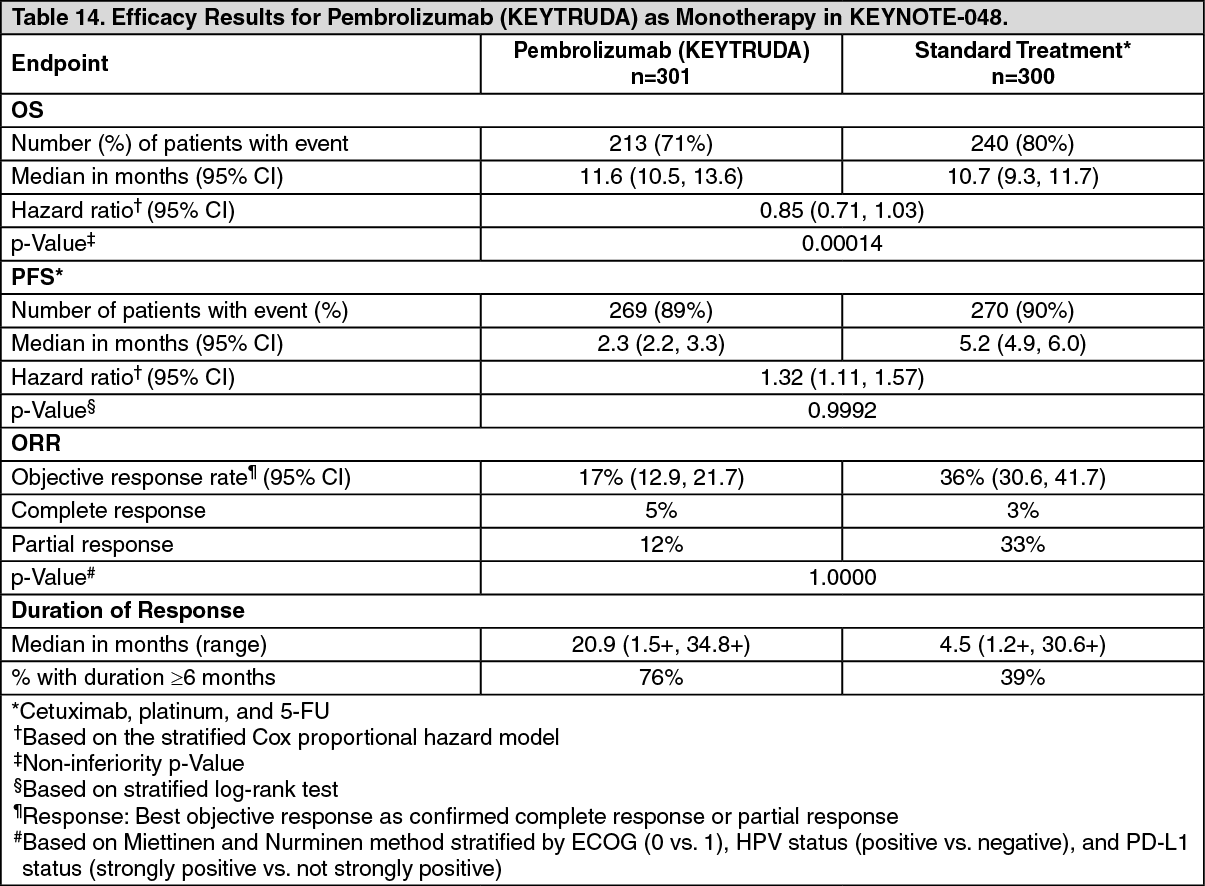 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image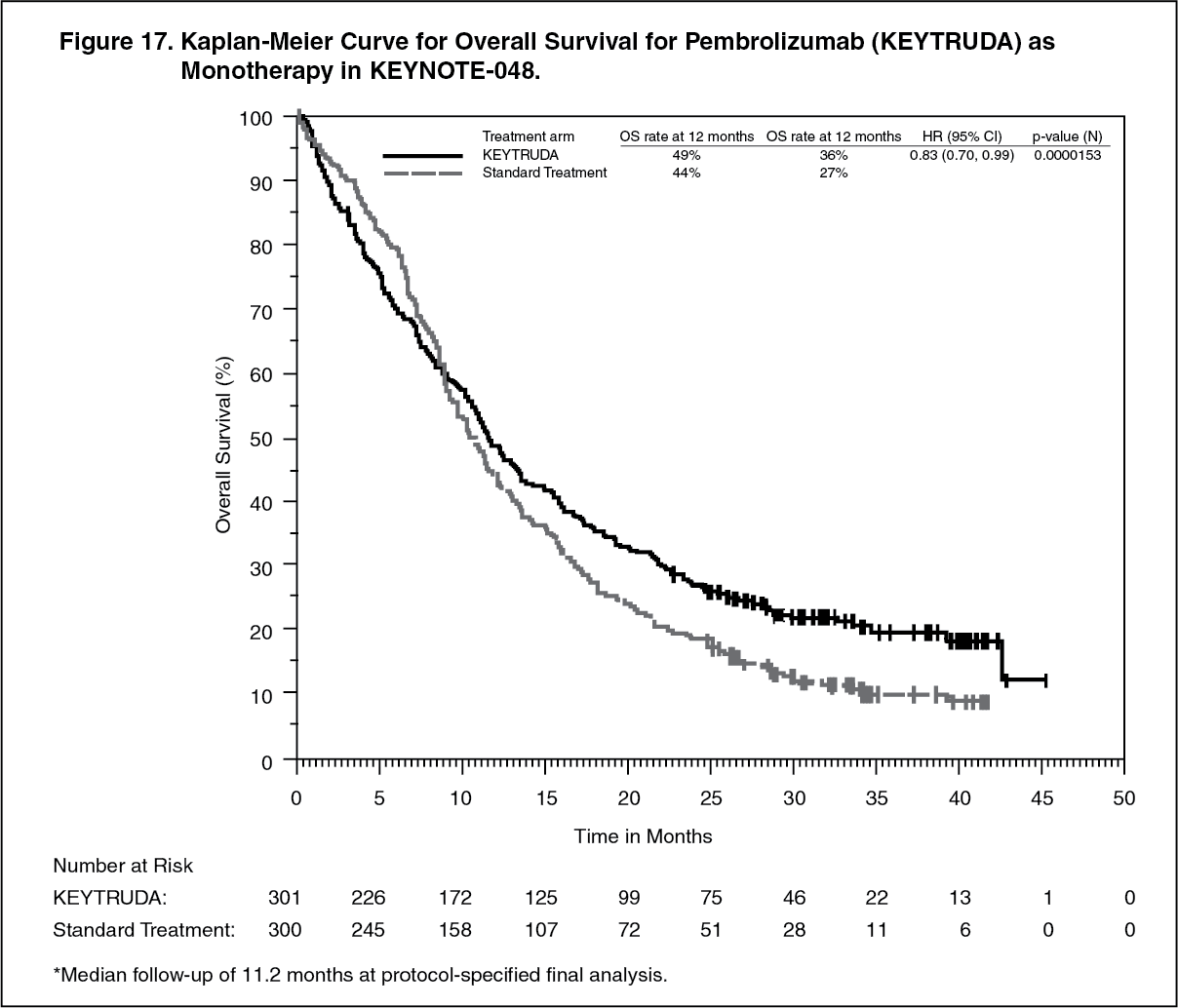 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image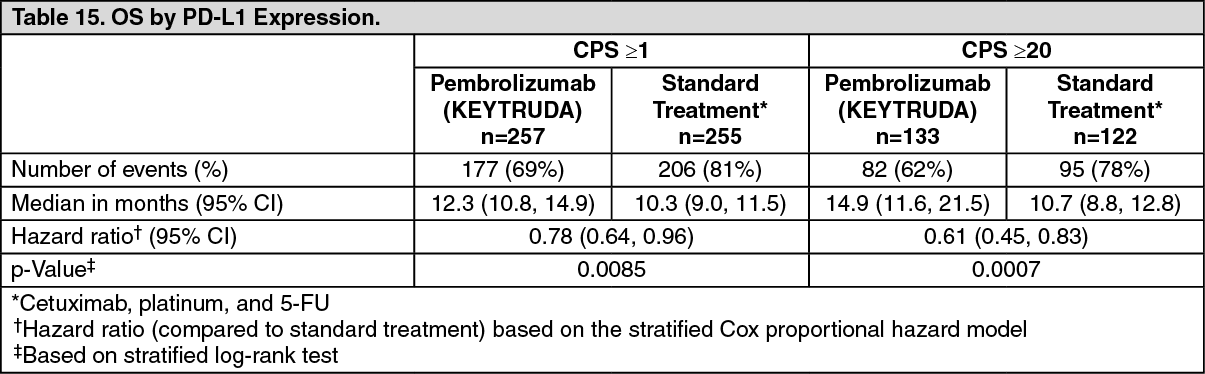 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image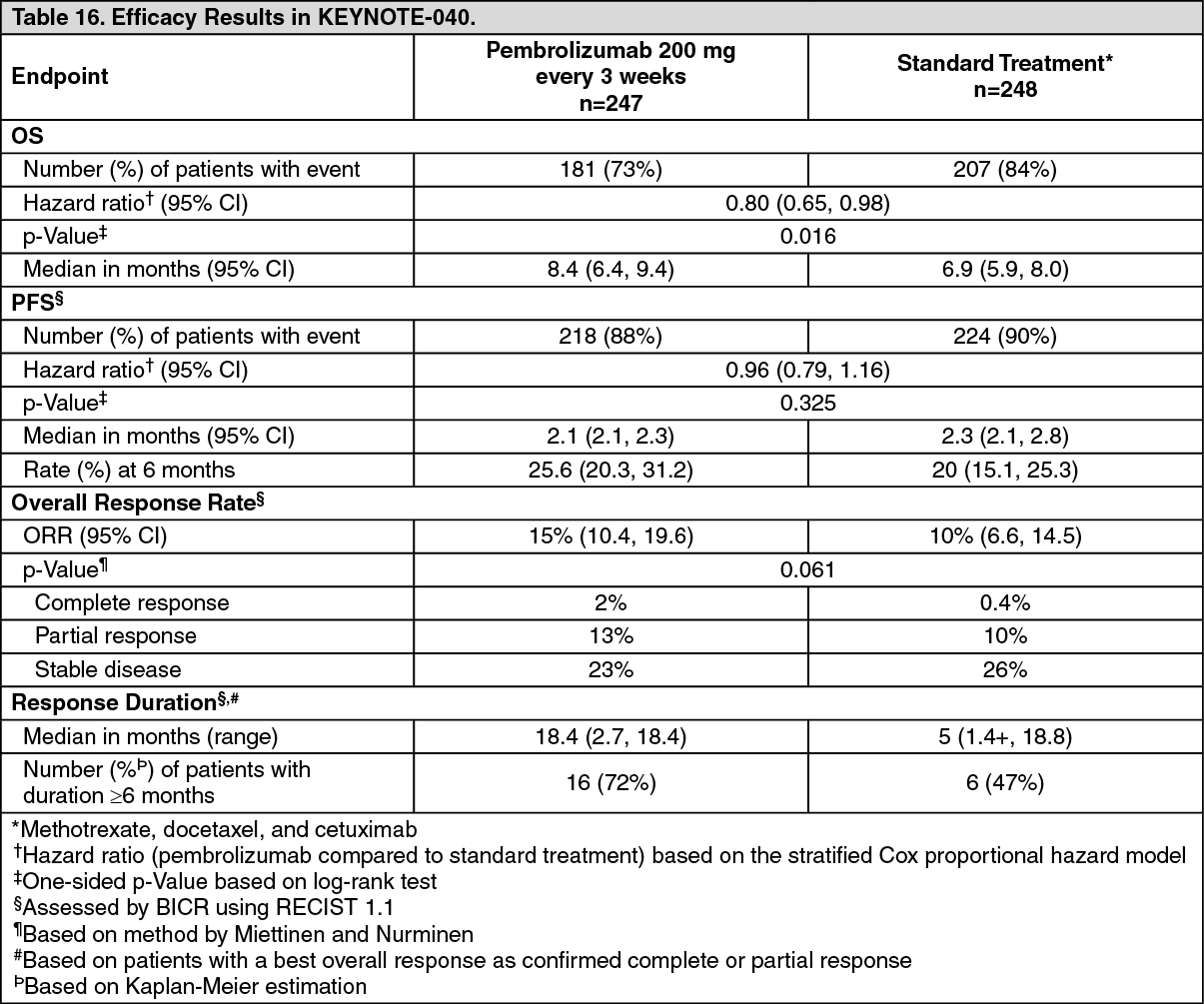 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image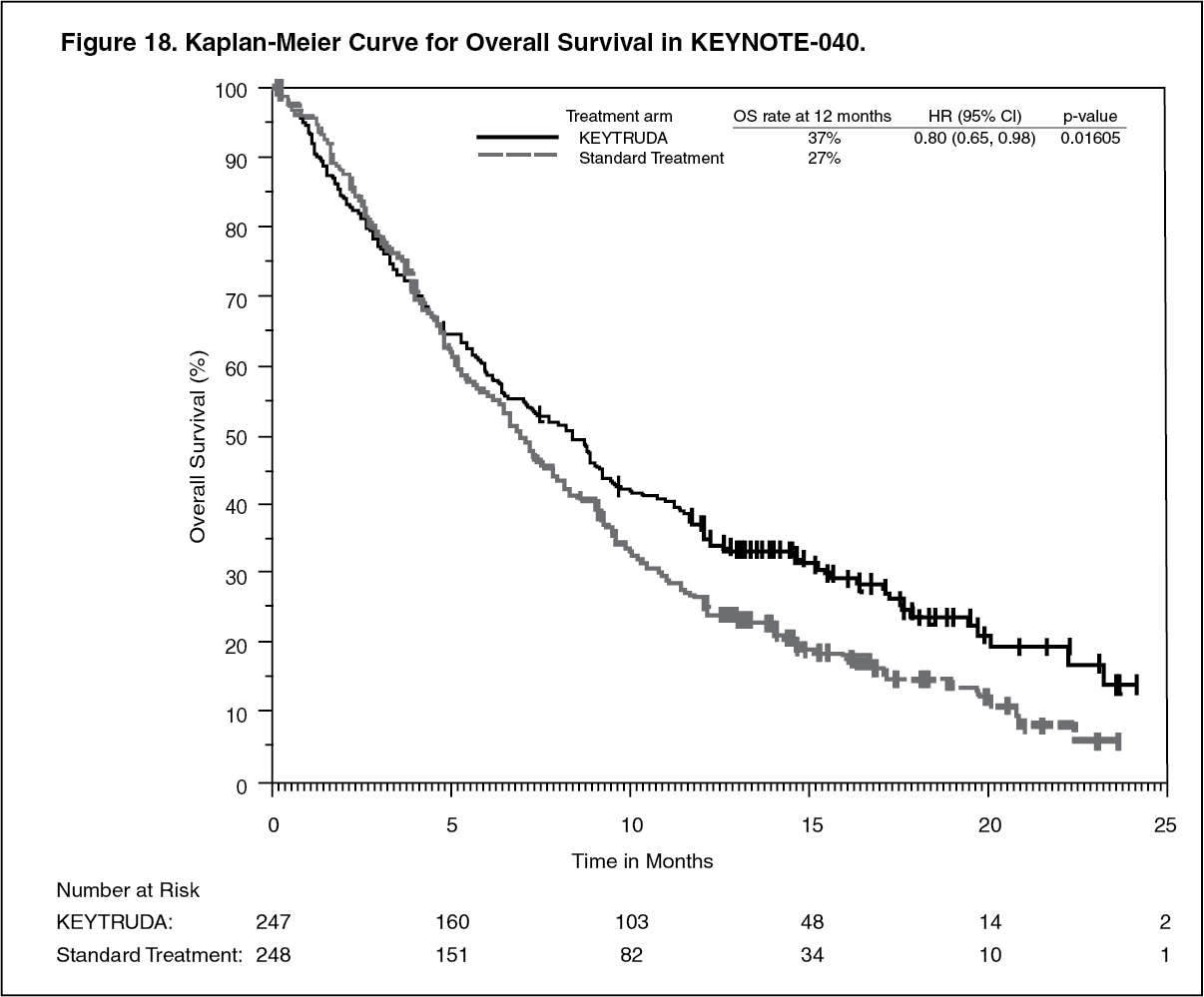 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image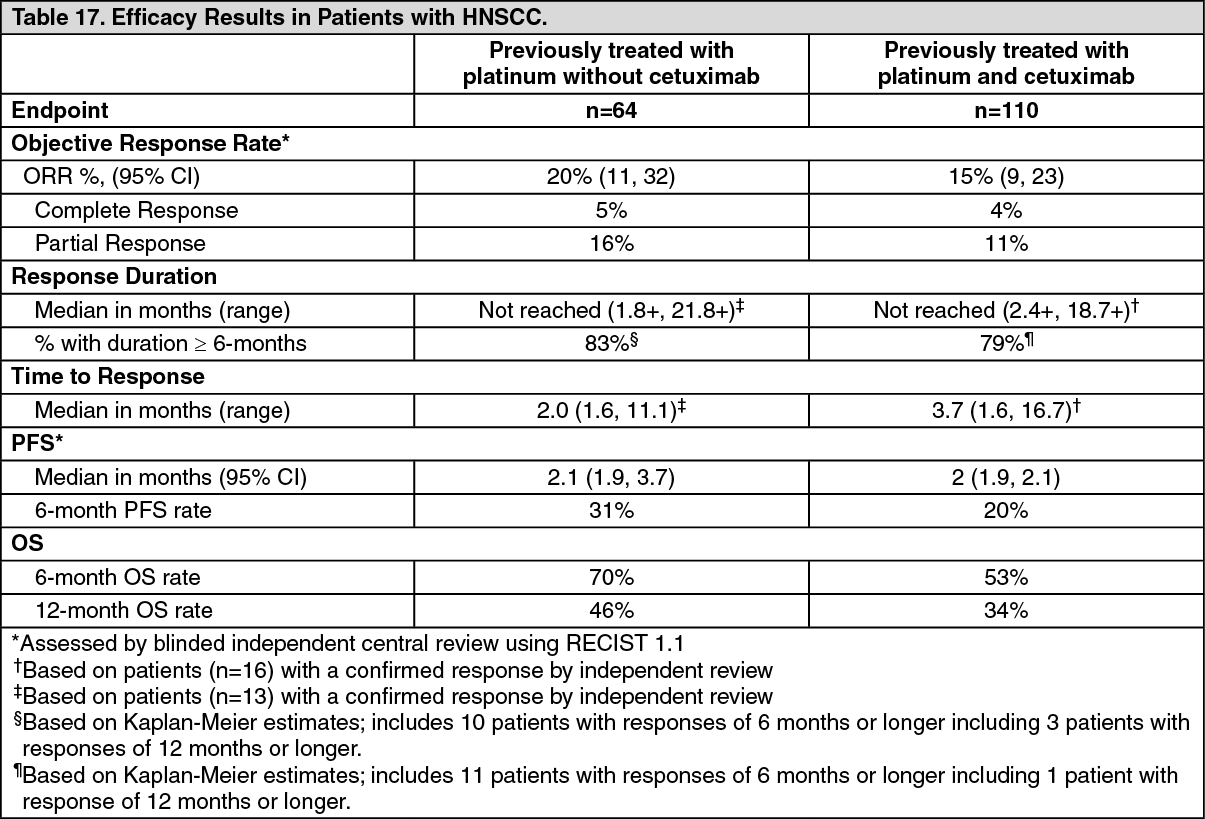 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image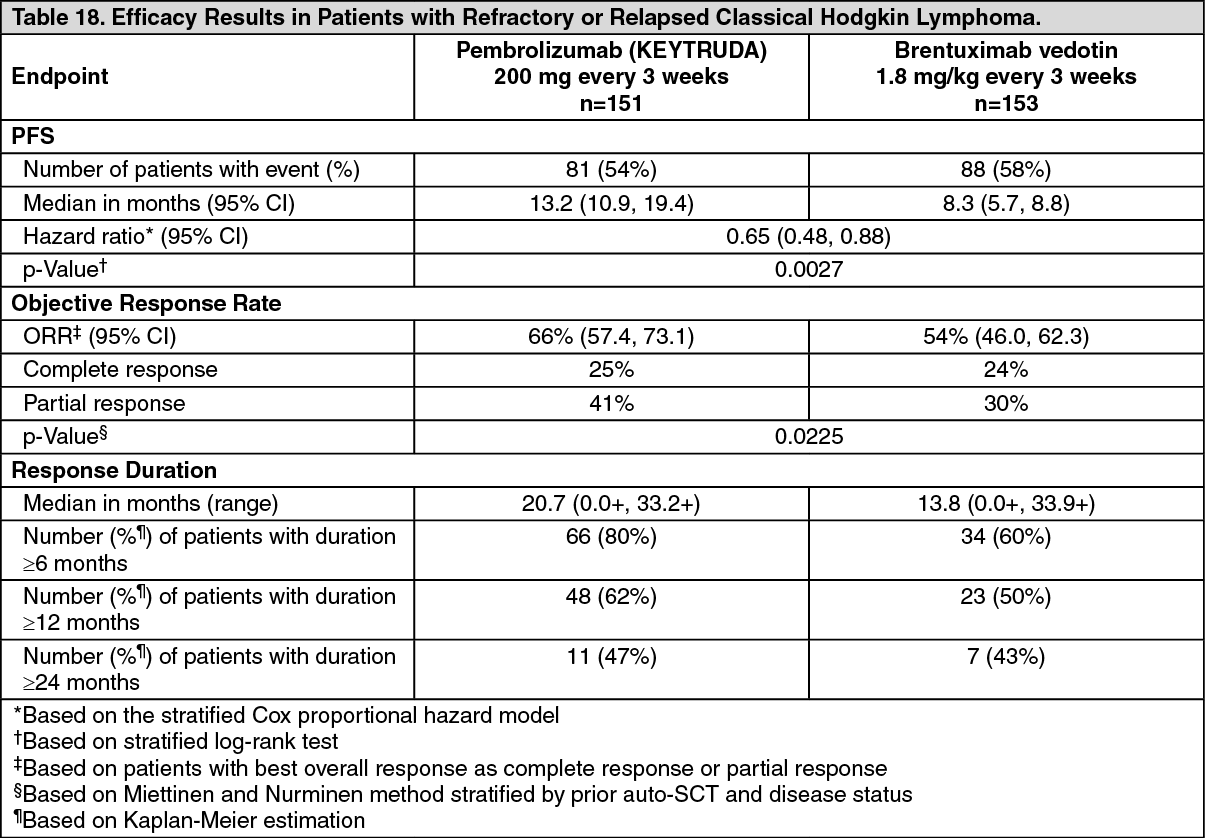 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image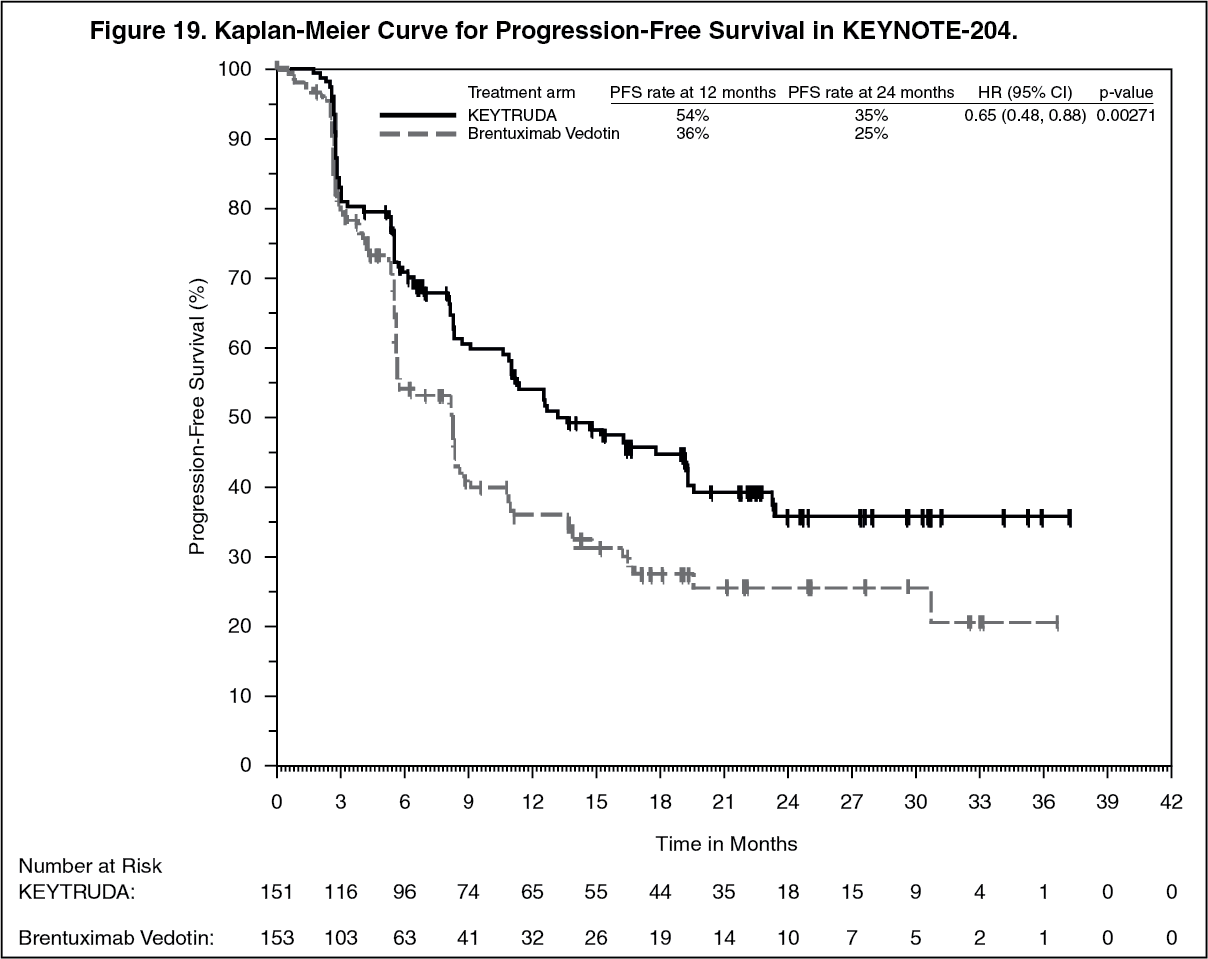 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image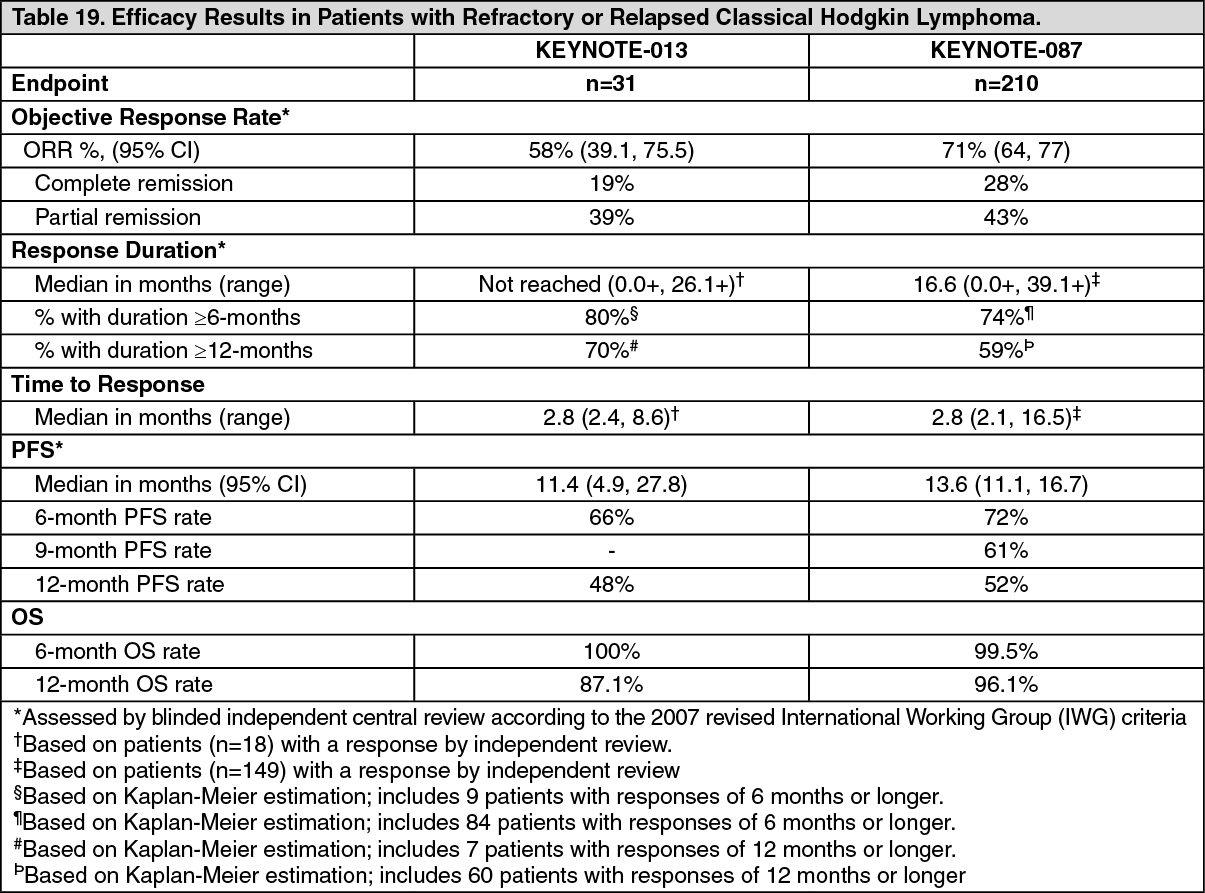 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image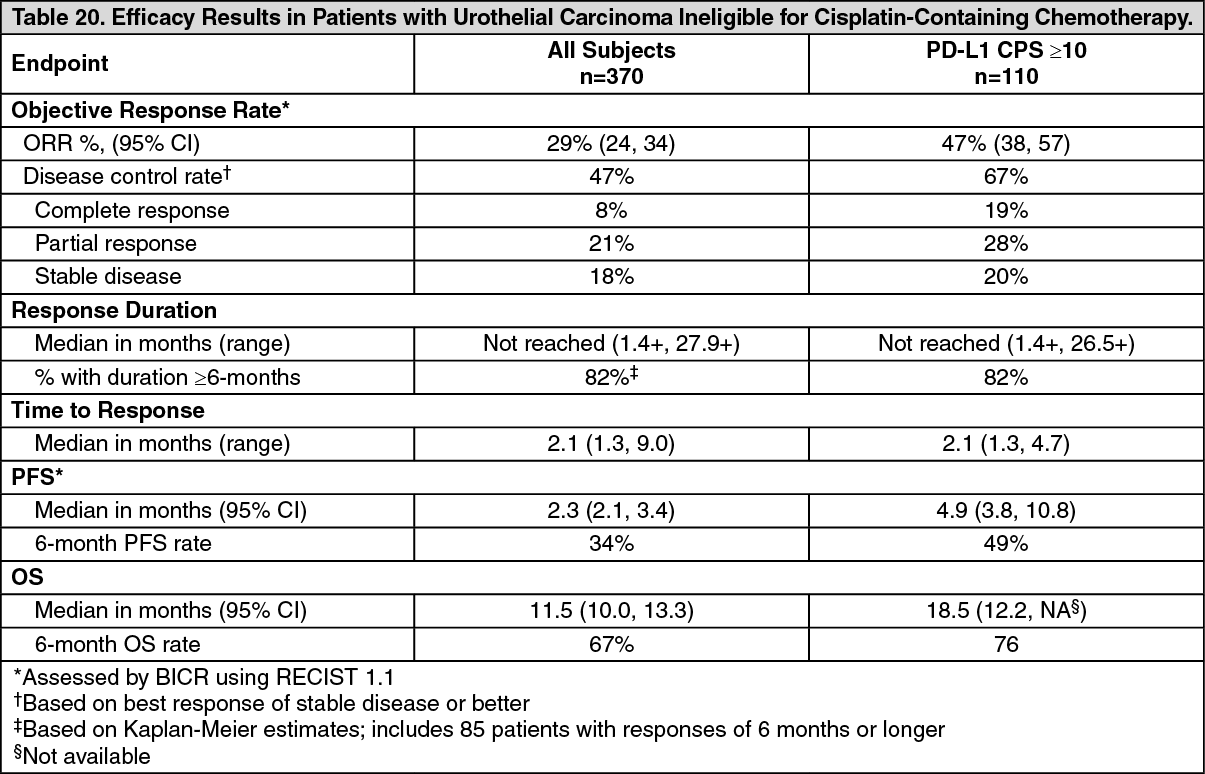 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image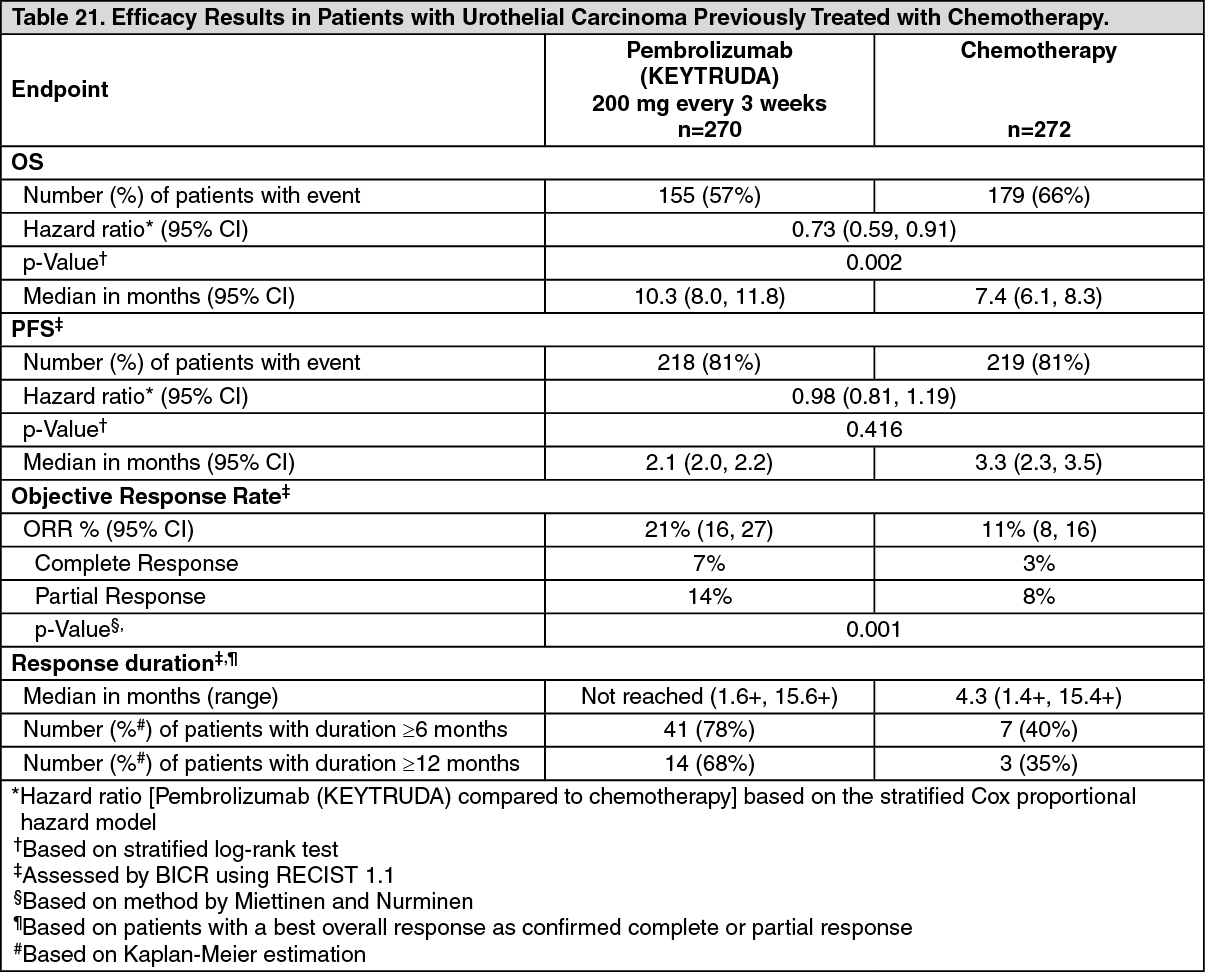 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image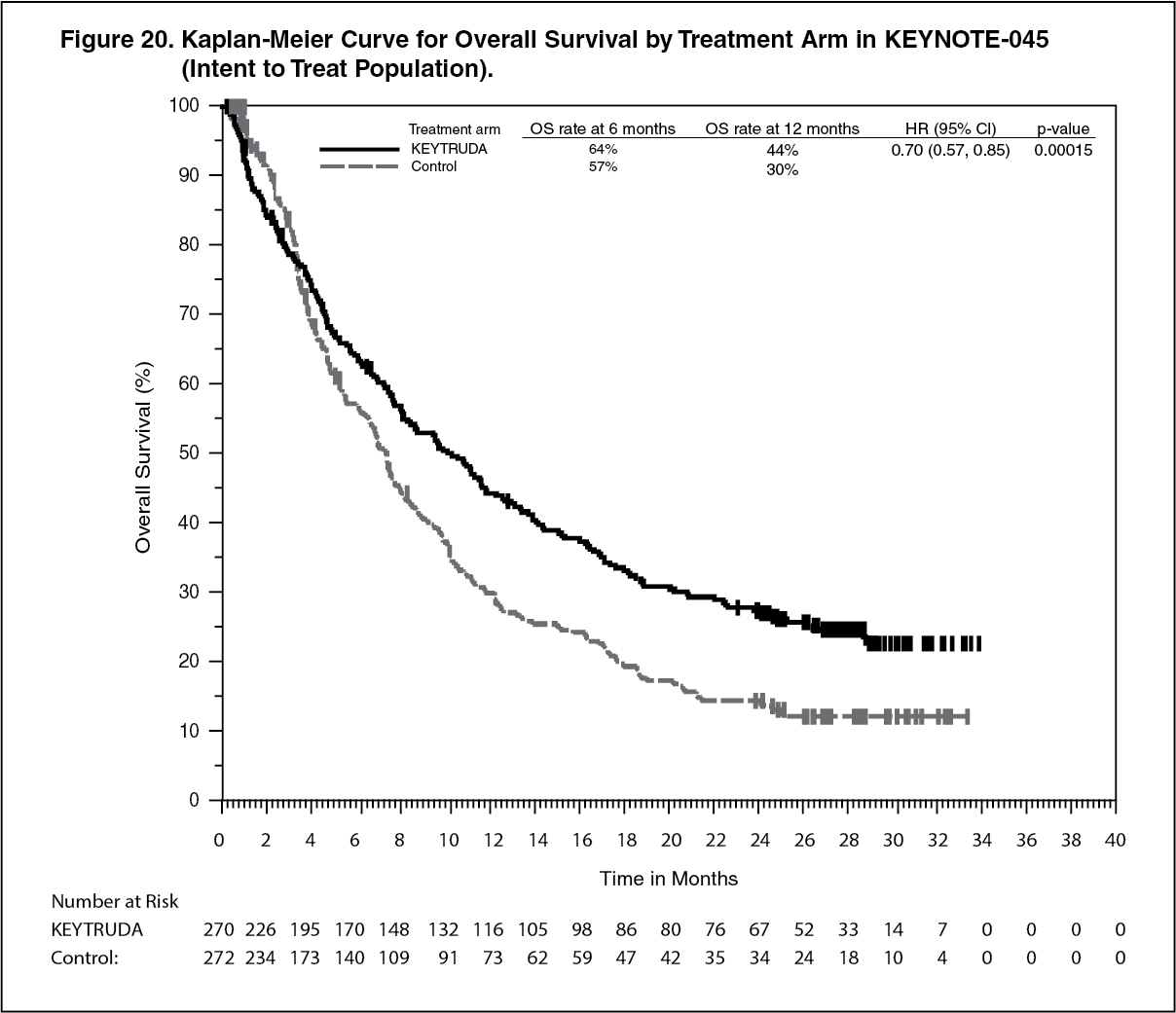 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image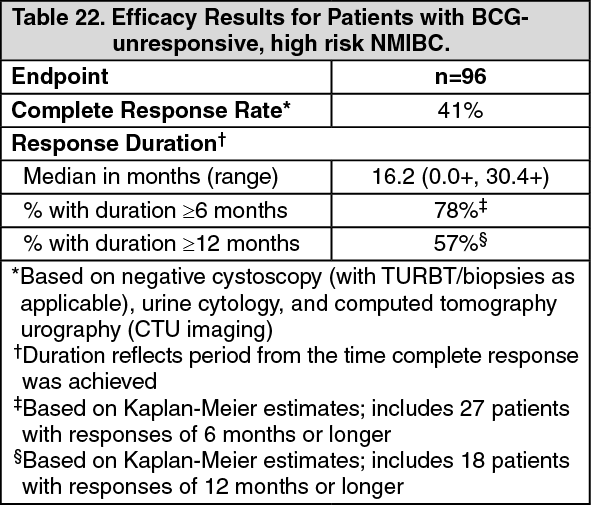 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image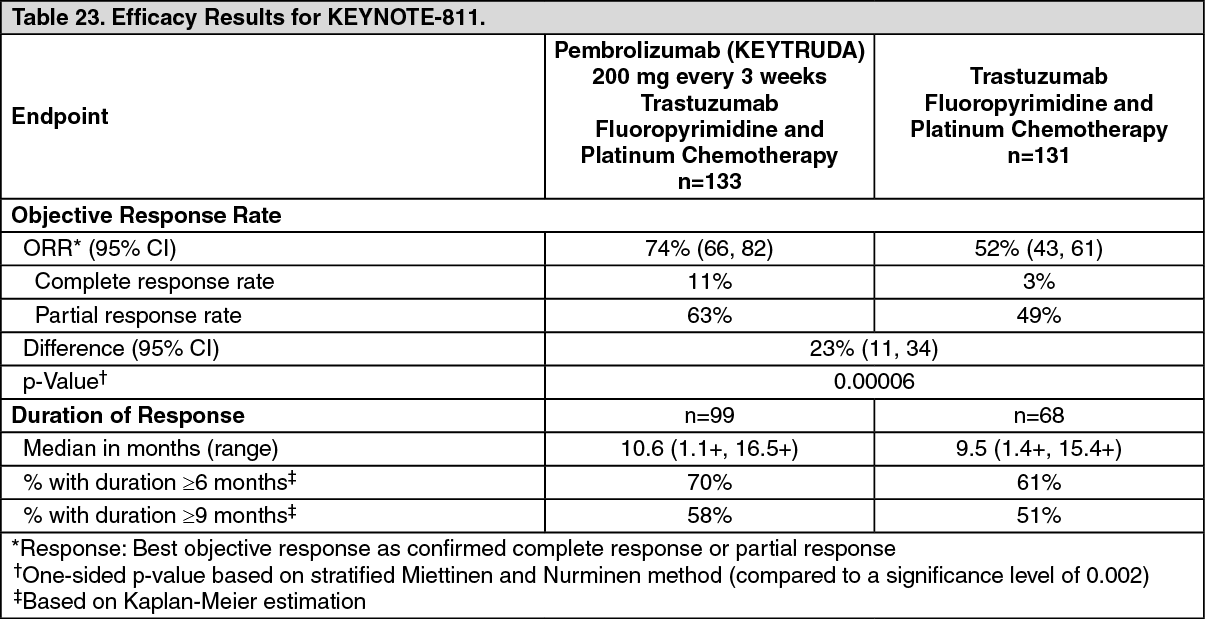 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image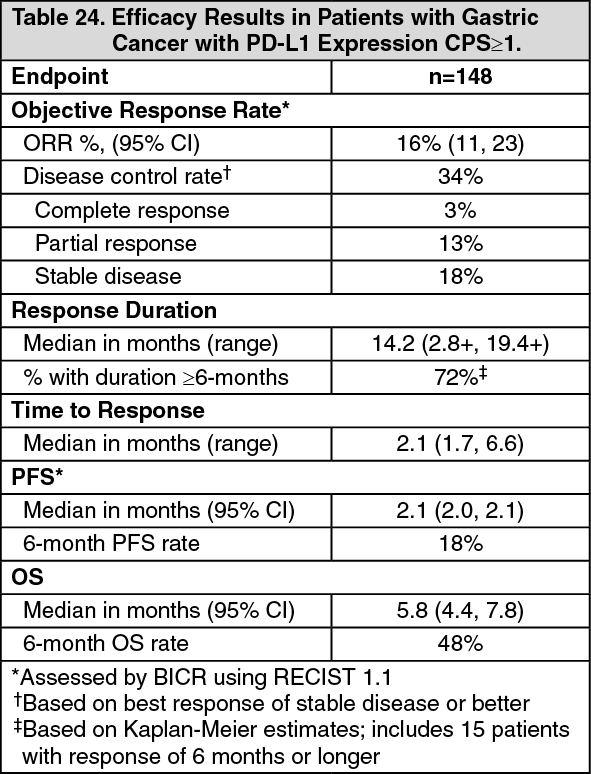 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image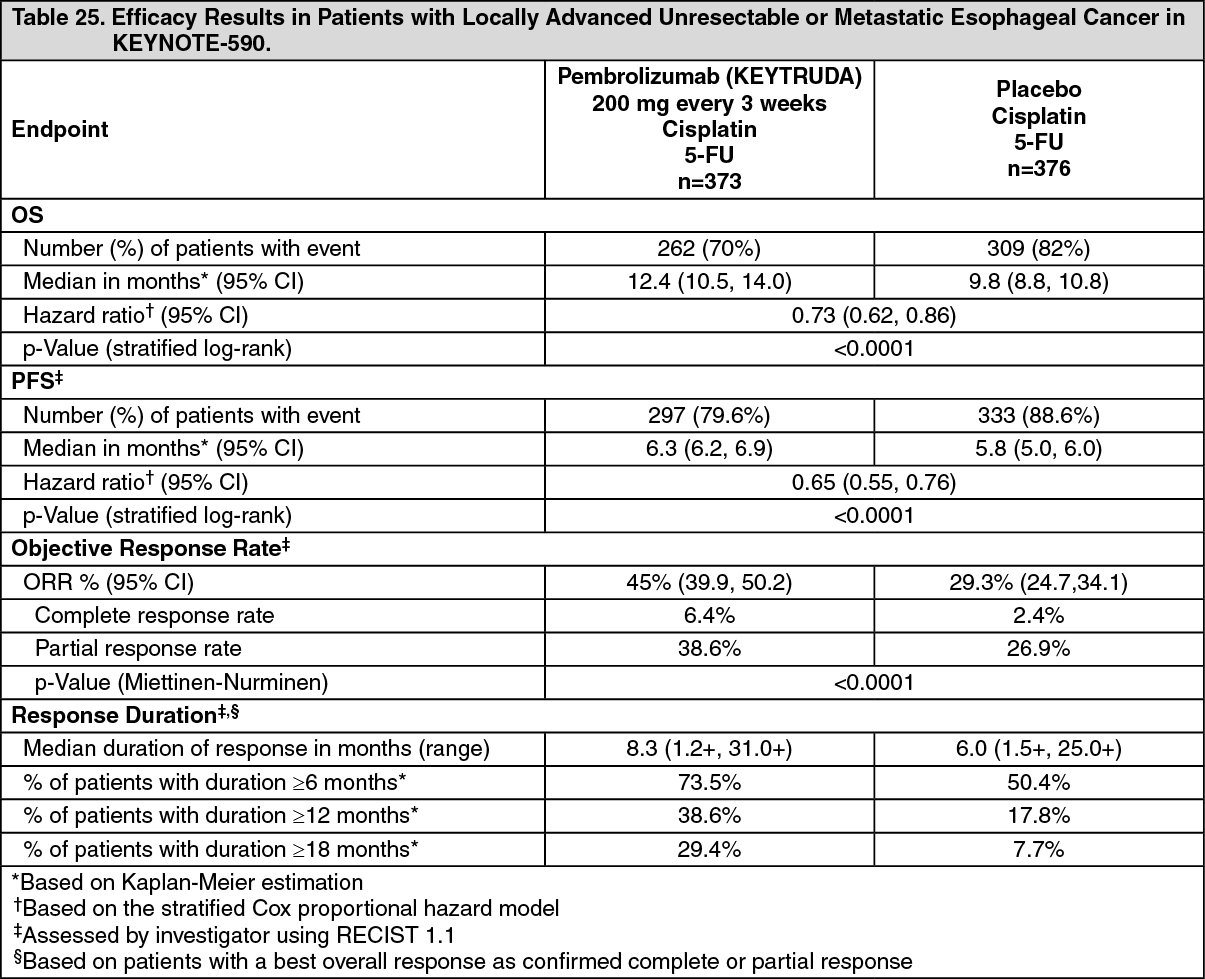 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image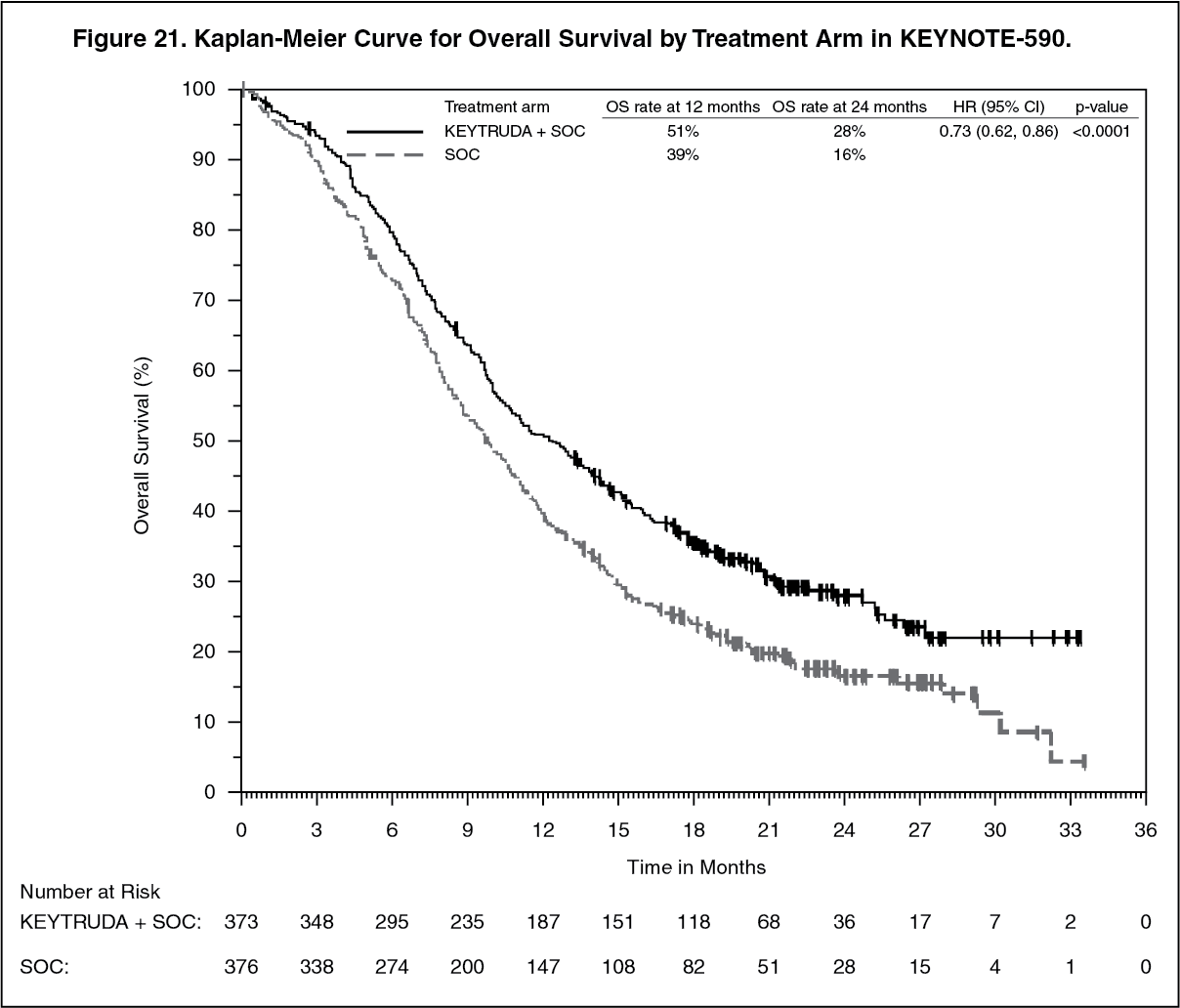 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image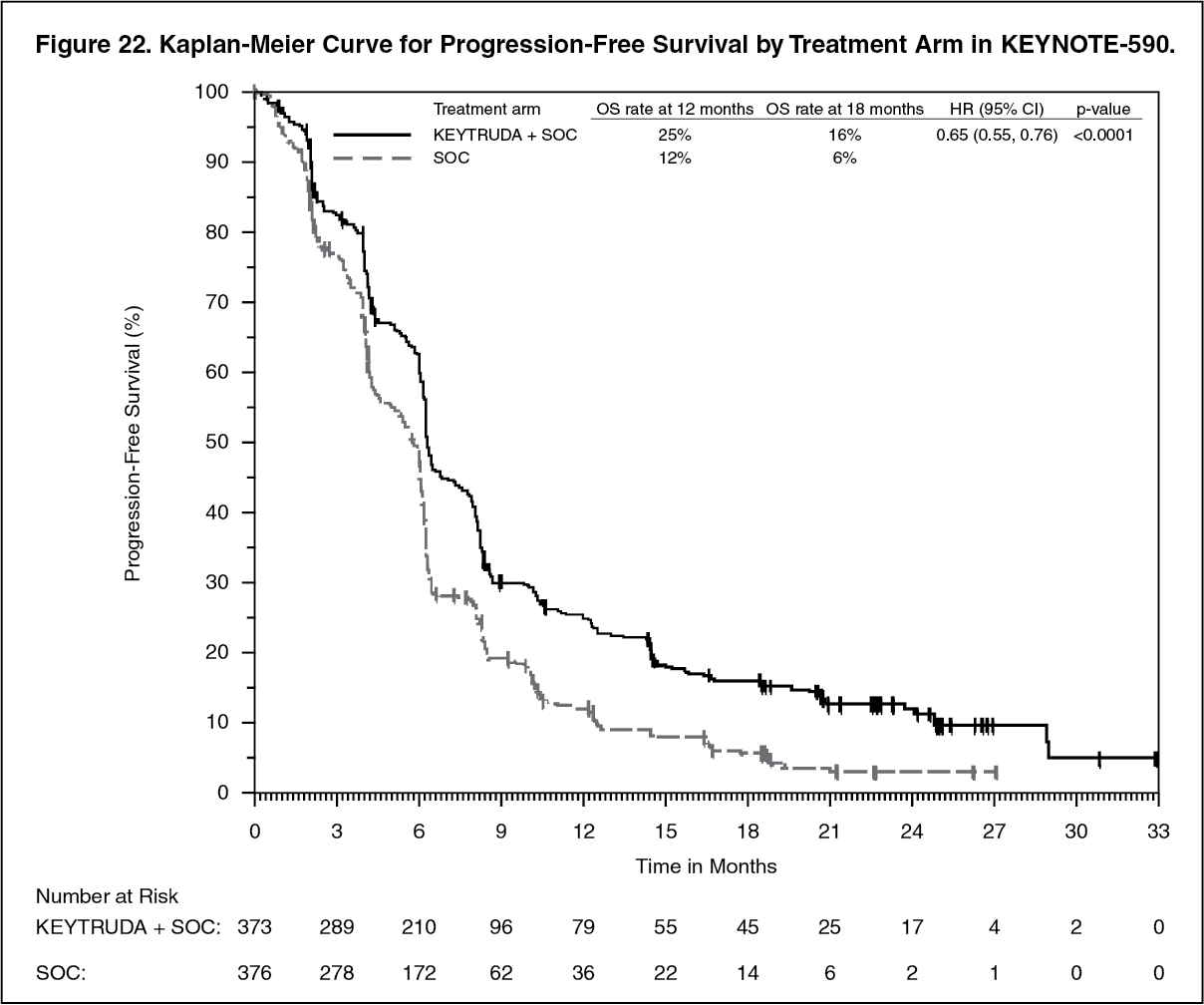 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image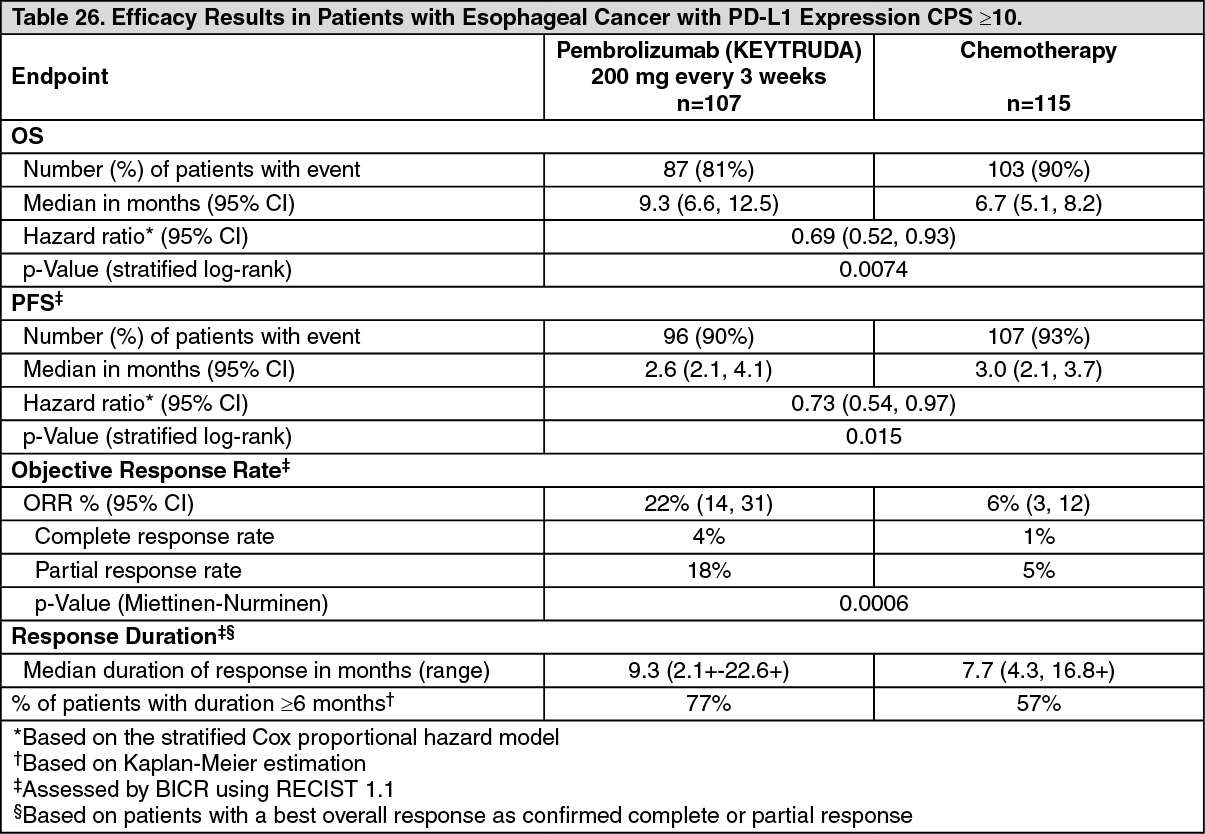 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image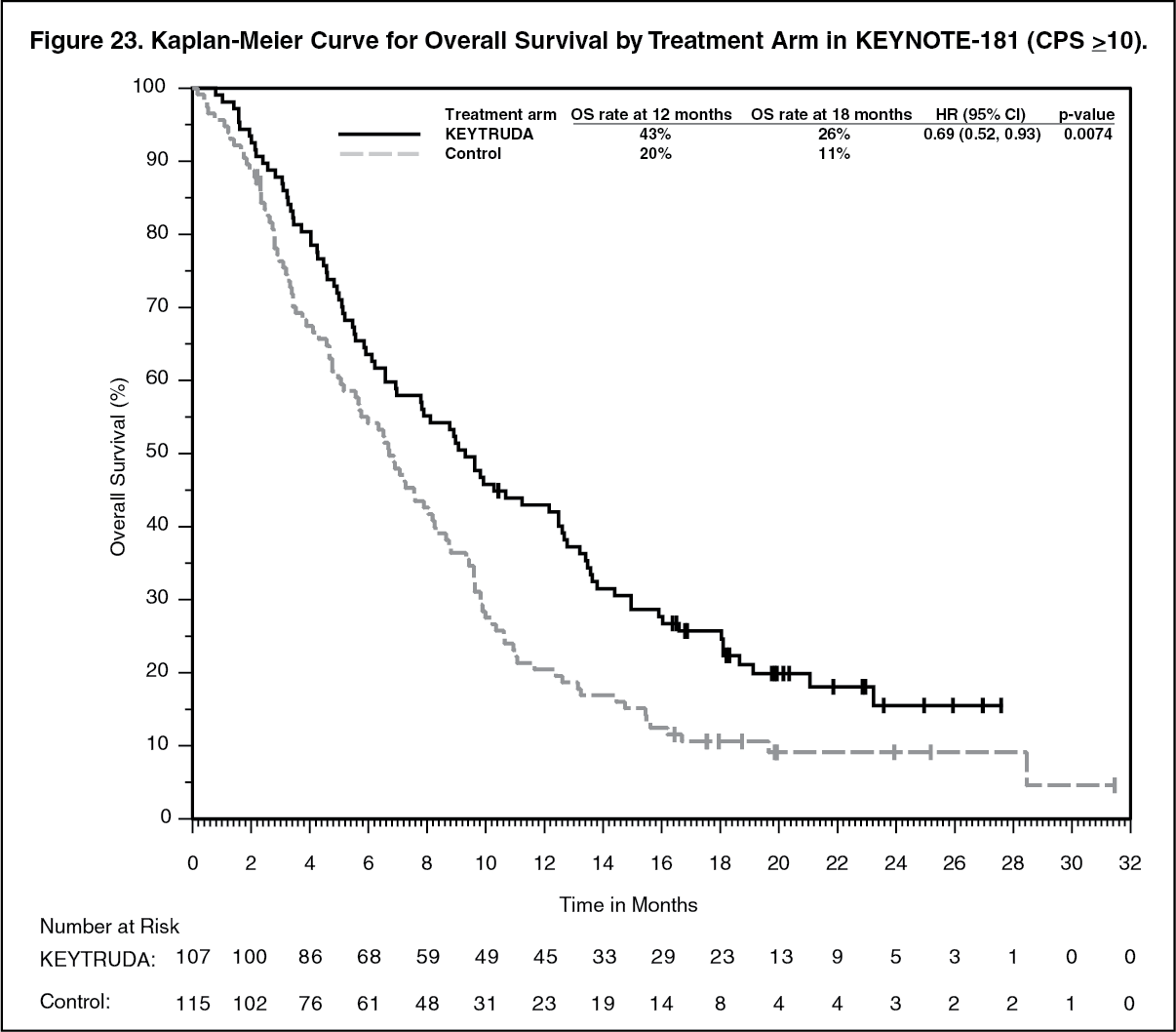 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image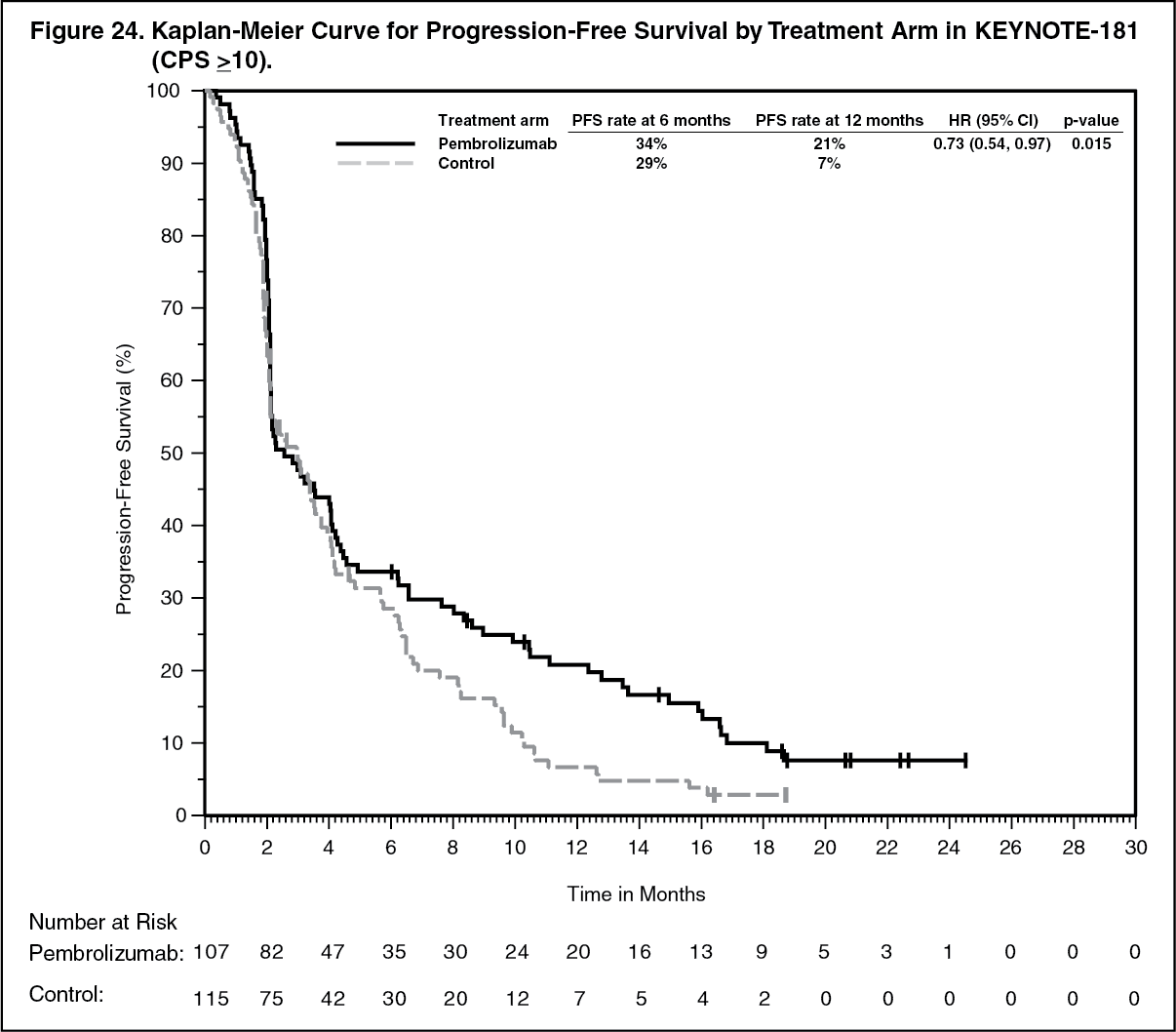 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image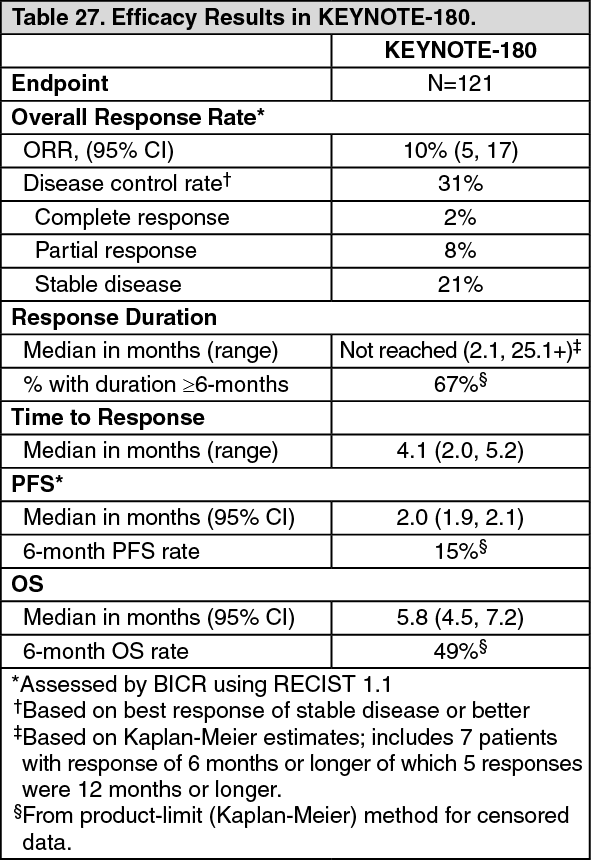 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image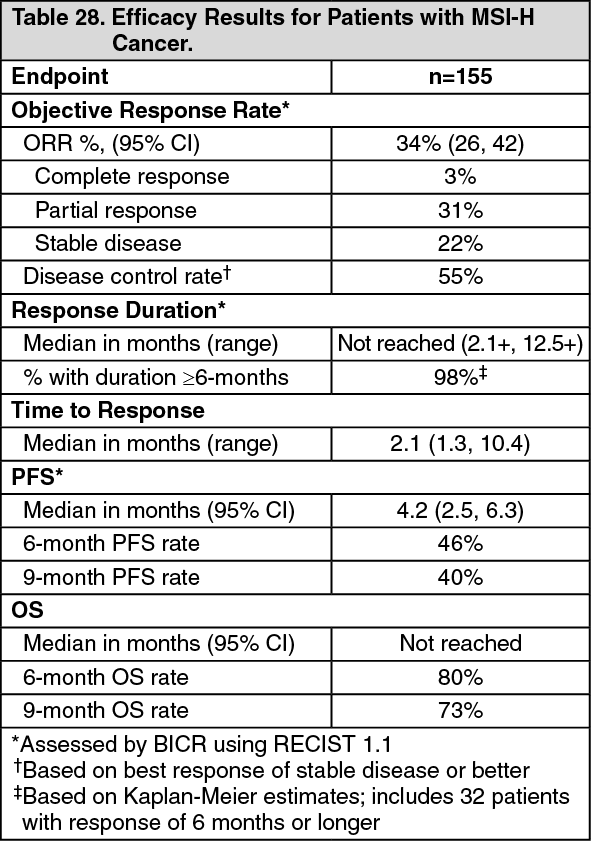 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image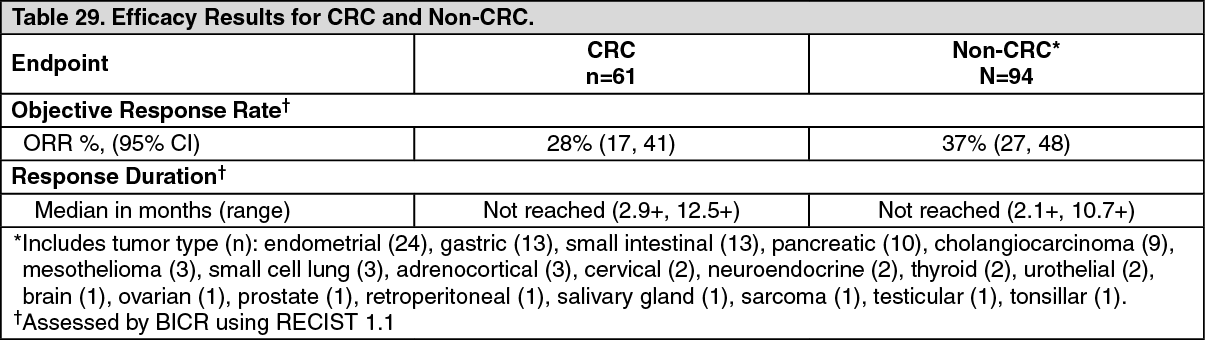 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image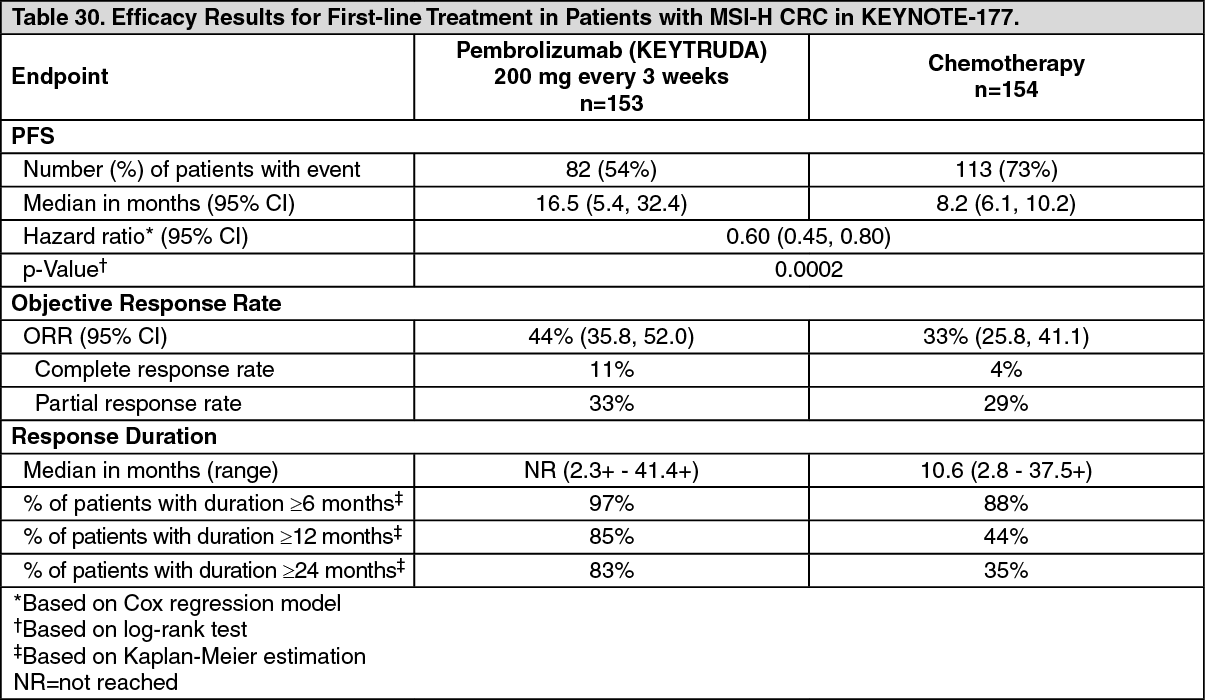 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image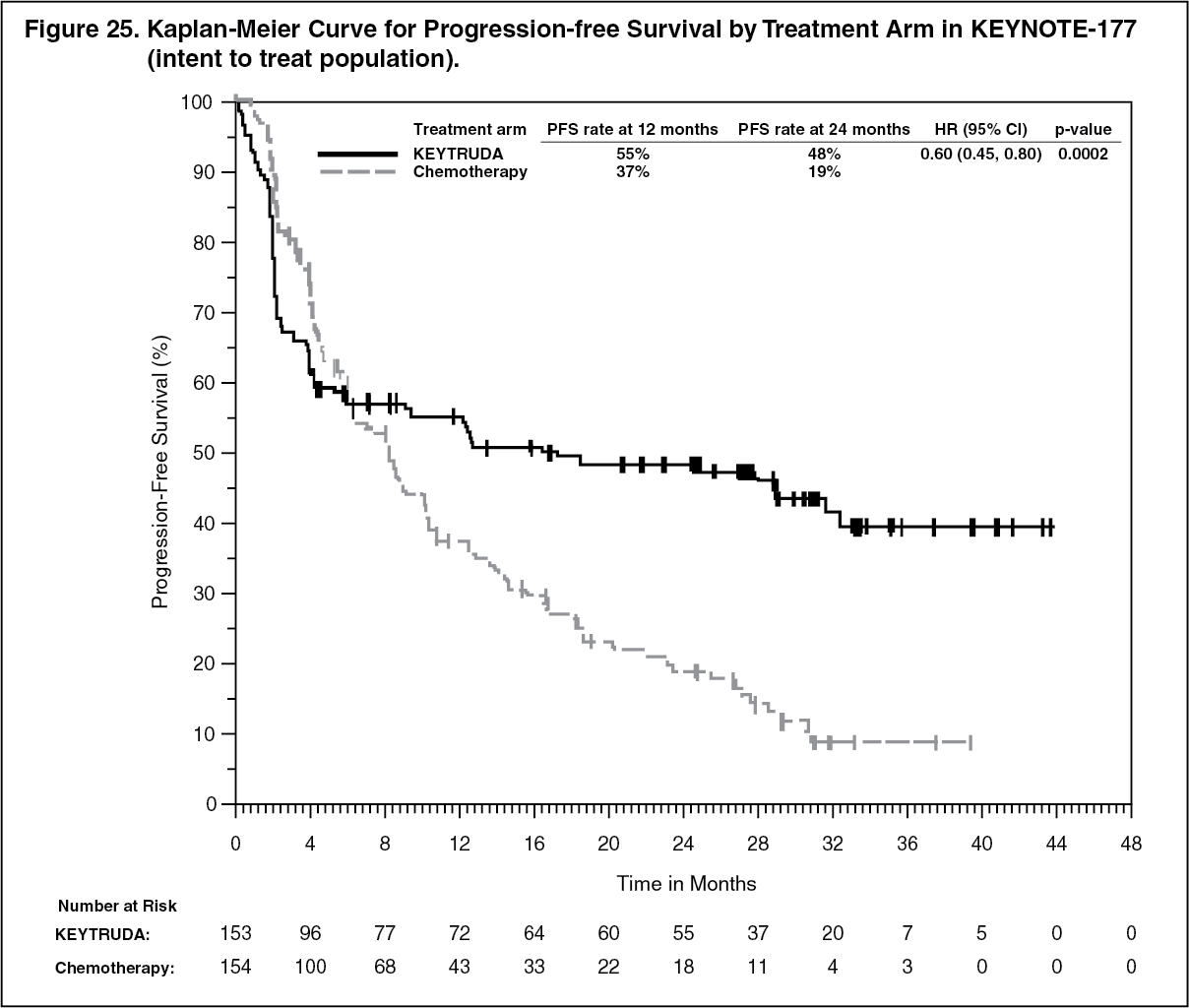 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image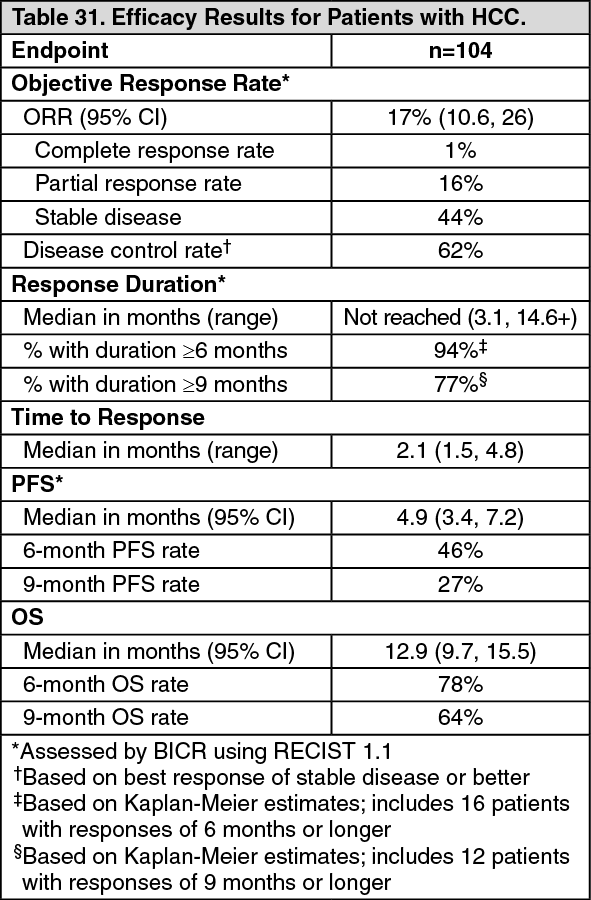 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image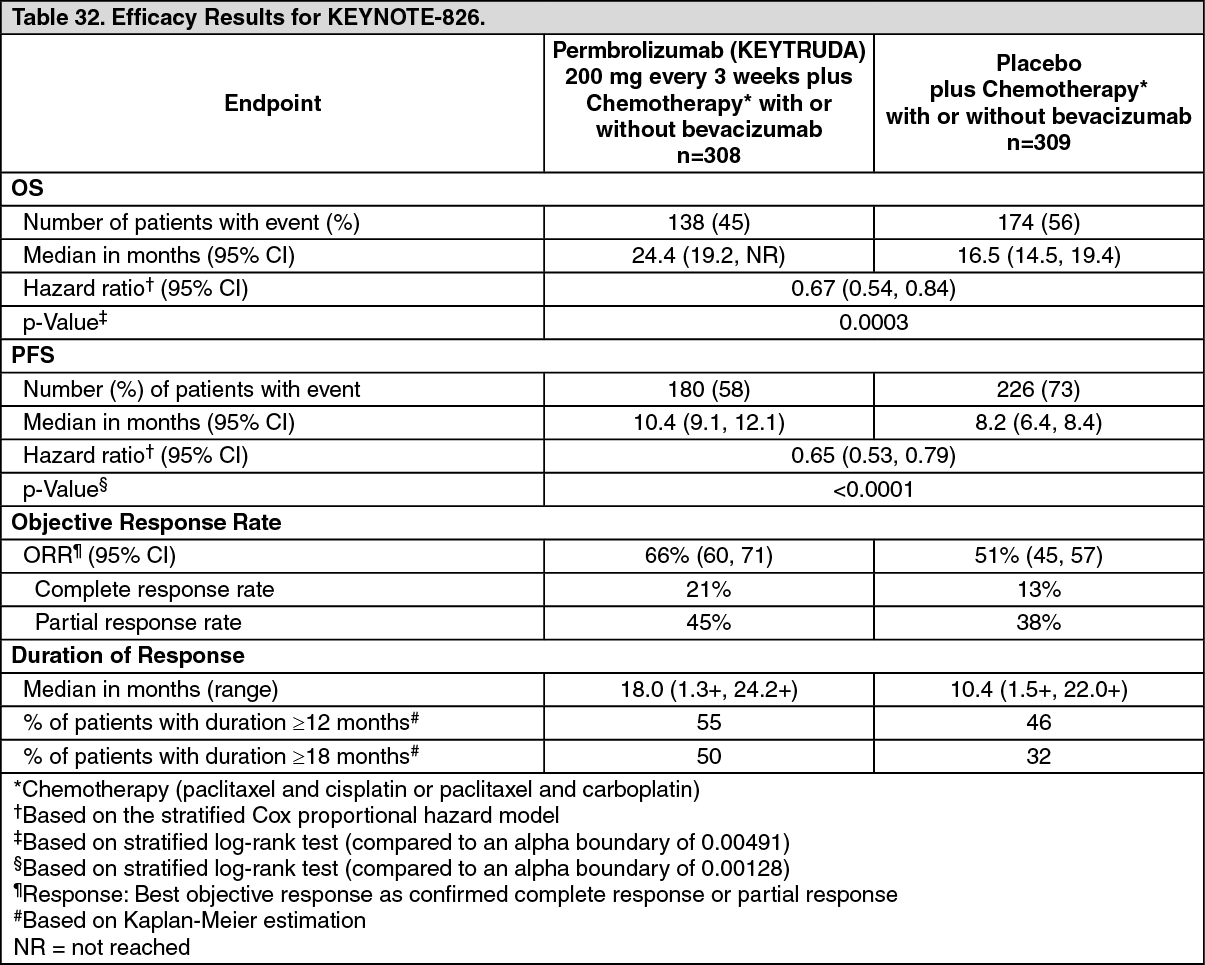 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image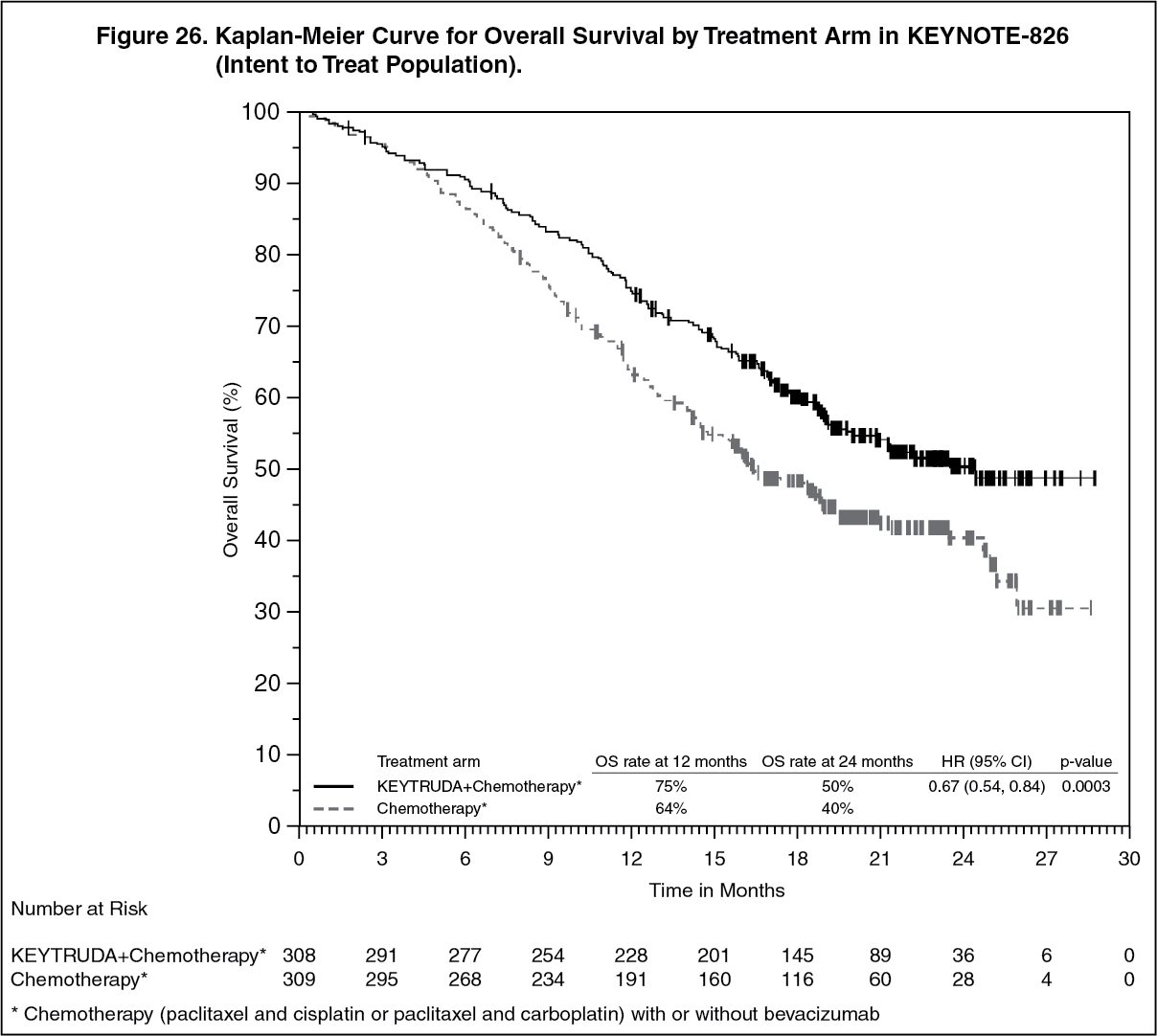 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image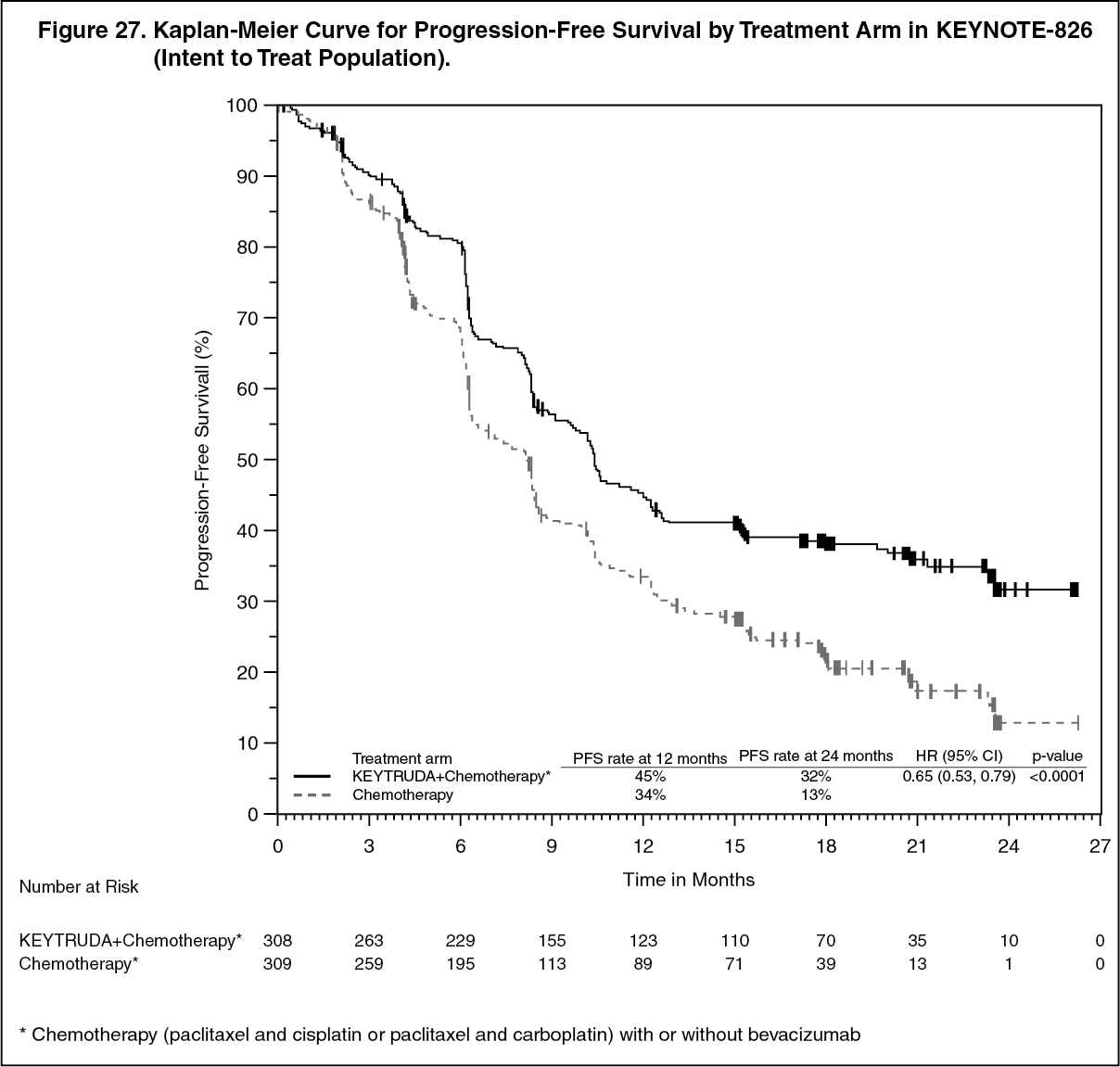 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image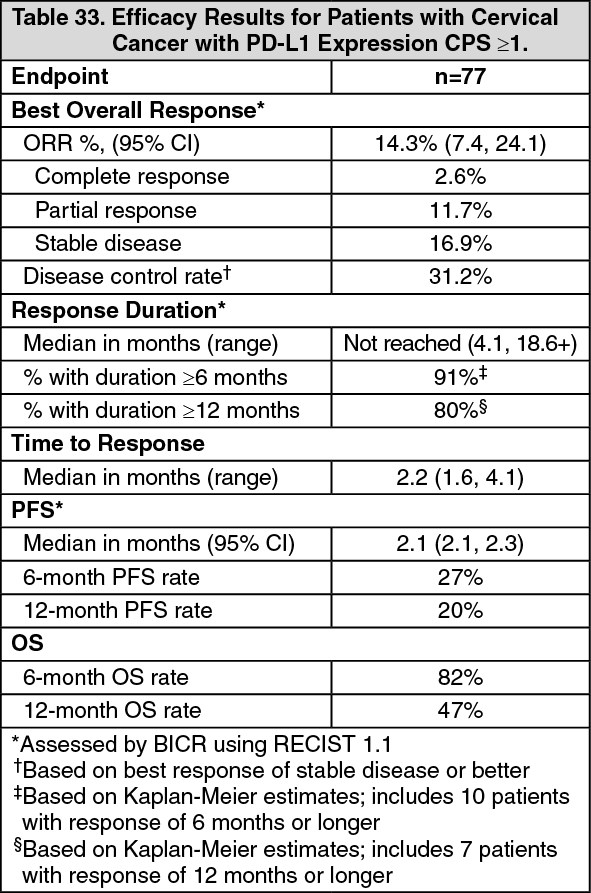 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image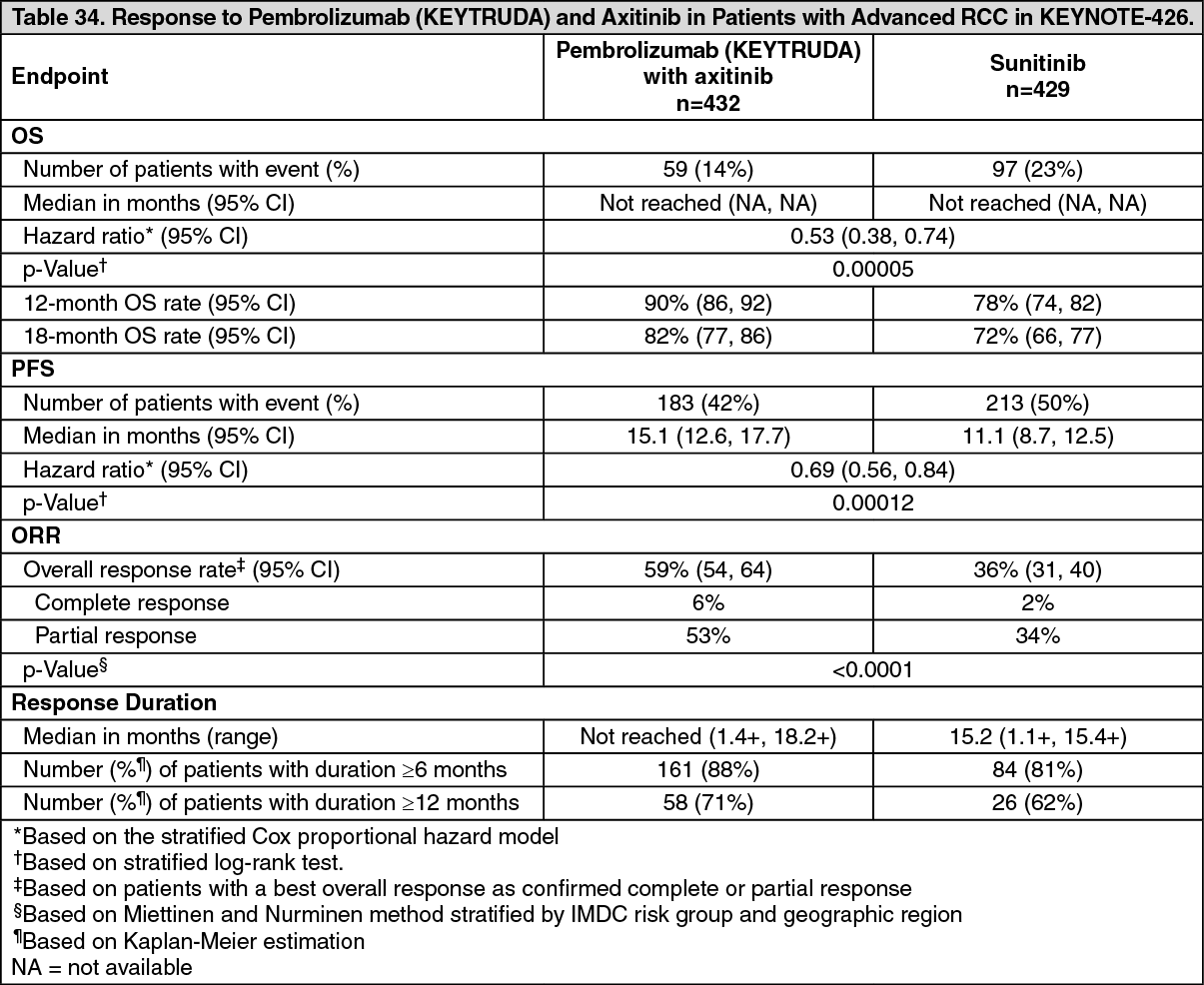 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image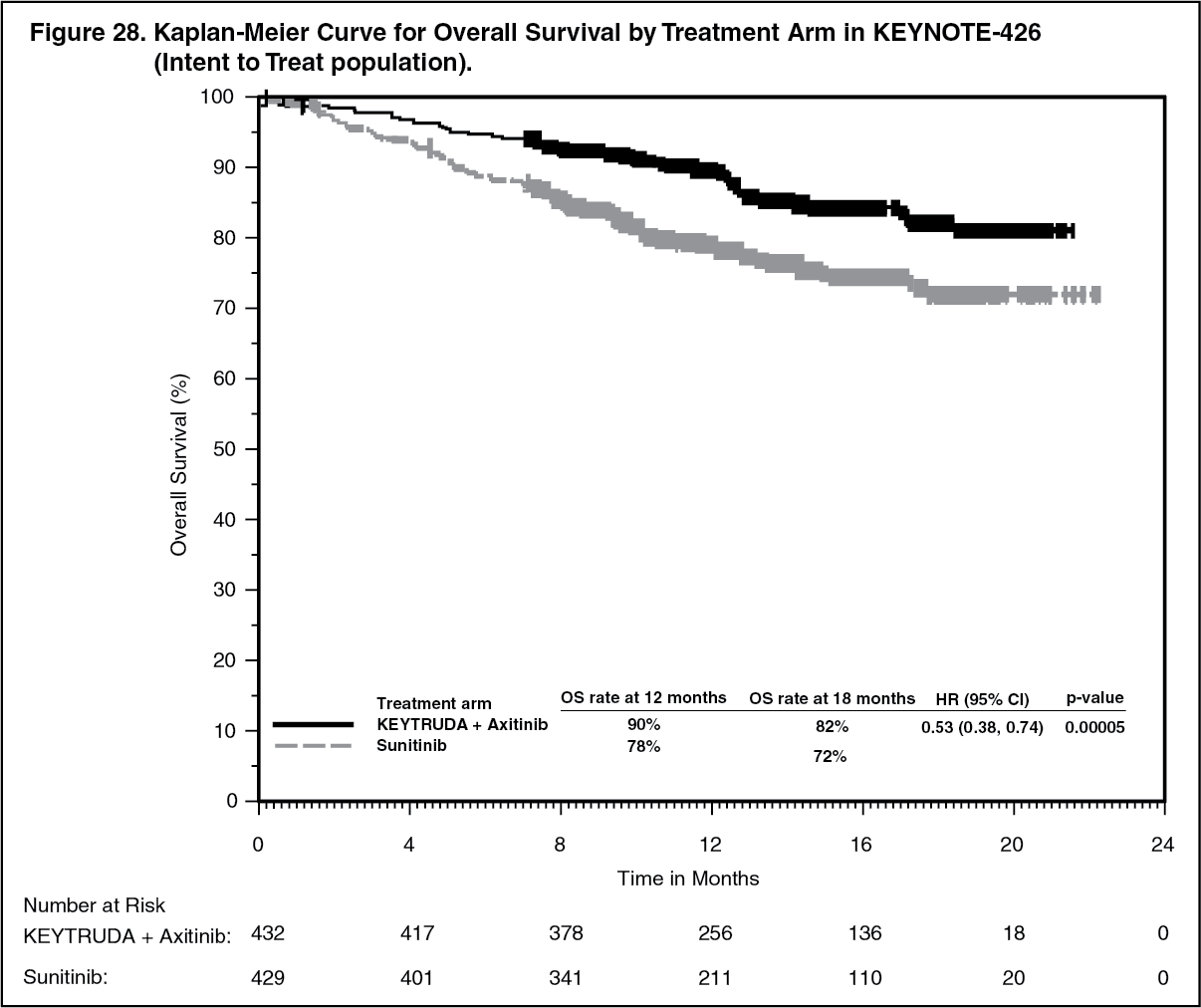 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image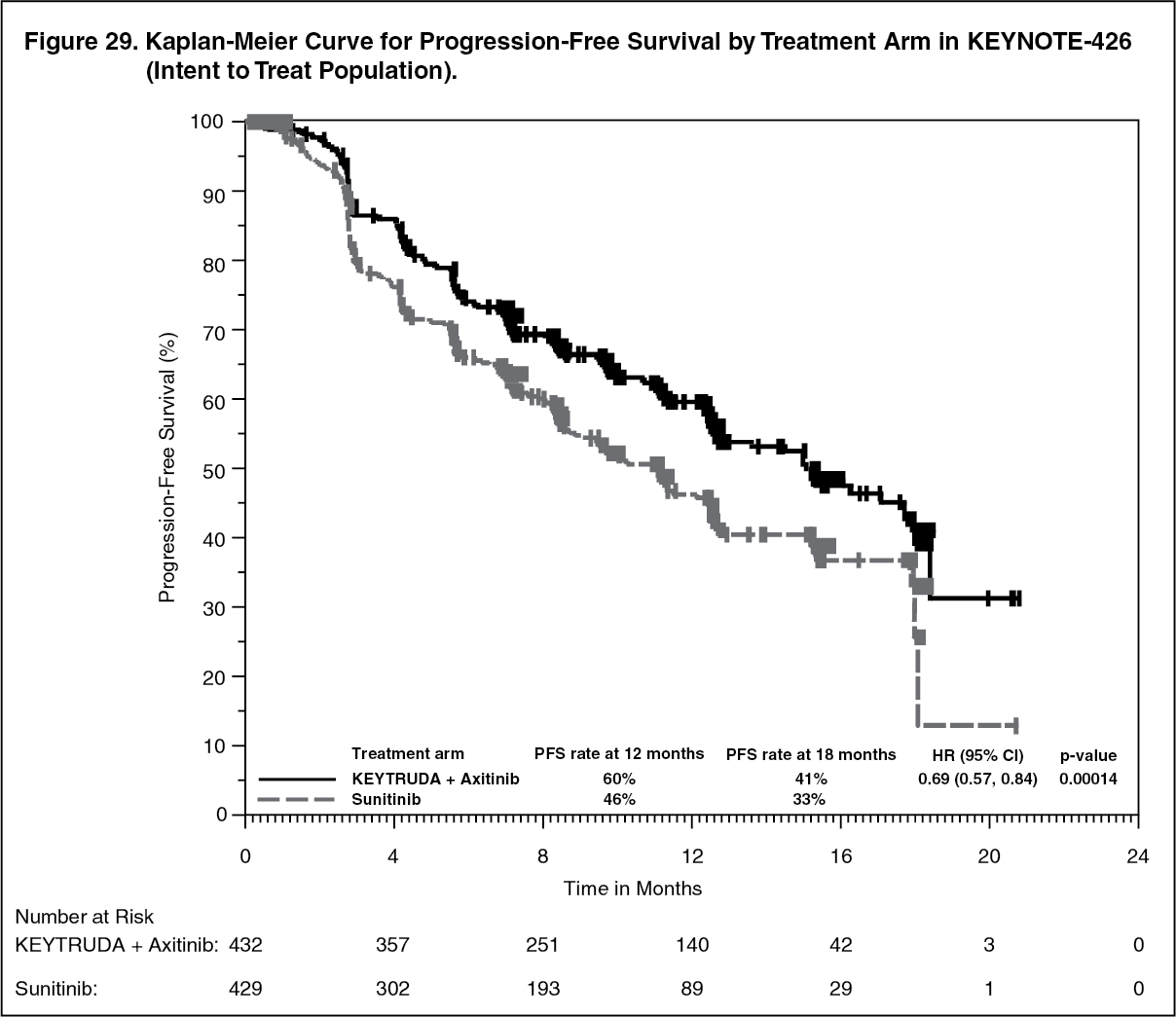 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image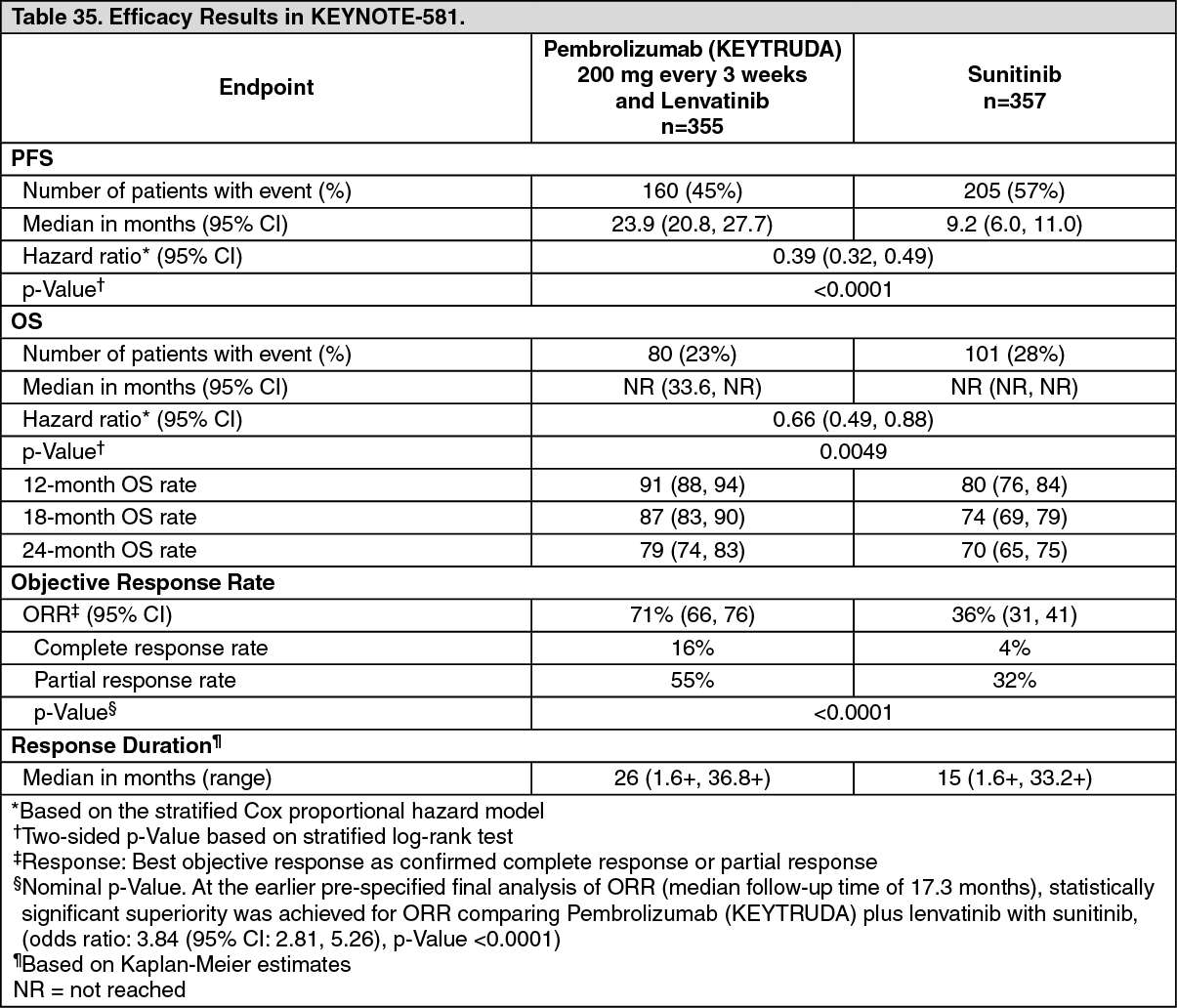 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image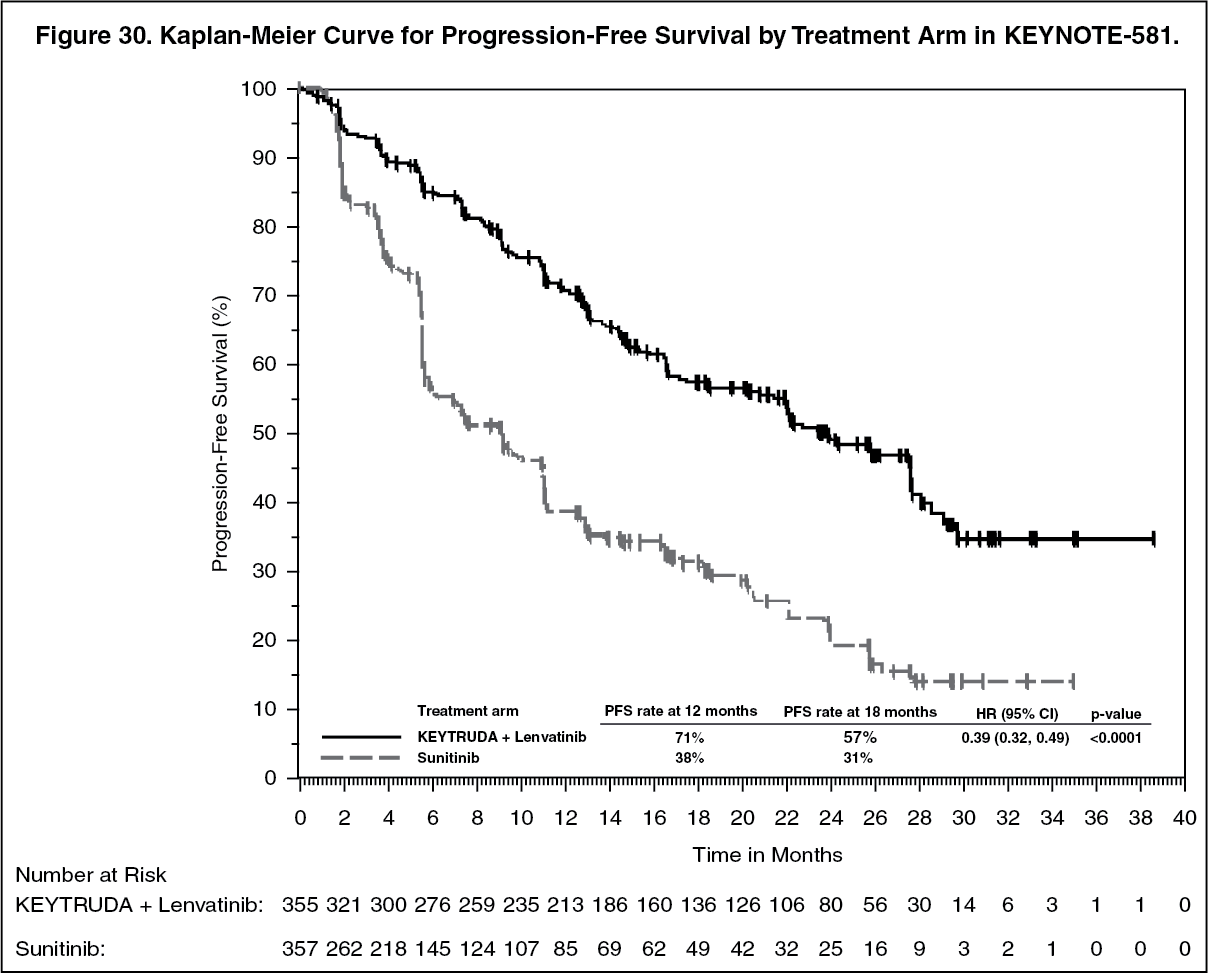 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image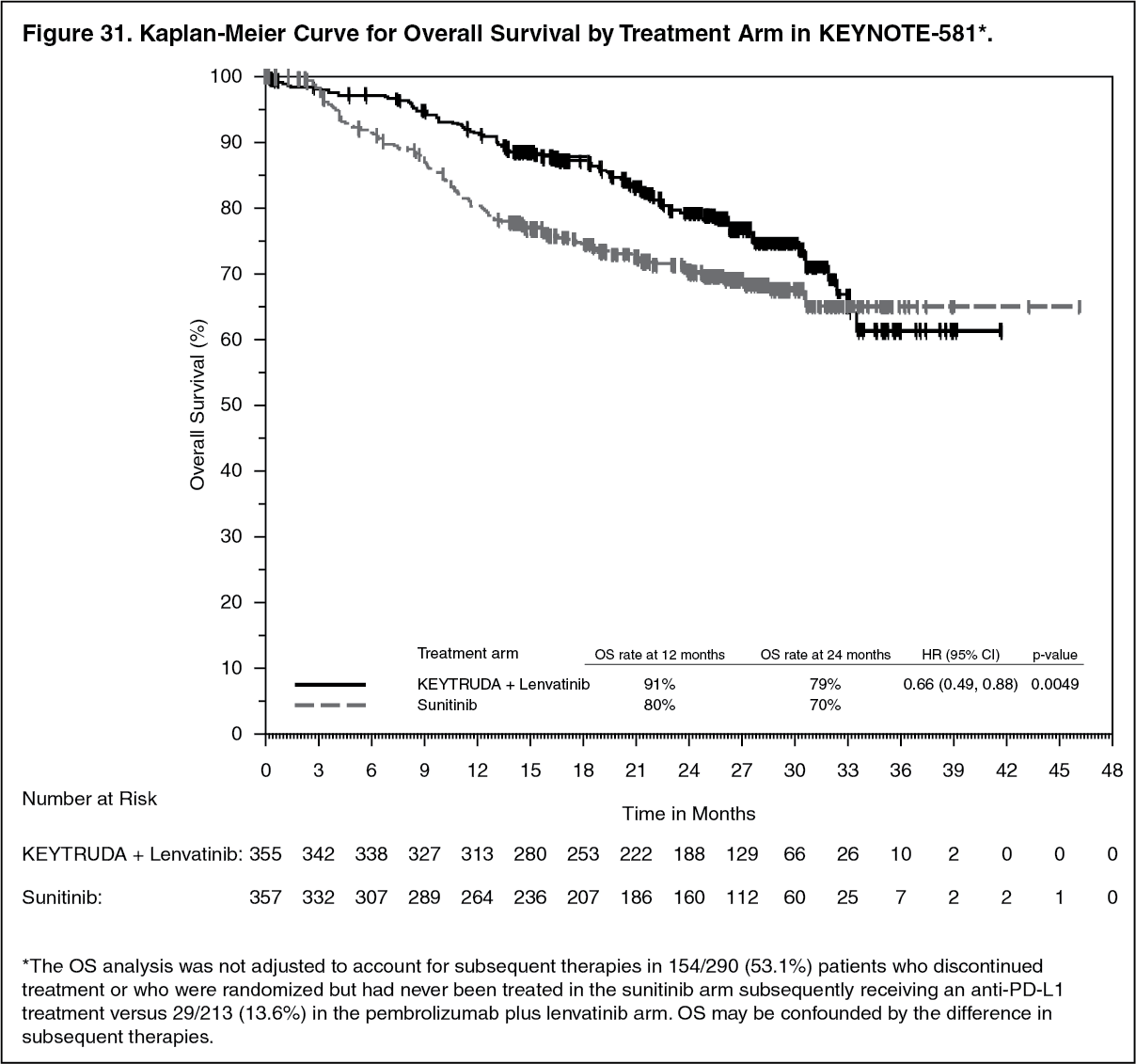 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image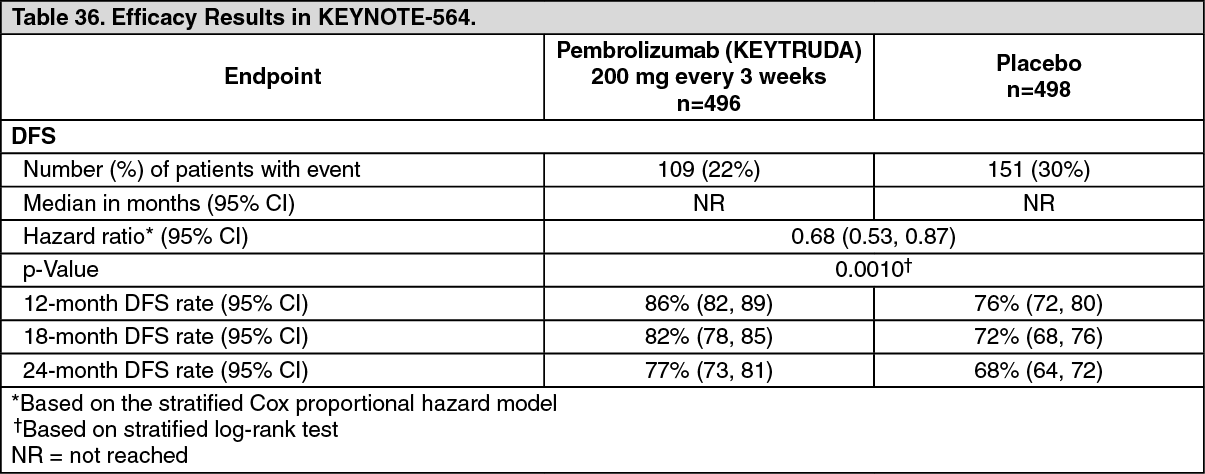 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image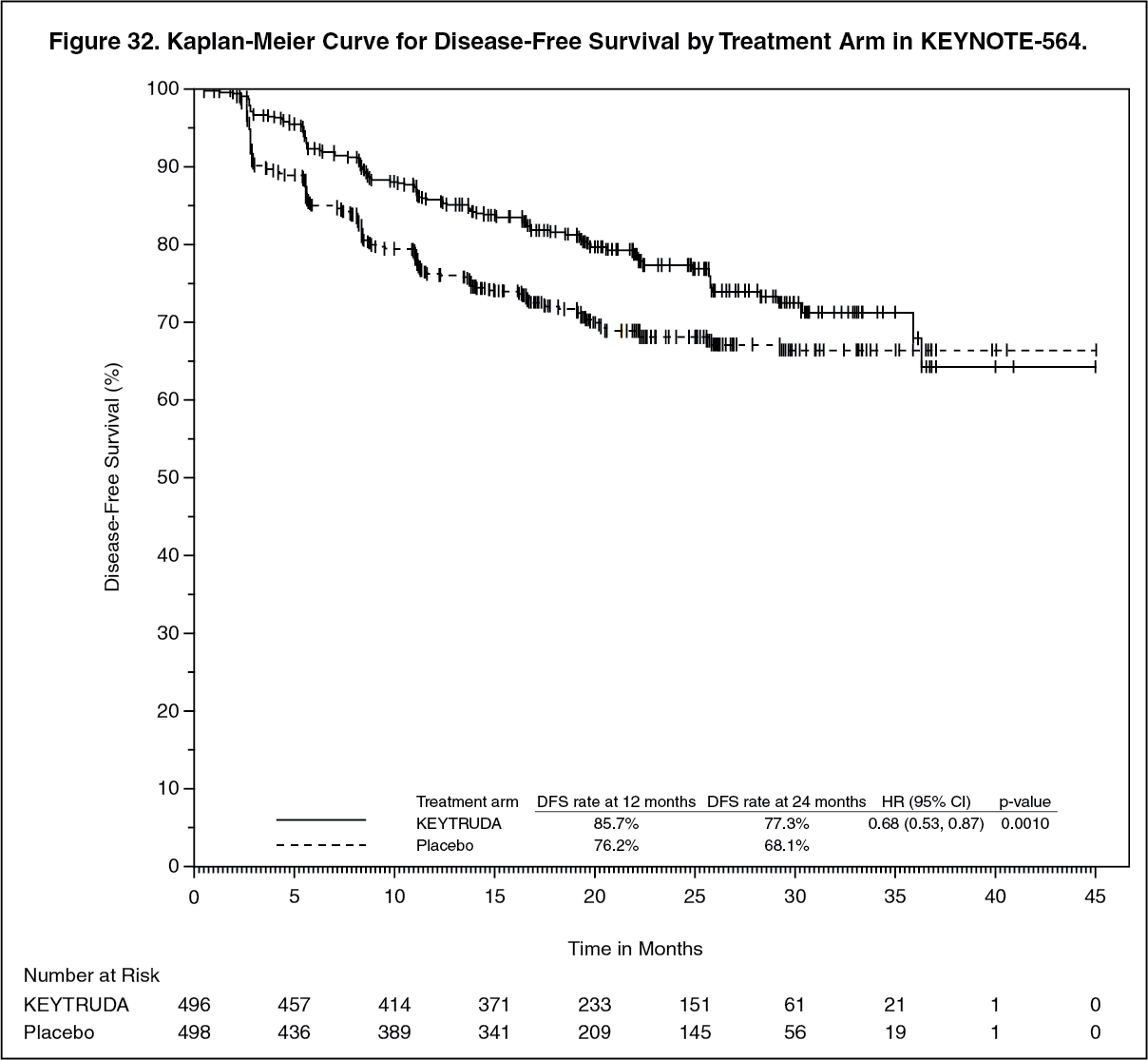 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image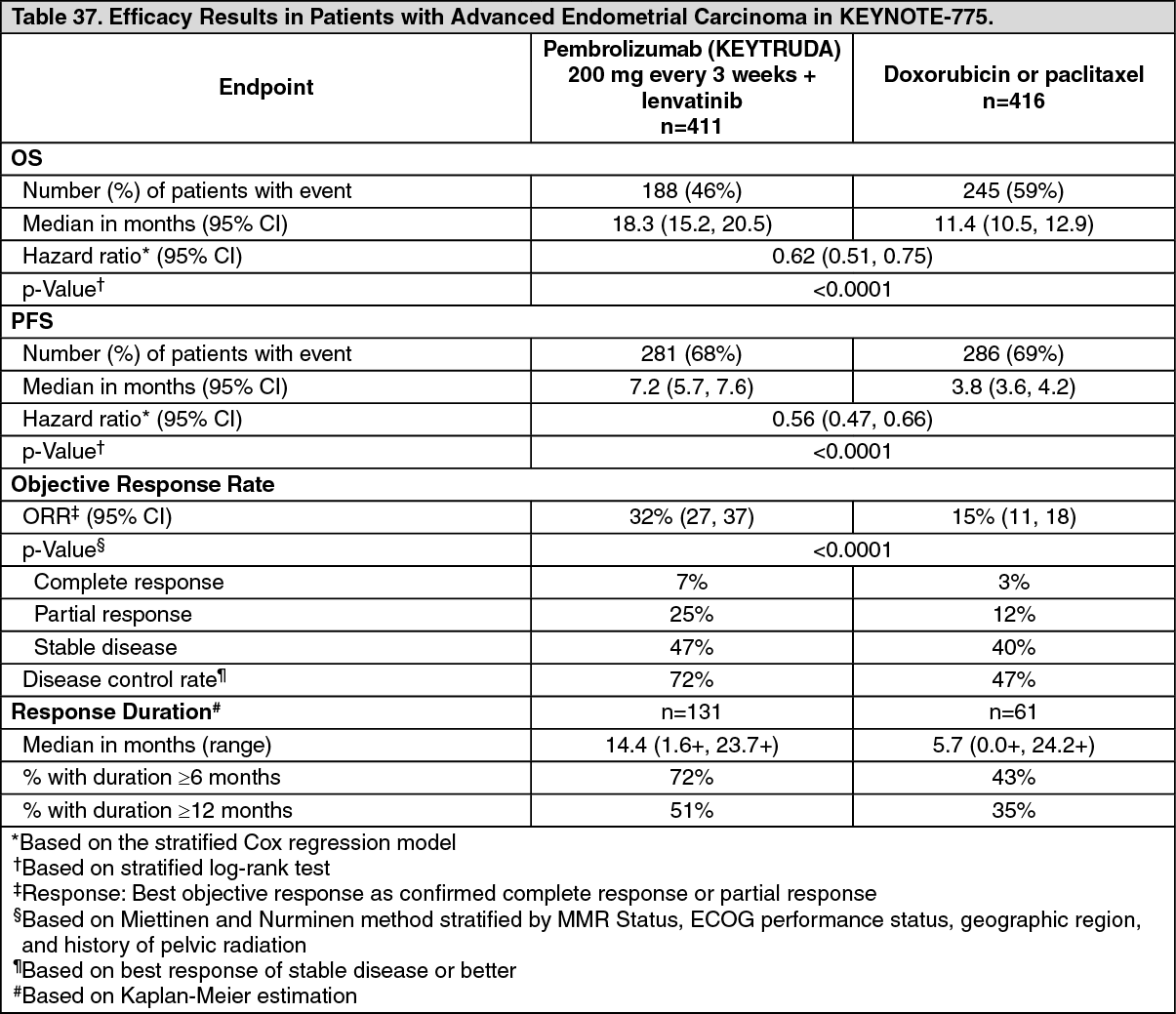 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image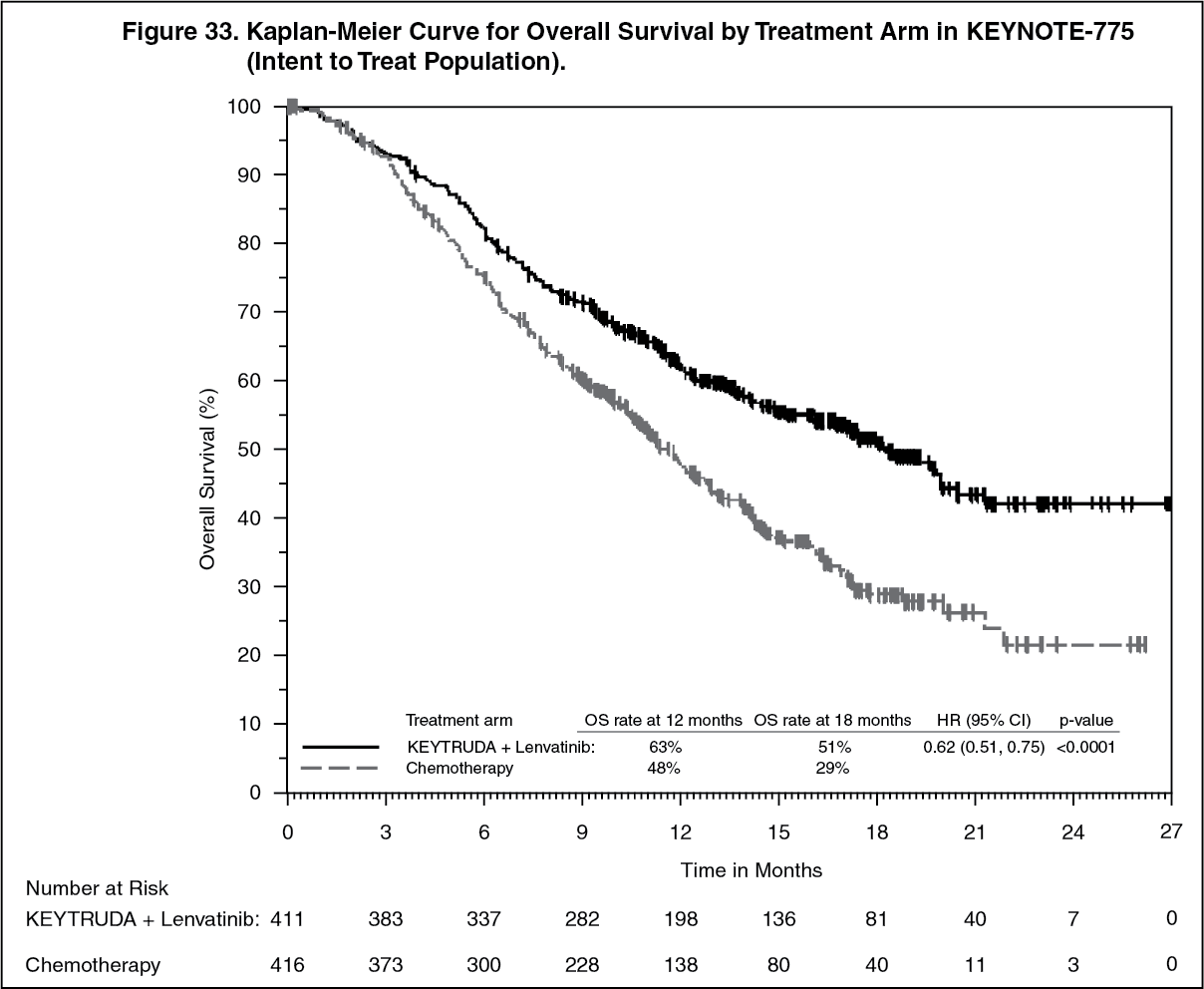 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image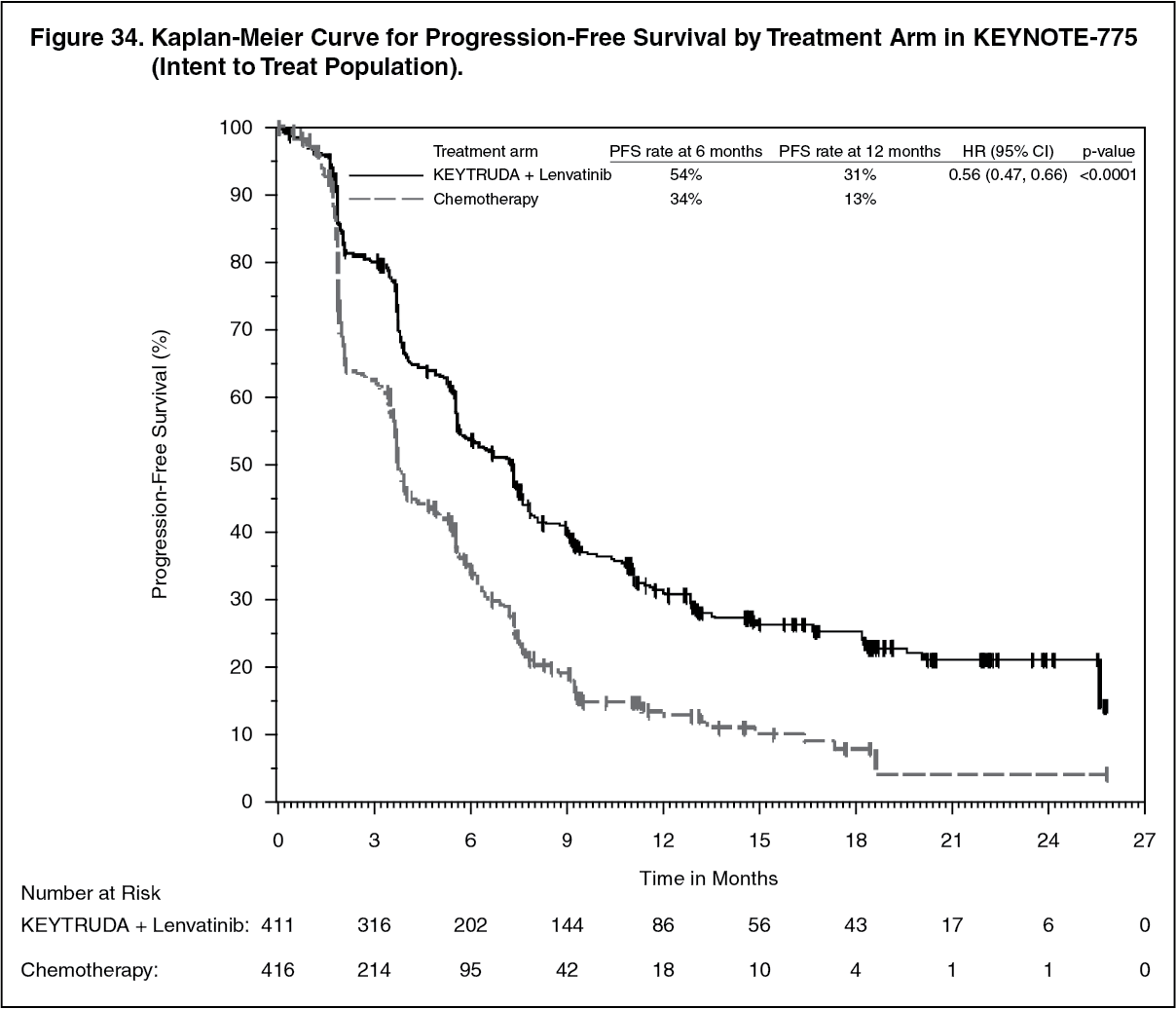 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image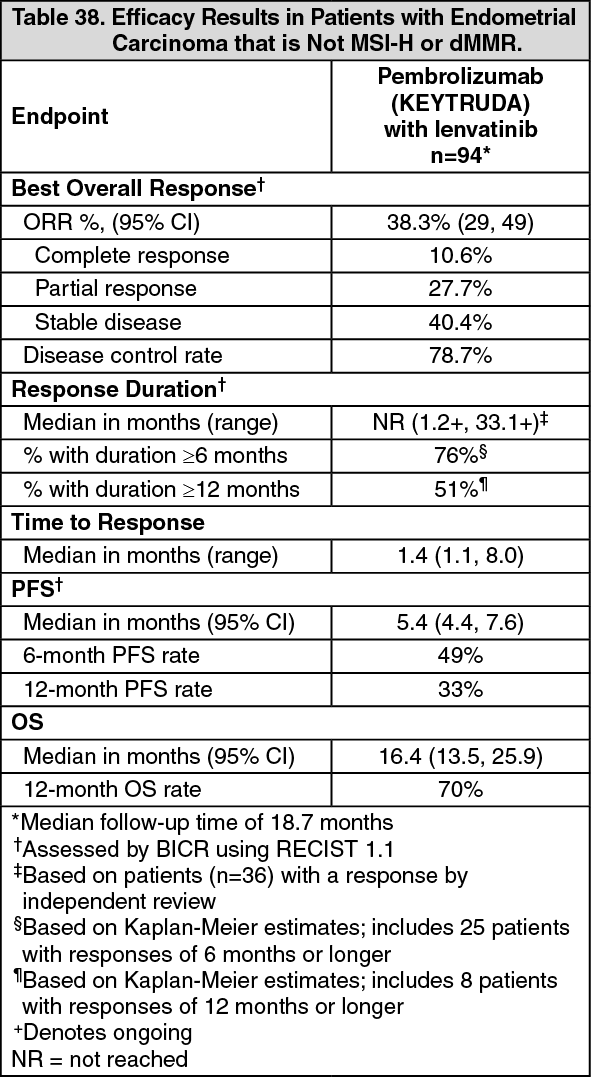 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image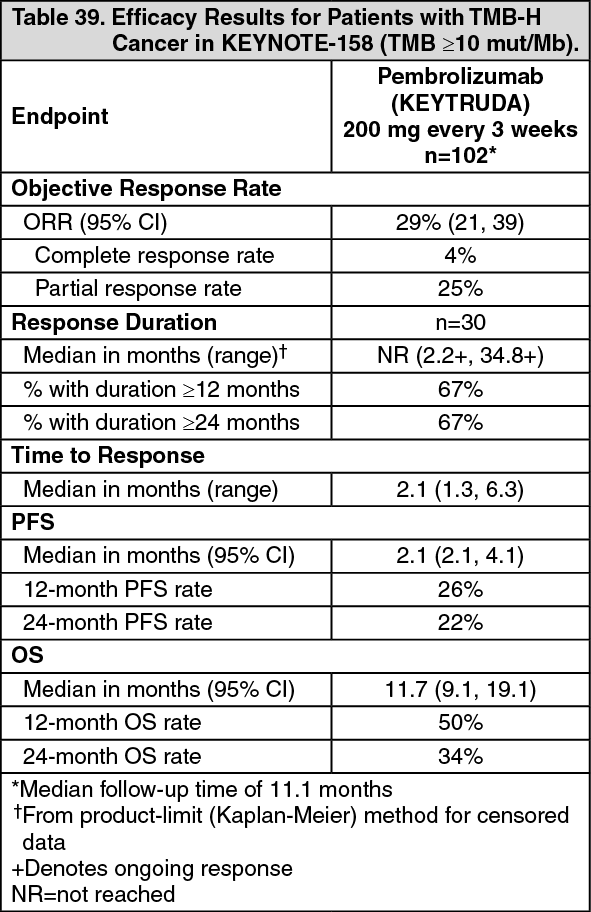 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image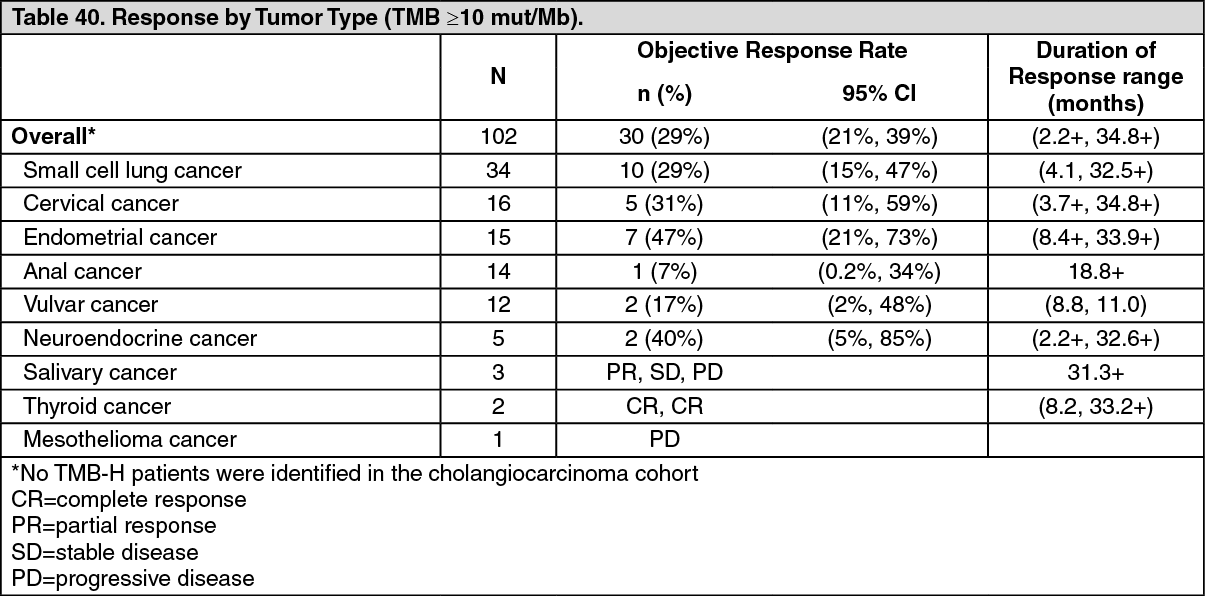 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image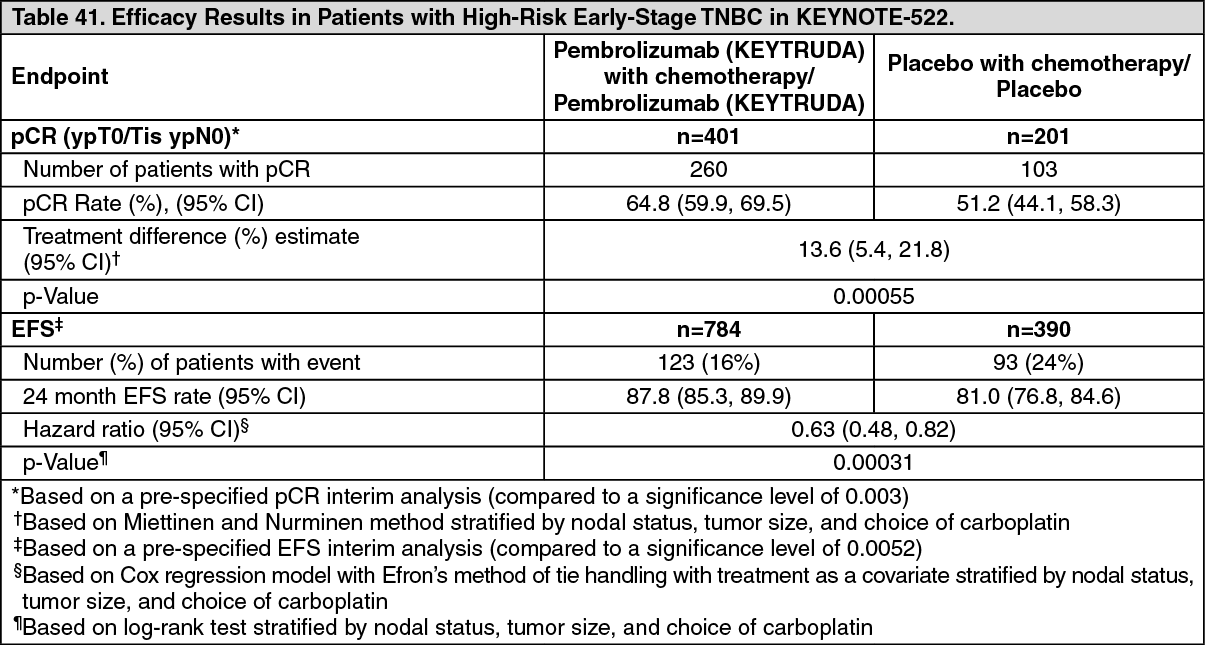 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image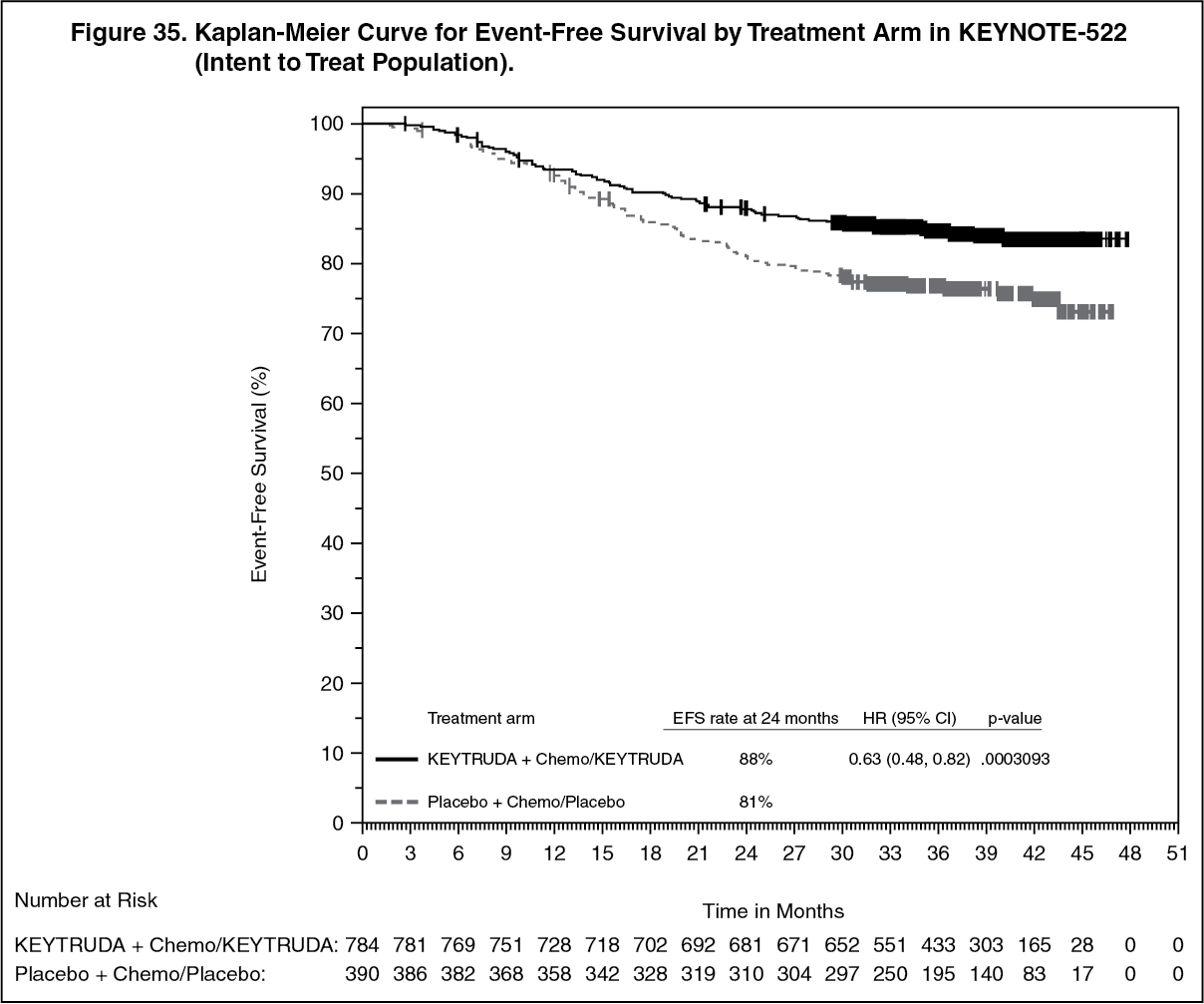 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image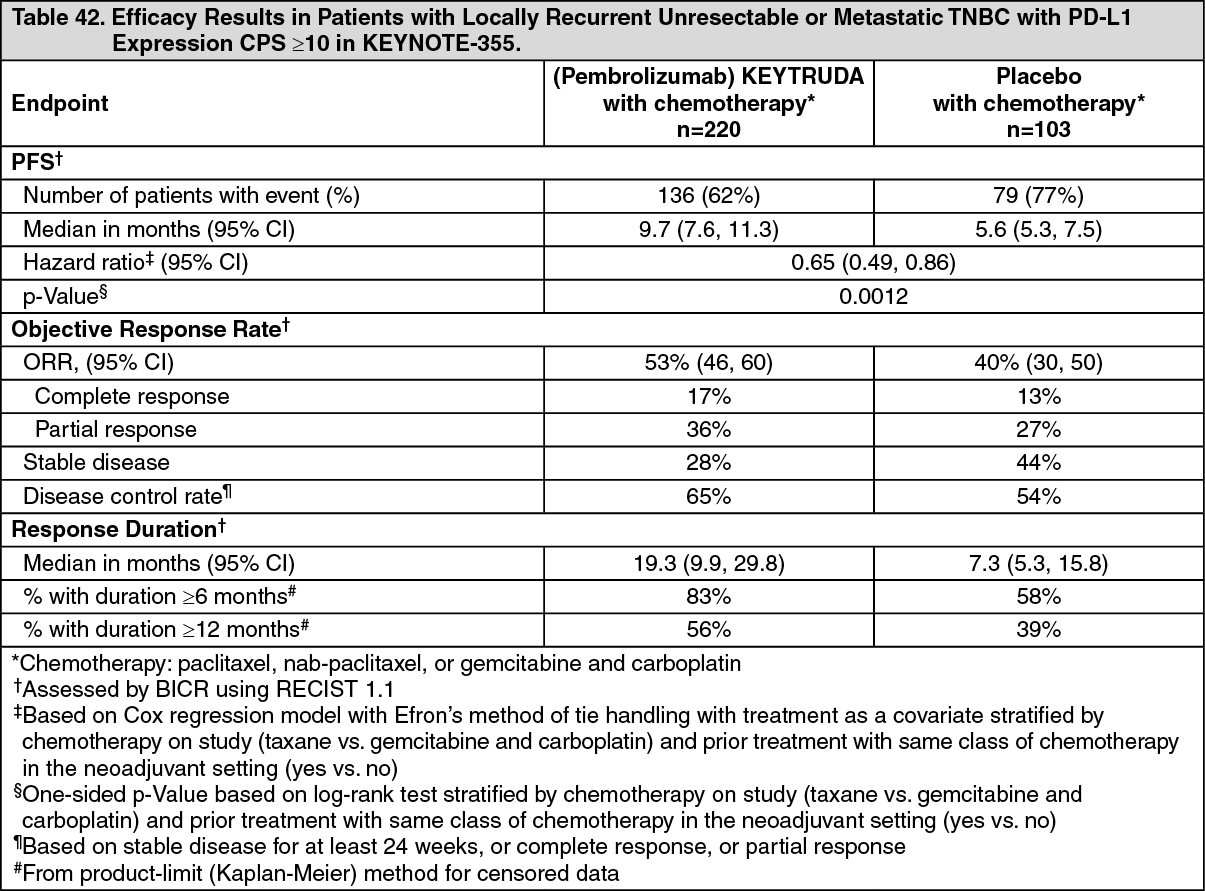 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image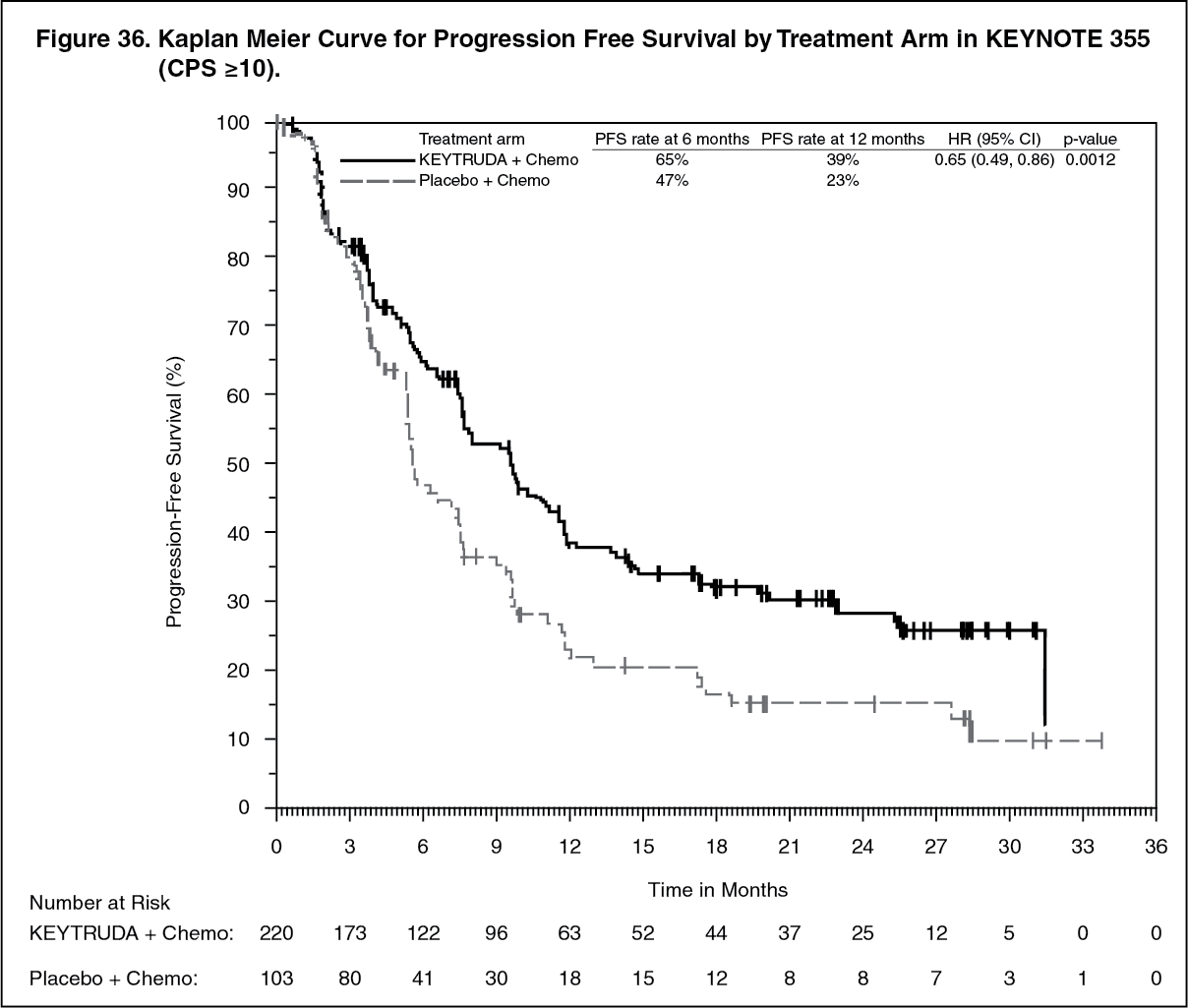 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image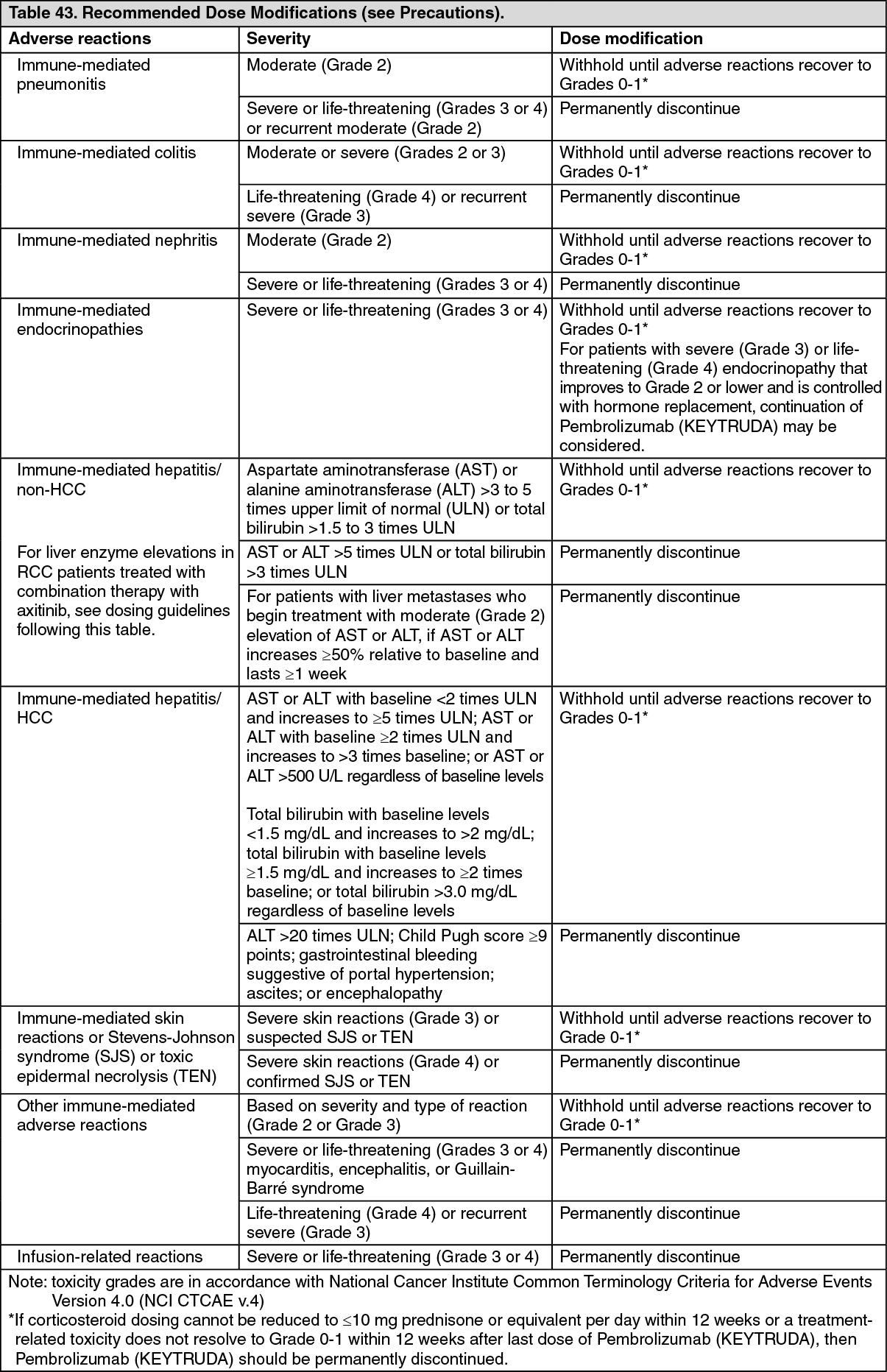 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image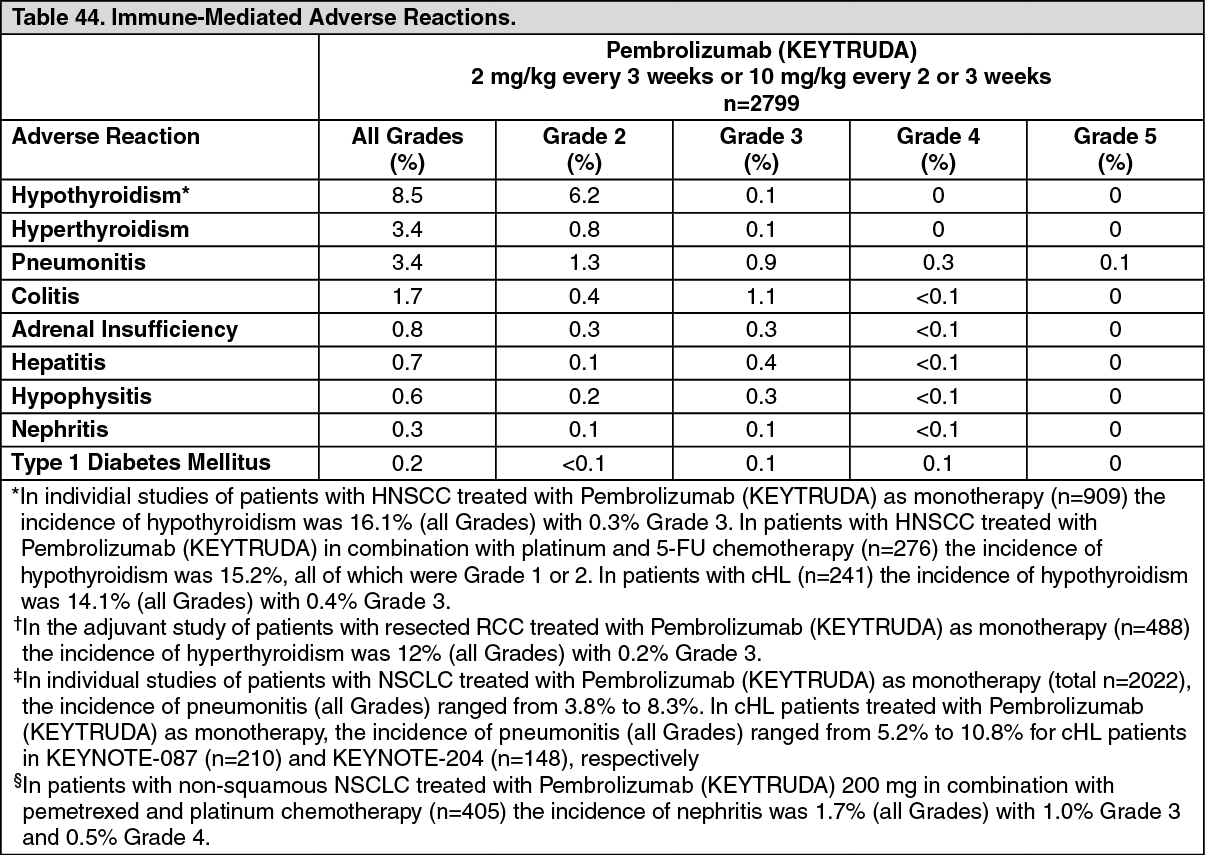 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image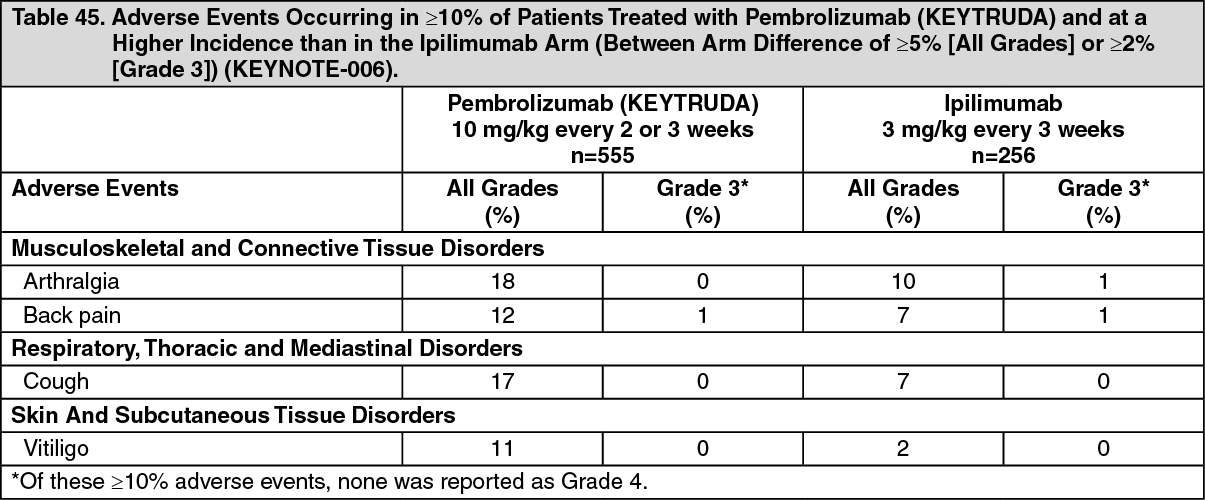 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image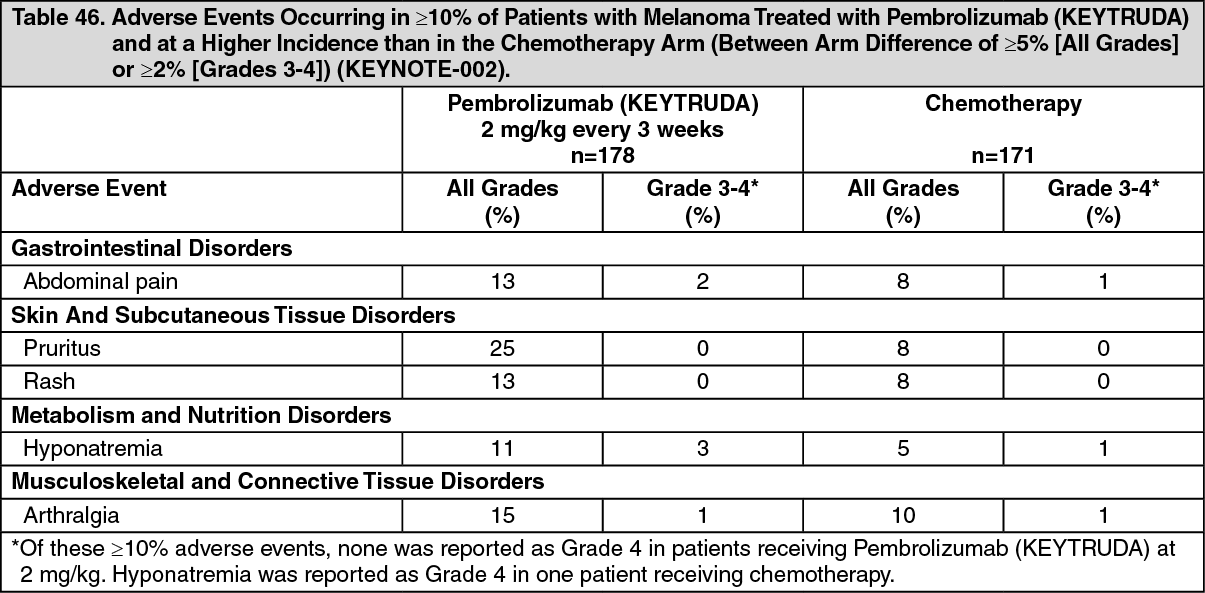 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image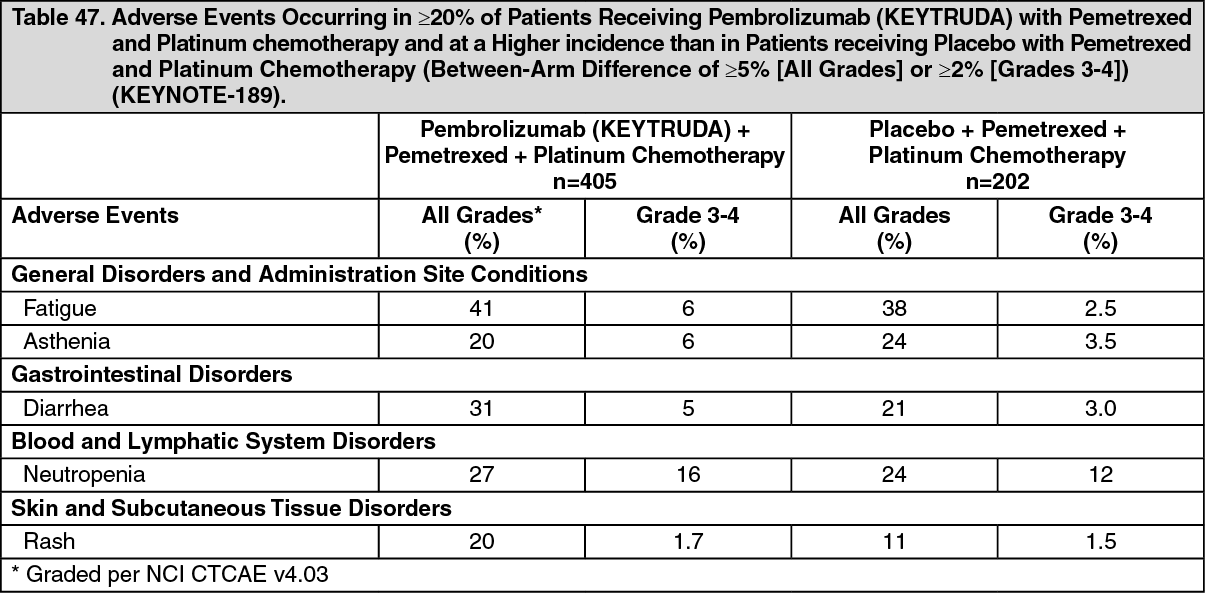 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image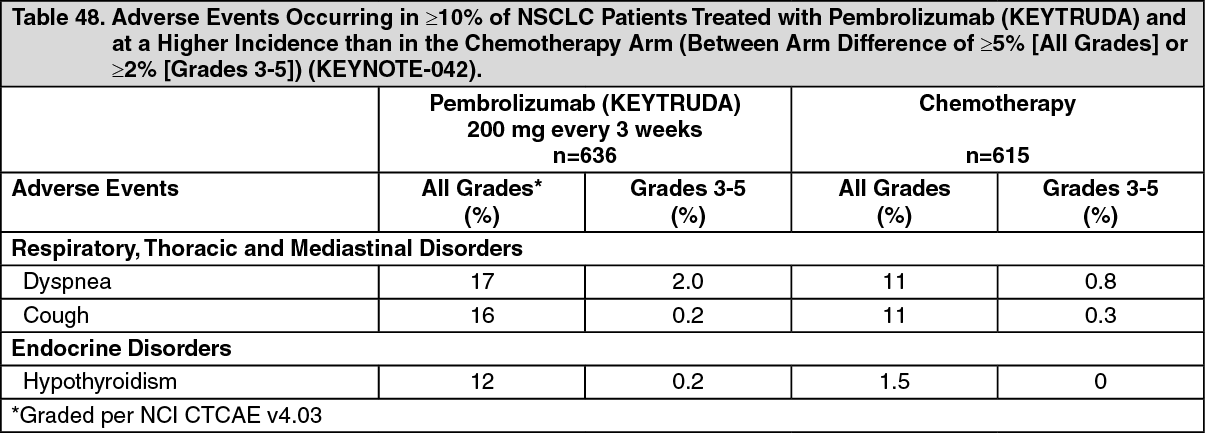 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image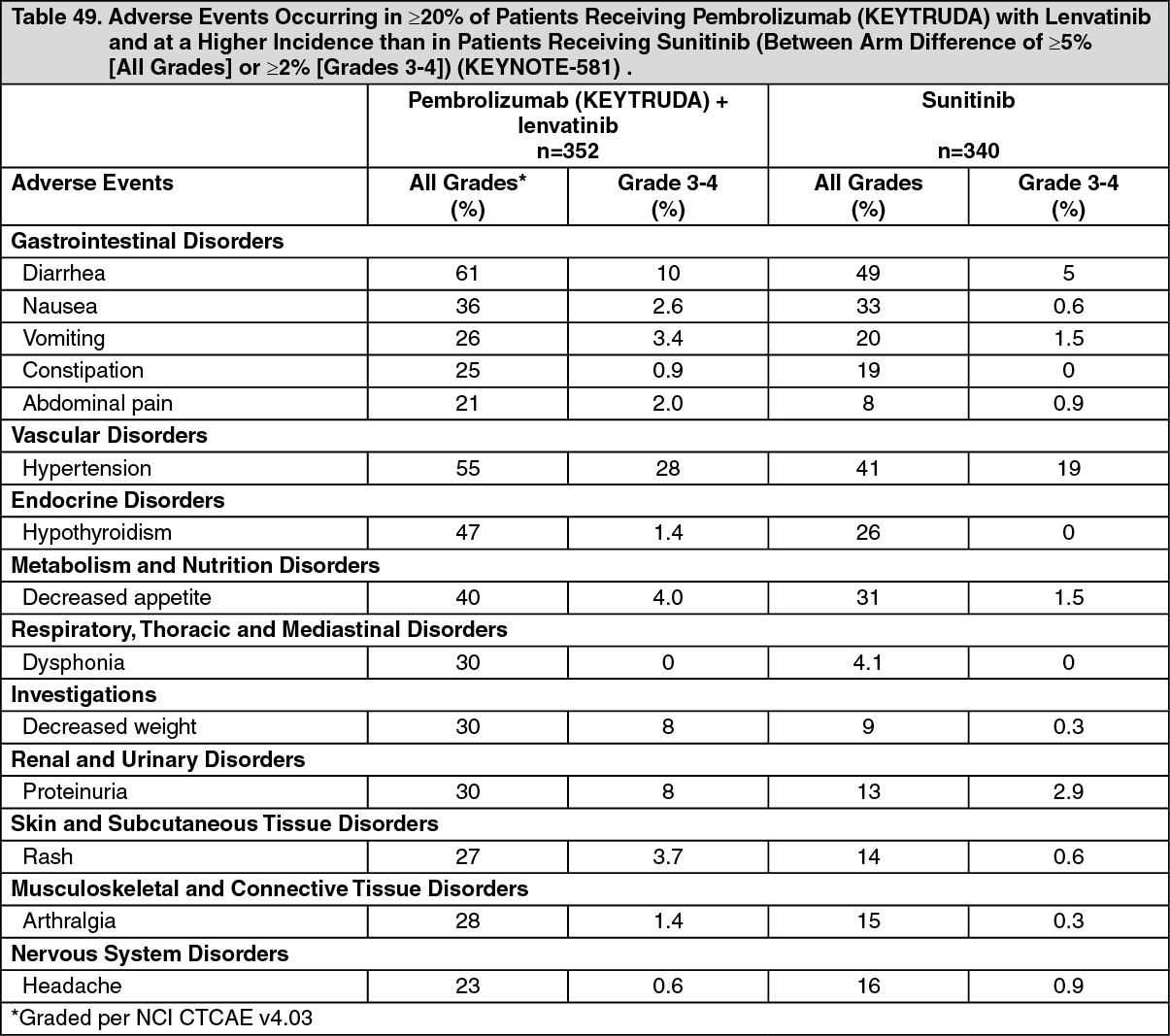 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image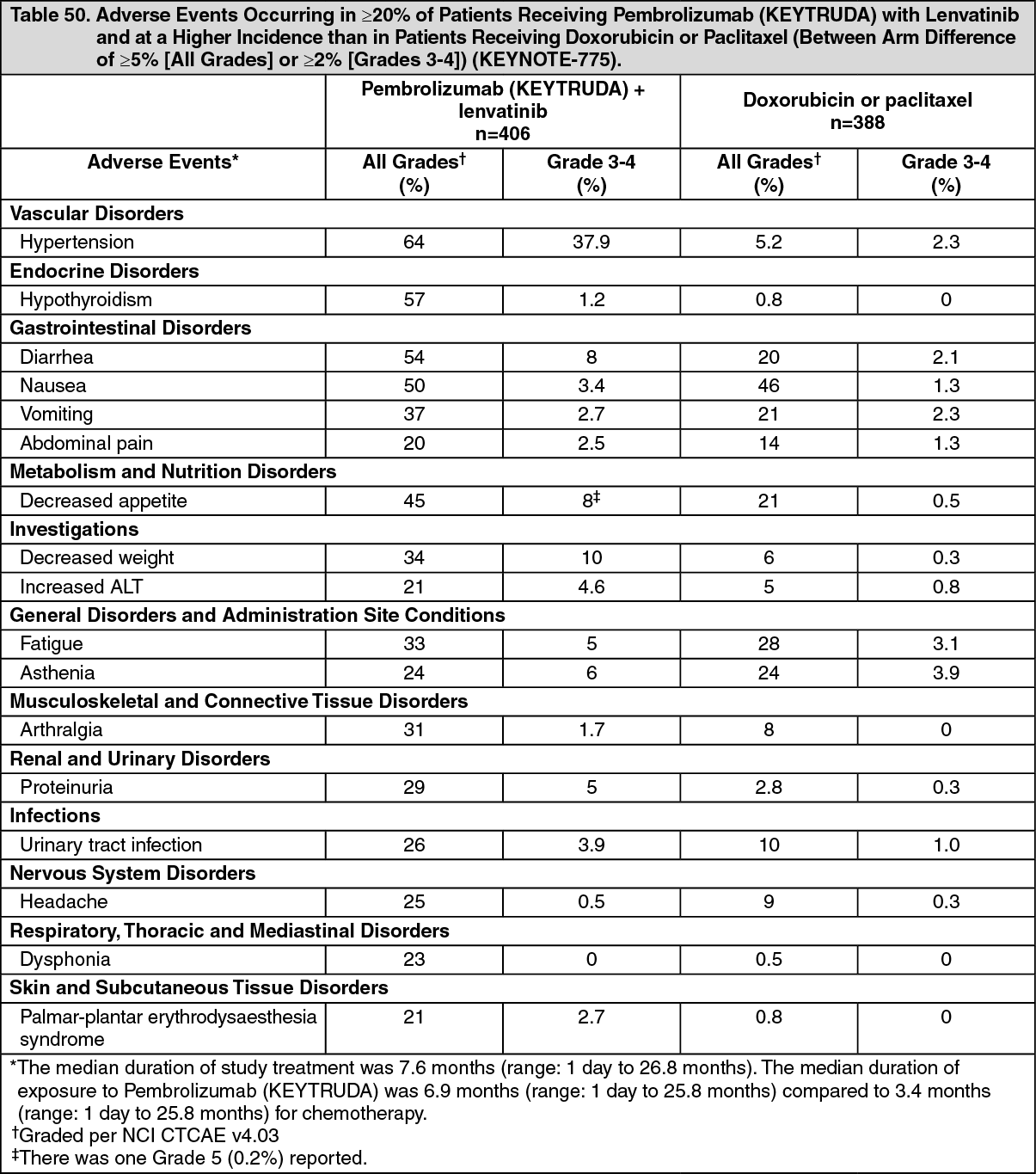 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out
