


 Sign Out
Sign Out


PD-L1 expression should be evaluated using the PD-L1 IHC 22C3 pharmDx kit or equivalent. For gastric cancer, if PD-L1 expression is not detected in an archival specimen, obtain a tumor biopsy for PD-L1 testing, if feasible.
MSI or MMR tumor status should be evaluated using a validated test.
TMB-H tumor status should be evaluated using the FoundationOne CDx assay or equivalent.
Because the effect of prior chemotherapy on test results for tumor mutation burden (TMB-H), MSI-H, or dMMR in patients with high grade gliomas is unclear, it is recommended to test for these markers in the primary tumor specimens obtained prior to initiation of temozolomide chemotherapy in patients with high grade gliomas.
Recommended Dosing: Pembrolizumab (KEYTRUDA) is administered as an intravenous infusion over 30 minutes.
The recommended dose of Pembrolizumab (KEYTRUDA) in adults is either: 200 mg every 3 weeks or; 400 mg every 6 weeks.
For use in combination, see the prescribing information for the concomitant therapies. When administering Pembrolizumab (KEYTRUDA) as part of a combination with intravenous chemotherapy, Pembrolizumab (KEYTRUDA) should be administered first.
For RCC patients treated with Pembrolizumab (KEYTRUDA) in combination with axitinib, see the prescribing information regarding dosing of axitinib. When used in combination with Pembrolizumab (KEYTRUDA), dose escalation of axitinib above the initial 5 mg dose may be considered at intervals of six weeks or longer [see Pharmacology: Pharmacodynamics: Clinical Studies under Actions].
For endometrial carcinoma and RCC patients treated with Pembrolizumab (KEYTRUDA) in combination with lenvatinib, the recommended initial dose of lenvatinib is 20 mg orally once daily until disease progression or unacceptable toxicity.
Patients should be treated with Pembrolizumab (KEYTRUDA) until disease progression or unacceptable toxicity. Atypical responses (i.e., an initial transient increase in tumor size or small new lesions within the first few months followed by tumor shrinkage) have been observed. Clinically stable patients with initial evidence of disease progression should remain on treatment until disease progression is confirmed.
For the adjuvant treatment of melanoma or RCC, Pembrolizumab (KEYTRUDA) should be administered for up to one year or until disease recurrence or unacceptable toxicity.
For the neoadjuvant and adjuvant treatment of high-risk early-stage TNBC, patients should be treated with neoadjuvant Pembrolizumab (KEYTRUDA) in combination with chemotherapy for 8 doses of 200 mg every 3 weeks or 4 doses of 400 mg every 6 weeks or until disease progression that precludes definitive surgery or unacceptable toxicity, followed by adjuvant treatment with Pembrolizumab (KEYTRUDA) as monotherapy for 9 doses of 200 mg every 3 weeks or 5 doses of 400 mg every 6 weeks or until disease recurrence or unacceptable toxicity. Patients who experience disease progression that precludes definitive surgery or unacceptable toxicity related to Pembrolizumab (KEYTRUDA) as neoadjuvant treatment in combination with chemotherapy should not receive Pembrolizumab (KEYTRUDA) monotherapy as adjuvant treatment.
Dose Modifications: No dose reductions of Pembrolizumab (KEYTRUDA) are recommended. Withhold or discontinue Pembrolizumab (KEYTRUDA) to manage adverse reactions as described in Table 43. (See Table 43.)
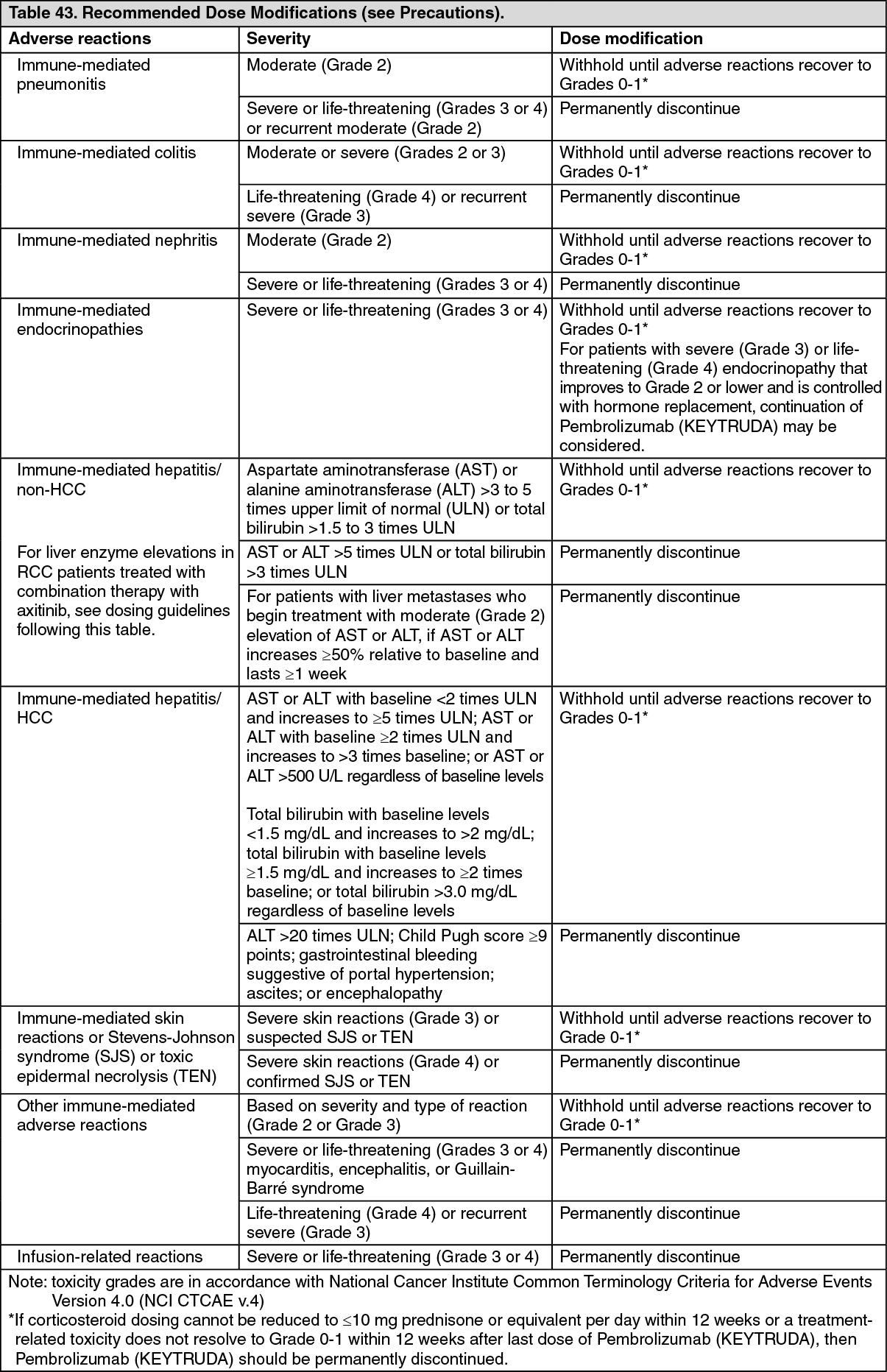 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageIn patients with cHL with Grade 4 hematological toxicity, Pembrolizumab (KEYTRUDA) should be withheld until adverse reactions recover to Grades 0-1.
In patients with RCC being treated with Pembrolizumab (KEYTRUDA) in combination with axitinib: If ALT or AST ≥3 times ULN but <10 times ULN, without concurrent total bilirubin ≥2 times ULN, withhold both Pembrolizumab (KEYTRUDA) and axitinib until these adverse reactions recover to Grades 0-1. Consider corticosteroid therapy. Consider rechallenge with a single drug or sequential rechallenge with both drugs after recovery. If rechallenging with axitinib, consider dose reduction as per the axitinib prescribing information.
If ALT or AST ≥10 times ULN or >3 times ULN with concurrent total bilirubin ≥2 times ULN, permanently discontinue both Pembrolizumab (KEYTRUDA) and axitinib and consider corticosteroid therapy.
When administering Pembrolizumab (KEYTRUDA) in combination with lenvatinib, interrupt one or both or dose reduce or discontinue lenvatinib to manage adverse reactions as appropriate. For recommendations for management of adverse reactions of lenvatinib, refer to the prescribing information for lenvatinib. No dose reductions are recommended for Pembrolizumab (KEYTRUDA).
Pediatric Patients: For melanoma, cHL and TMB-H cancer, the recommended dose of Pembrolizumab (KEYTRUDA) in pediatric patients is 2 mg/kg (up to a maximum of 200 mg), administered as an intravenous infusion over 30 minutes every 3 weeks.
Geriatric Patients: No overall differences in safety or efficacy were reported between elderly patients (65 years and over) and younger patients (less than 65 years). No dose adjustment is necessary in this population.
Renal Impairment: No dose adjustment is needed for patients with mild or moderate renal impairment. Pembrolizumab (KEYTRUDA) has not been studied in patients with severe renal impairment.
Hepatic Impairment: No dose adjustment is needed for patients with mild hepatic impairment. Pembrolizumab (KEYTRUDA) has not been studied in patients with moderate or severe hepatic impairment.