


 Sign Out
Sign Out


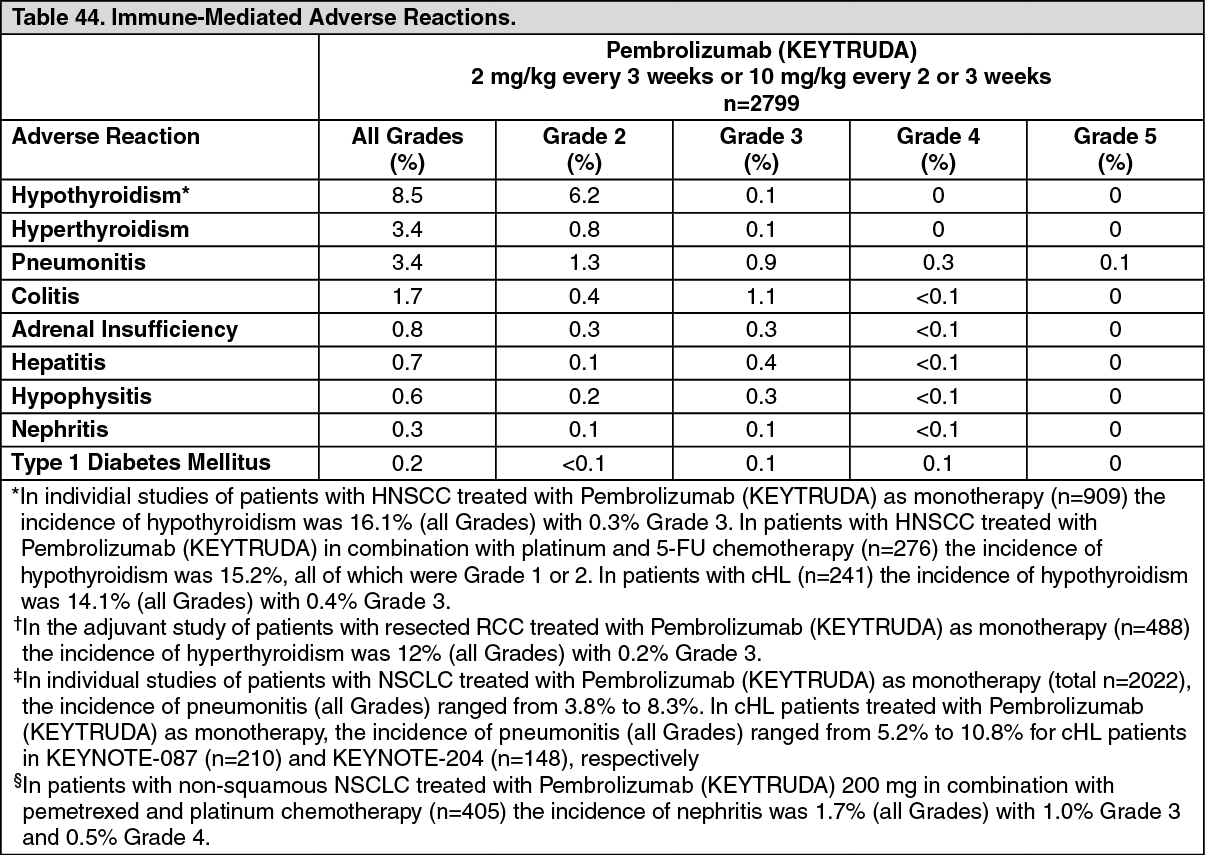
Immune-mediated adverse reactions [see Precautions]: Immune-mediated adverse reactions are presented based on 2799 patients with melanoma and NSCLC. The safety profile was generally similar for patients with melanoma and NSCLC. Table 44 presents the incidence of immune-mediated adverse reactions by Grade that occurred in patients receiving Pembrolizumab (KEYTRUDA). (See Table 44.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageIn individual studies of patients with HNSCC treated with Pembrolizumab (KEYTRUDA) as monotherapy (n=909) the incidence of hypothyroidism was 16.1% (all Grades) with 0.3% Grade 3. In patients with HNSCC treated with Pembrolizumab (KEYTRUDA) in combination with platinum and 5-FU chemotherapy (n=276) the incidence of hypothyroidism was 15.2%, all of which were Grade 1 or 2. In patients with cHL (n=389) the incidence of hypothyroidism was 17% all of which were Grade 1 or 2. In the adjuvant study of patients with resected RCC treated with Pembrolizumab (KEYTRUDA) as monotherapy (n=488) the incidence of hypothyroidism was 21% (all Grades) with 0.2% Grade 3. † In the adjuvant study of patients with resected RCC treated with Pembrolizumab (KEYTRUDA) as monotherapy (n=488) the incidence of hyperthyroidism was 12% (all Grades) with 0.2% Grade 3. ‡ In individual studies of patients with NSCLC treated with Pembrolizumab (KEYTRUDA) as monotherapy (total n=2022), the incidence of pneumonitis (all Grades) ranged from 3.8% to 8.3%. In cHL patients treated with Pembrolizumab (KEYTRUDA) as monotherapy, the incidence of pneumonitis (all Grades) ranged from 5.2% to 10.8% for cHL patients in KEYNOTE-087 (n=210) and KEYNOTE-204 (n=148), respectively. § In patients with non-squamous NSCLC treated with Pembrolizumab (KEYTRUDA) 200 mg in combination with pemetrexed and platinum chemotherapy (n=405) the incidence of nephritis was 1.7% (all Grades) with 1.0% Grade 3 and 0.5% Grade 4.
Endocrinopathies: The median time to onset of adrenal insufficiency was 5.3 months (range 26 days to 16.6 months). The median duration was not reached (range 4 days to 1.9+ years). Adrenal insufficiency led to discontinuation of Pembrolizumab (KEYTRUDA) in 1 (<0.1%) patient. Adrenal insufficiency resolved in 5 patients. The median time to onset of hypophysitis was 3.7 months (range 1 day to11.9 months). The median duration was 4.7 months (range 8+ days to 12.7+ months). Hypophysitis led to discontinuation of Pembrolizumab (KEYTRUDA) in 4 (0.1%) patients. Hypophysitis resolved in 7 patients. The median time to onset of hyperthyroidism was 1.4 months (range 1 day to 21.9 months). The median duration was 2.1 months (range 3 days to 15.0+ months). Hyperthyroidism led to discontinuation of Pembrolizumab (KEYTRUDA) in 2 (<0.1%) patients. Hyperthyroidism resolved in 71 patients. The median time to onset of hypothyroidism was 3.5 months (range 1 day to 18.9 months). The median duration was not reached (range 2 days to 27.7+ months). One (<0.1%) patient discontinued Pembrolizumab (KEYTRUDA) due to hypothyroidism.
Pneumonitis: The median time to onset of pneumonitis was 3.3 months (range 2 days to 19.3 months). The median duration was 1.5 months (range 1 day to 17.2+ months). Pneumonitis led to discontinuation of Pembrolizumab (KEYTRUDA) in 36 (1.3%) patients. Pneumonitis resolved in 55 patients. Colitis: The median time to onset of colitis was 3.5 months (range 10 days to 16.2 months). The median duration was 1.3 months (range 1 day to 8.7+ months).
Colitis: led to discontinuation of Pembrolizumab (KEYTRUDA) in 15 (0.5%) patients. Colitis resolved in 41 patients.
Hepatitis: The median time to onset of hepatitis was 1.3 months (range 8 days to 21.4 months). The median duration was 1.8 months (range 8 days to 20.9+ months). Hepatitis led to discontinuation of Pembrolizumab (KEYTRUDA) in 6 (0.2%) patients. Hepatitis resolved in 15 patients.
Nephritis: The median time to onset of nephritis was 5.1 months (range 12 days to 12.8 months). The median duration was 3.3 months (range 12 days to 8.9+ months). Nephritis led to discontinuation of Pembrolizumab (KEYTRUDA) in 3 (0.1%) patients. Nephritis resolved in 5 patients.
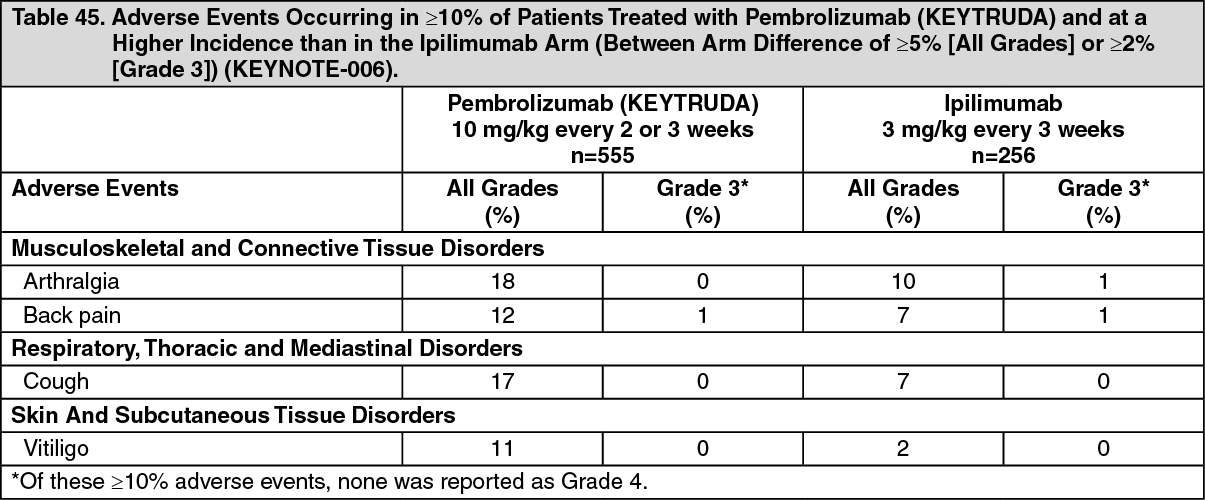
Other adverse events: Melanoma: Table 45 summarizes the adverse events that occurred in at least 10% of patients with melanoma treated with Pembrolizumab (KEYTRUDA) in KEYNOTE-006. The most common adverse events (reported in at least 15% of patients) were arthralgia and cough. (See Table 45.)
 Click on icon to see table/diagram/image
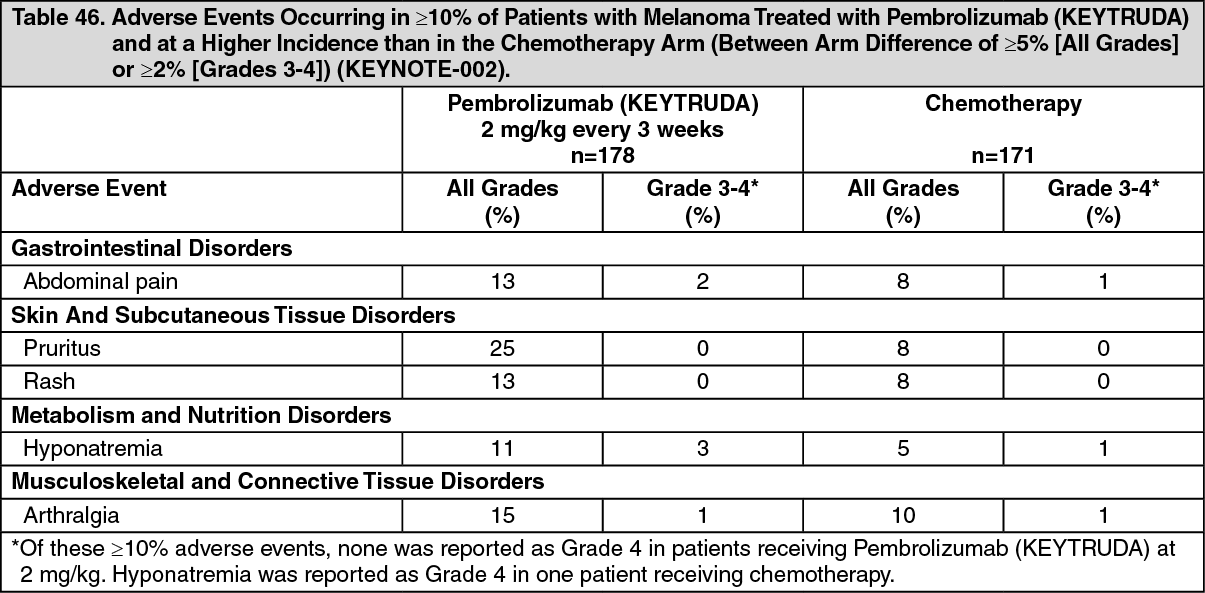
Click on icon to see table/diagram/imageTable 46 summarizes the adverse events that occurred in at least 10% of patients with melanoma treated with Pembrolizumab (KEYTRUDA) at a dose of 2 mg/kg in KEYNOTE-002. The most common adverse event (reported in at least 20% of patients) was pruritus. (See Table 46.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageOverall, the safety profile was similar across all doses and between patients previously treated with ipilimumab and patients naïve to treatment with ipilimumab.
Resected Melanoma: Among the 969 patients with resected melanoma enrolled in KEYNOTE-716 and 1019 patients with resected melanoma enrolled in KEYNOTE-054, the adverse reactions were generally similar to those occurring in patients with unresectable or metastatic melanoma or NSCLC.
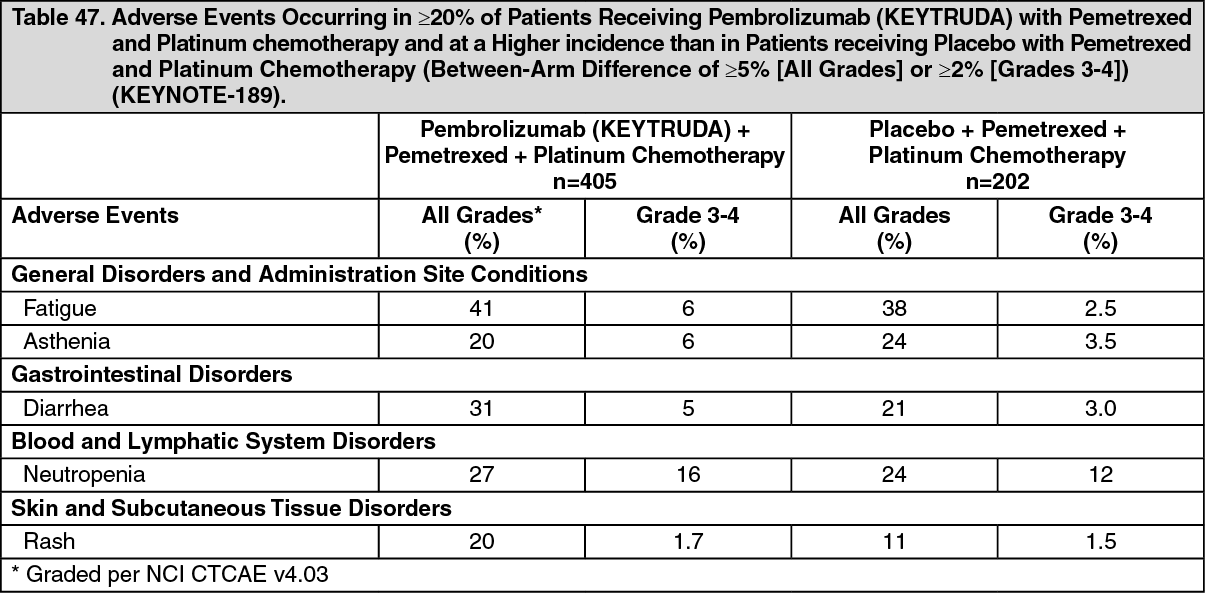
Non-Small Cell Lung Carcinoma: Combination Therapy: Table 47 summarizes the adverse events that occurred in at least 20% of patients treated with Pembrolizumab (KEYTRUDA), pemetrexed, and platinum chemotherapy in KEYNOTE-189. Adverse events occurring in previously untreated patients with NSCLC receiving Pembrolizumab (KEYTRUDA) in combination with carboplatin and either paclitaxel or nab-paclitaxel in KEYNOTE-407 were generally similar to those occurring in patients with KEYNOTE-189 with the exception of alopecia (46%) and arthralgia (21%). (See Table 47.)
 Click on icon to see table/diagram/image
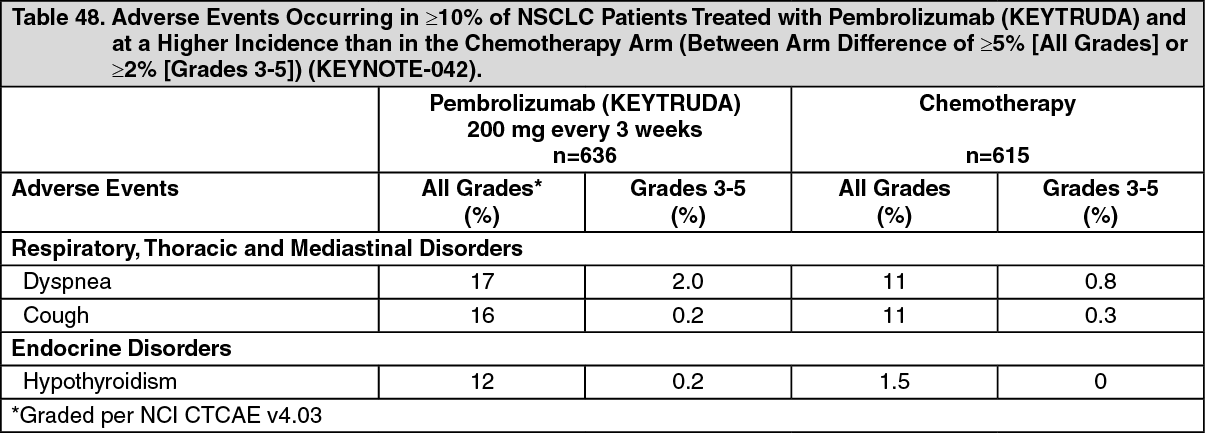
Click on icon to see table/diagram/imageMonotherapy: Table 48 summarizes the adverse events that occurred in at least 10% of previously untreated patients with NSCLC receiving Pembrolizumab (KEYTRUDA) in KEYNOTE-042. The most common adverse events (reported in at least 15% of patients) were dyspnea and cough. Adverse events occurring in previously untreated patients with NSCLC receiving Pembrolizumab (KEYTRUDA) in KEYNOTE-024 and previously treated patients in KEYNOTE-010 were generally similar to those occurring in patients in KEYNOTE-042. (See Table 48.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageOther Cancers: Monotherapy: Adverse events occurring in patients with SCLC, HNSCC, cHL, urothelial carcinoma, gastric cancer, esophageal cancer, MSI-H cancer, CRC, HCC, cervical cancer, TMB-H cancer, or adjuvant treatment of RCC were generally similar to those occurring in patients with melanoma or NSCLC.
Combination Therapy: Head and Neck Cancer: In patients with HNSCC receiving Pembrolizumab (KEYTRUDA) plus chemotherapy (platinum and 5-FU), adverse reactions occurring at a greater severity (Grade 3-4) and at a higher incidence (≥2% difference) compared to cetuximab plus chemotherapy (platinum and 5-FU) were: fatigue (7% vs. 4.9%), mucosal inflammation (10% vs. 5%), and stomatitis (8% vs. 3.5%).
Gastric Cancer: In patients with gastric cancer receiving Pembrolizumab (KEYTRUDA) plus trastuzumab and chemotherapy (fluoropyrimidine and platinum), adverse reactions occurring in at least 20% of patients and at a higher incidence (≥2% difference) of Grades 3-4 severity compared to placebo plus trastuzumab and chemotherapy (fluoropyrimidine and platinum) were: vomiting (4.6% vs. 1.9%), anemia (14% vs.12%), decreased platelet count (14% vs.10%), and lymphopenia (13% vs. 9%).
Cervical Cancer: In patients with cervical cancer receiving (Pembrolizumab) KEYTRUDA plus chemotherapy (paclitaxel and cisplatin or paclitaxel and carboplatin) with or without bevacizumab, adverse reactions occurring at a higher incidence (≥2%) of Grades 3-5 severity for (Pembrolizumab) KEYTRUDA plus chemotherapy with or without bevacizumab compared to placebo plus chemotherapy with or without bevacizumab were: anemia (30% vs. 27%), neutropenia (12% vs. 10%), thrombocytopenia (8% vs. 5%), asthenia (3.6% vs. 1.6%).
Esophageal Cancer: In patients with esophageal cancer, adverse reactions occurring in at least 20% of patients and at a higher incidence (≥2%) of Grades 3-5 severity for Pembrolizumab (KEYTRUDA) in combination with chemotherapy (cisplatin and 5-FU) compared to placebo and chemotherapy (cisplatin and 5-FU) were: vomiting (7% vs. 5%), stomatitis (6% vs. 3.8%), neutrophil count decreased (24.1% vs 17.3%), and white blood cell count decreased (9.2% vs. 4.9%).
Renal Cell Carcinoma: In Combination with Axitinib (KEYNOTE-426): The most common adverse reactions that occurred in at least 20% of previously untreated patients with RCC receiving Pembrolizumab (KEYTRUDA) and axitinib in KEYNOTE-426 were diarrhea, hypertension, fatigue, hypothyroidism, decreased appetite, palmar-plantar erythrodysaesthesia syndrome, nausea, ALT increased, AST increased, dysphonia, cough and constipation.
In KEYNOTE-426, a higher than expected incidence of Grades 3 and 4 ALT increased (20%) and AST increased (13%) were observed in previously untreated patients with RCC receiving Pembrolizumab (KEYTRUDA) in combination with axitinib. The median time to onset of ALT increased was 2.3 months (range: 7 days to 19.8 months). In patients with ALT ≥3 times ULN (Grades 2-4, n=116), ALT resolved to Grades 0-1 in 94%. Fifty-nine percent of the patients with increased ALT received systemic corticosteroids. Of the patients who recovered, 92 (84%) were rechallenged with either Pembrolizumab (KEYTRUDA) (3%) or axitinib (31%) monotherapy or with both (50%). Of these patients, 55% had no recurrence of ALT >3 times ULN, and of those patients with recurrence of ALT >3 times ULN, all recovered. There were no Grade 5 hepatic events. [See General under Dosage & Administration and Precautions.]
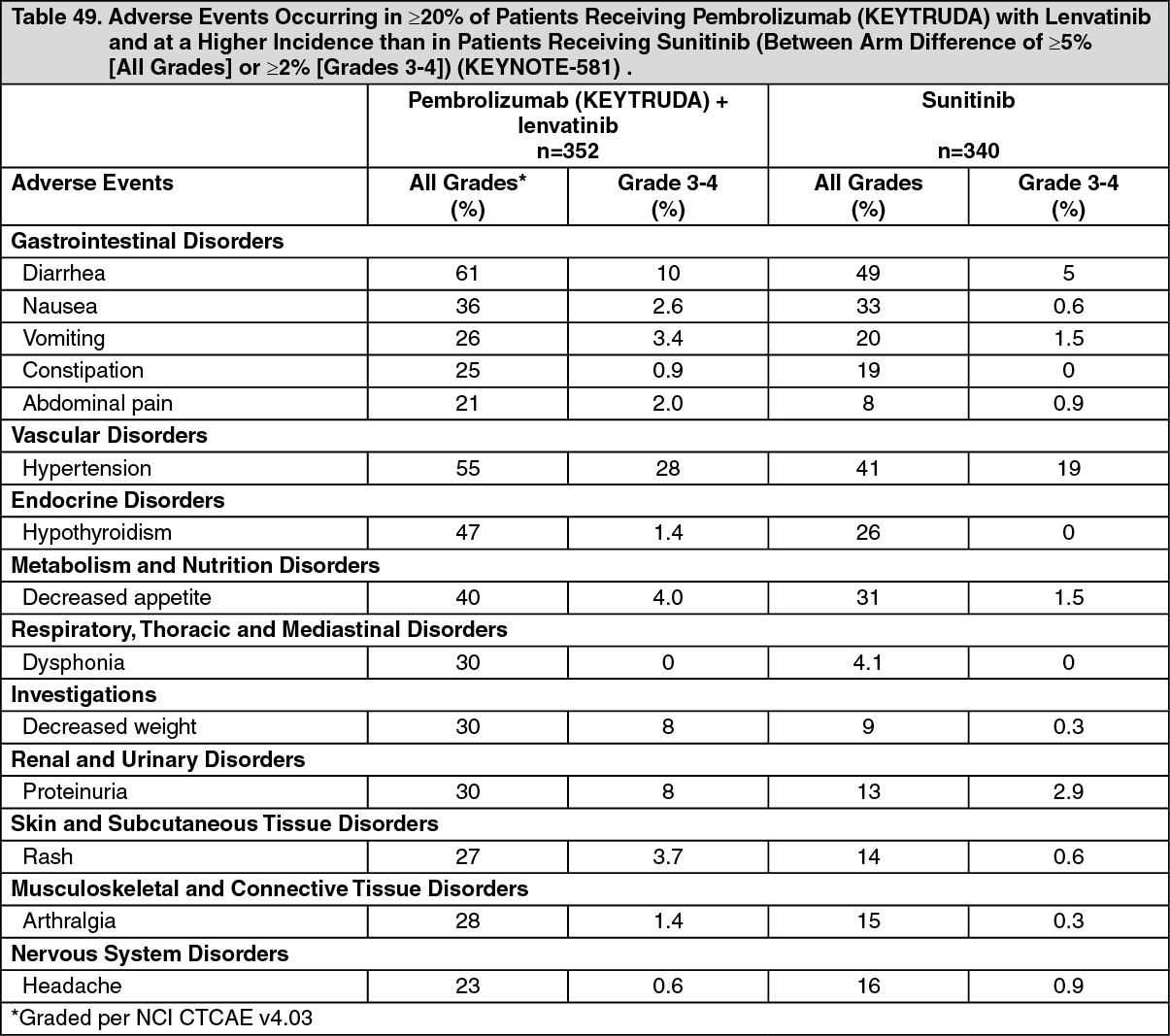
In Combination with Lenvatinib (KEYNOTE-581): Table 49 summarizes the adverse events that occurred in at least 20% of patients treated with Pembrolizumab (KEYTRUDA) and lenvatinib in KEYNOTE-581. (See Table 49.)
 Click on icon to see table/diagram/image
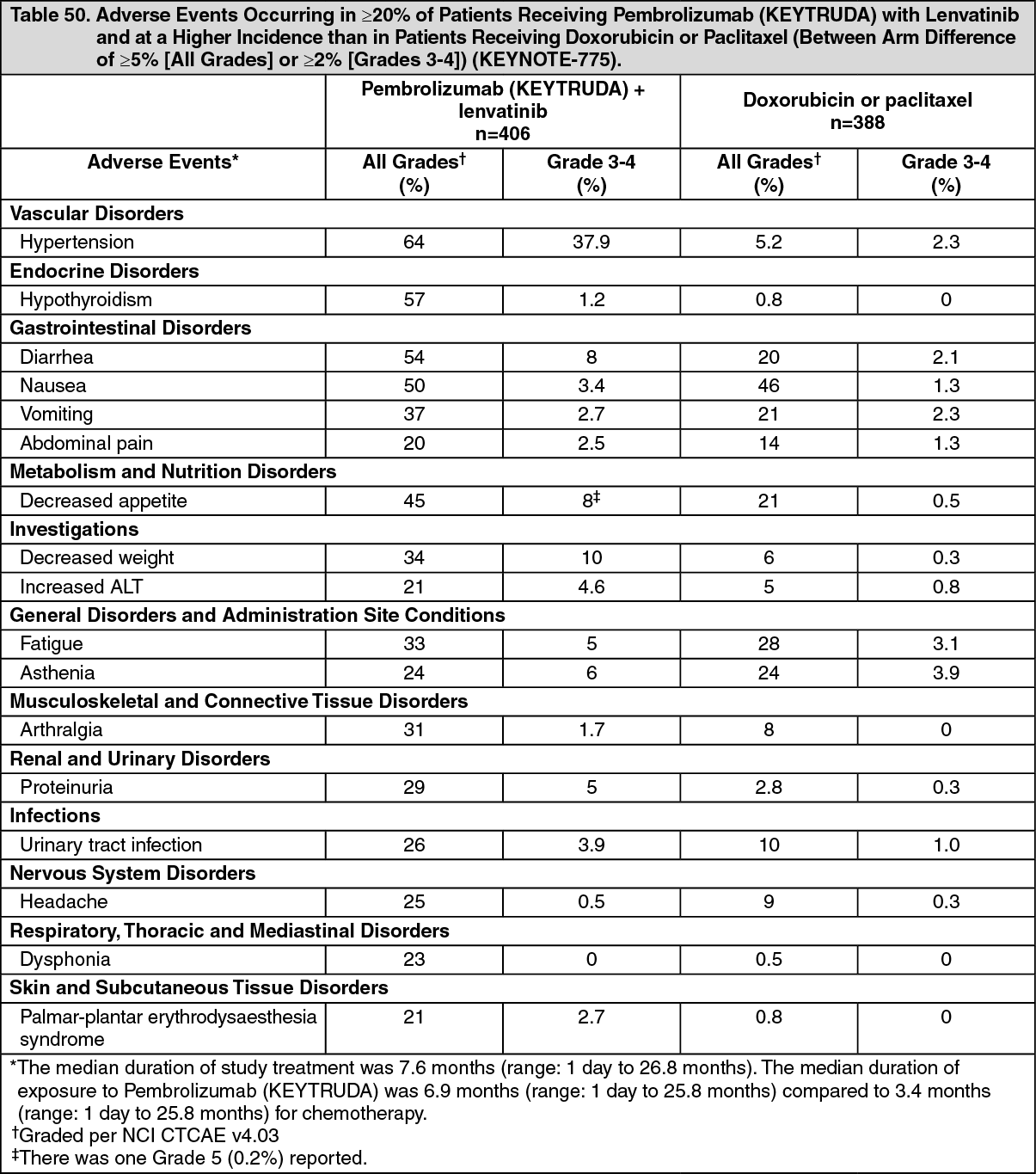
Click on icon to see table/diagram/imageEndometrial Carcinoma: Table 50 summarizes the adverse events that occurred in at least 20% of patients treated with Pembrolizumab (KEYTRUDA) and lenvatinib in KEYNOTE 775. Adverse events occurring in patients with endometrial carcinoma receiving Pembrolizumab (KEYTRUDA) in combination with lenvatinib in KEYNOTE-146 were generally similar to those occurring in patients in KEYNOTE-775. (See Table 50.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageDiscontinuation of Pembrolizumab (KEYTRUDA), lenvatinib or both due to an adverse reaction (Grades 1-4) occurred in 30% of patients; 15% Pembrolizumab (KEYTRUDA), and 11% both drugs. The most common adverse reactions leading to discontinuation of Pembrolizumab (KEYTRUDA) were diarrhea, increased ALT, and intestinal obstruction (each 1.0%). Refer to the lenvatinib prescribing information for lenvatinib discontinuation information.
Dose interruptions of Pembrolizumab (KEYTRUDA), lenvatinib, or both due to an adverse reaction occurred in 69% of patients; Pembrolizumab (KEYTRUDA) was interrupted in 50%, and both drugs were interrupted in 31% of patients. The most common adverse reactions leading to interruption of Pembrolizumab (KEYTRUDA) (≥2%) were diarrhea (8%), increased ALT (3.9%), hypertension (3.4%), increased AST (3.2%), decreased appetite (2.2%), fatigue (2.2%), urinary tract infection (2.2%), proteinuria (2.0%), and asthenia (2.0%). Refer to the lenvatinib prescribing information for lenvatinib interruption information.
Triple Negative Breast Cancer: KEYNOTE 522: Controlled study of neoadjuvant and adjuvant treatment of patients with high-risk early stage TNBC: In patients with high-risk early-stage TNBC receiving Pembrolizumab (KEYTRUDA) in combination with chemotherapy (carboplatin and paclitaxel followed by doxorubicin or epirubicin and cyclophosphamide), given as a neoadjuvant treatment and continued as monotherapy adjuvant treatment, adverse reactions occurring in at least 20% of the patients and at a higher incidence (≥5% difference) compared to patients with TNBC receiving placebo in combination with chemotherapy (carboplatin and paclitaxel followed by doxorubicin or epirubicin and cyclophosphamide), given as a neoadjuvant treatment and continued alone as adjuvant treatment were diarrhea (41% vs. 34%), rash (30% vs. 24%), pyrexia (28% vs. 19%), and decreased appetite (23% vs. 17%). Of these adverse reactions, Grade 3-4 events were diarrhea (3.2% vs. 1.8%), rash (1.8% vs. 0.3%), pyrexia (1.3% vs. 0.3%), and decreased appetite (0.9% vs. 0.3%).
KEYNOTE 355: Controlled study of combination therapy in patients with locally recurrent unresectable or metastatic TNBC: In patients with TNBC receiving Pembrolizumab (KEYTRUDA) in combination with chemotherapy (paclitaxel, nab paclitaxel, or gemcitabine and carboplatin), adverse reactions occurring in at least 20% of the patients and at a higher incidence (≥5% difference) compared to patients with TNBC receiving placebo in combination with chemotherapy (paclitaxel, nab paclitaxel, or gemcitabine and carboplatin) were diarrhea (28% vs. 23%), decreased appetite (21% vs. 14%), and rash (20% vs. 12%). Of these adverse reactions, Grade 3-4 events were diarrhea (1.8% vs. 1.8%), decreased appetite (0.8% vs. 0.4%), and rash (0.8% vs. 0.0%).
Postmarketing Experience: The following adverse reactions have been identified during post-approval use of Pembrolizumab (KEYTRUDA). Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
Musculoskeletal and connective tissue disorders: arthritis.
Eye disorders: Vogt-Koyanagi-Harada syndrome.
Immune system disorders: hemophagocytic lymphohistiocytosis
View ADR Monitoring Form