750 mg: Each vial contains: Cefuroxime (as sodium) 750 mg.
1.5 g: Each vial contains: Cefuroxime (as sodium) 1.5 g.
Cefuroxime sodium is the essential ingredient of this drug without excipients. It is the sodium salt of (6R,7R)-3-carbamoyloxymethyl-7-[Z-2-methoxyimino-2-(fur-2-yl)acetamido]ceph-3-em-4-carboxylate.
Molecular formula: C16H15N4NaO8S. Molecular weight: 446.37.
It is a white to yellowish powder or crystalline powder.
Pharmacology: Pharmacological Action: 1.5 g: Cefuroxime is a second generation cephalosporin. The bactericidal action of cefuroxime results from inhibition of cell-wall synthesis through binding with bacterial protein. Cefuroxime has antibacterial activity against a wide range of pathogenic bacteria, and it is stable in the presence of many kinds of beta-lactamases, especially stable with plasmid mediated-enzyme commonly found in Enterobacteriaceae.
From animal in vitro test and the treatment of clinical infections, it is proven that cefuroxime is usually active against the following bacteria: Aerobes, Gram-positive: Staphylococcus aureus (including beta-lactamase producing bacteria), Streptococcus pneumoniae, and Streptococcus pyogenes.
Aerobes, Gram-negative: Escherichia coli, Haemophilus influenzae (including beta-lactamase producing bacteria), Haemophilus parainfluenzae, Klebsiella pneumoniae, Moraxella (Branhamella) catarrhalis (including beta-lactamase producing bacteria), Neisseria gonorrhoeae (including beta-lactamase producing bacteria).
Most strains of Enterococcus faecalis, methicillin-resistant Staphylococcus aureus, Clostridium difficile, and Bacteroides fragilis have been shown by in vitro tests to be resistant to cefuroxime.
Pharmacokinetics: 750 mg: Cefuroxime sodium (CEFUVEX) is given by intramuscular or intravenous injection. Peak plasma concentrations of about 27 μg per mL have been achieved 45 minutes after an intramuscular dose of 750 mg with measurable amounts presents 8 hours after a dose. Up to 50% of cefuroxime in the circulation is bound to plasma proteins. The plasma half life is about 70 minutes and is prolonged in patients with renal impairment and in neonates.
Cefuroxime is widely distributed in the body including pleural fluid, sputum, bone, synovial fluid and aqueous humor, but only achieves therapeutic concentrations in the CSF when the meninges are inflamed. It crosses the placenta and has been detected in breast milk.
Cefuroxime is excreted unchanged by glomerular filtration and renal tubular secretion, and high concentrations are achieved in the urine. Following injection, most of a dose of cefuroxime is secreted within 24 hours, the majority within 6 hours. Probenecid competes for renal tubular secretions with cefuroxime resulting in higher and more prolonged plasma concentrations of cefuroxime. Small amounts of cefuroxime are excreted in bile.
Plasma concentrations are reduced by dialysis.
1.5 g: After I.M. injection of a 750-mg dose of cefuroxime to normal volunteers, the mean peak serum concentration was 27 μg/mL. The peak occurred at approximately 45 minutes (range, 15 to 60 minutes). Following I.V. doses of 750 mg and 1.5 g, serum concentrations were approximately 50 and 100 μg/mL, respectively, at 15 minutes. Therapeutic serum concentrations of approximately 2 μg/mL or more were maintained for 5.3 hours and 8 hours or more, respectively. There was no evidence of accumulation of cefuroxime in the serum following I.V. administration of 1.5-g doses every 8 hours to normal volunteers. The serum half-life after either I.M. or I.V. injections is approximately 80 minutes.
Approximately 89% of a dose of cefuroxime is excreted by the kidneys over an 8-hour period, resulting in high urinary concentrations.
Following the I.M. injection of a 750-mg single dose, urinary concentrations averaged 1300 μg/mL during the first 8 hours. I.V. injection doses of 750 mg and 1.5 g produced urinary levels averaging 1150 and 2500 μg/mL, respectively, during the first 8-hour period.
The concomitant oral administration of probenecid with cefuroxime slows tubular secretion, decreases renal clearance by approximately 40%, increases the peak serum level by approximately 30%, and increases the serum half-life by approximately 30%. Cefuroxime is detectable in therapeutic concentrations in pleural fluid, joint fluid, bile, sputum, bone, and aqueous humor.
Cefuroxime is detectable in therapeutic concentrations in cerebrospinal fluid (CSF) of adults and pediatric patients with meningitis. Cefuroxime concentration can be detected in cerebrospinal fluid during multiple dosing of patients with meningitis.
Cefuroxime is approximately 50% bound to serum protein.
Toxicology: Genotoxicity: 1.5 g: Although potential carcinogenicity of this drug is not evaluated by animal lifelong study, mutagenic action of this drug is not found in micronucleus test and bacterial test.
Reproductive toxicity: 1.5 g: Cefuroxime does not damage the reproductive capacity of rats with a dose of 1000 mg/Kg/day, and there is no damage to the growth of fetus of rats and mice with a dose of 3200 mg/Kg/day. But the pertinence between animal and human is still not established by clinical study.
750 mg: Used in the treatment of susceptible infections like bone and joint infections, bronchitis, gonorrhea, meningitis, otitis media, peritonitis, pharyngitis, sinusitis, skin infections surgical infections, and urinary tract infections.
1.5 g: This drug is indicated for the treatment of patients with infections caused by susceptible strains of the designated organisms in the following diseases: Respiratory tract infections and ear, nose and throat (ENT) infections caused by Streptococcus pneumoniae, Haemophilus influenzae (including ampicillin-resistant strains), Klebsiella spp., Staphylococcus aureus (penicillinase-producing and non-producing strains), Streptococcus pyogenes, and Escherichia coli, including otitis media, sinusitis, tonsillitis, pharyngitis, acute and chronic bronchitis, bronchiectasis with infection, bacterial pneumonia, lung abscess and postoperative pulmonary infection.
Urinary tract infections caused by Escherichia coli and Klebsiella spp., including pyelonephritis, cystitis and asymptomatic bacteriuria.
Skin and skin structure infections caused by Staphylococcus aureus (penicillinase producing and non-producing strains), Streptococcus pyogenes, Escherichia coli, Klebsiella spp and Enterobacter spp., including cellulitis, erysipelas, peritonitis and traumatic infection.
Septicemia caused by Staphylococcus aureus (penicillinase-producing and non-producing strains), Streptococcus pneumoniae, Escherichia coli, Haemophilus influenzae (including ampicillin-resistant strains), and Klebsiella spp.
Meningitis caused by Streptococcus pneumoniae, Haemophilus influenzae (including ampicillin-resistant strains), Neisseria meningitidis, and Staphylococcus aureus (penicillinase producing and non-producing strains).
Gonorrhea: Uncomplicated and complicated gonorrhea due to Neisseria gonorrhoeae (penicillinase producing and non-producing strains), especially for the patients in whom penicillin treatment is not recommended.
Bone and joint infections caused by Staphylococcus aureus (penicillinase producing and non-producing strains).
The preoperative prophylactic administration of this drug may prevent the growth of susceptible disease-causing bacteria and thereby may reduce the incidence of certain perioperative and postoperative infections in patients undergoing surgical procedures (e.g. abdominal and pelvic surgery, orthopedic surgery, cardiac, lung, esophagus or vascular surgeries, and total joint arthroplasty) that are classified as clean-contaminated or potentially contaminated procedures.
750 mg: Infants: 30-60 mg per kg body weight per day maximum dose of 100 mg/day given in 3 or 4 divided doses.
Adults: 750 mg twice daily.
For infections the usual dose is 750 mg every 8 hours. In case of severe infections 1.5 g of cefuroxime is given intravenously for about 6 or 8 hours.
Or as directed by the Physicians.
The reconstituted solution should be used immediate after preparation. Do not allow to freeze.
1.5 mg: After constitution, this drug may be given intravenously or by deep intramuscular injection into a large muscle mass. Before injecting intramuscularly, aspiration is necessary to avoid inadvertent injection into a blood vessel.
For Intramuscular Use: Cefuroxime should be constituted with 6 mL of sterile water for injection. Shake gently to disperse and withdraw completely the resulting suspension for injection.
For Intravenous Use: Cefuroxime should be constituted with not less than 12 mL of sterile water for injection. Shake gently and then slowly inject the solution into a vein or give it through the tubing system.
The usual adult dosage range for this drug is 750 mg to 1.5 grams every 8 hours, usually for 5 to 10 days.
In life-threatening infections or infections due to less susceptible organisms, 1.5 grams every 6 hours may be required. In bacterial meningitis, the dosage should not exceed 3 grams every 8 hours. The recommended dosage for uncomplicated gonococcal infection is 1.5 grams given intramuscularly as a single dose at 2 different sites together with 1 gram of oral probenecid.
For preventive use for clean-contaminated or potentially contaminated surgical procedures, 1.5-gram dose administered intravenously just before surgery (approximately one-half to 1.5 hours before the initial incision) is recommended. Thereafter, give 750 mg intravenously or intramuscularly every 8 hours when the procedure is prolonged. For preventive use during open chest surgery, a 1.5-gram dose administered intravenously at the induction of anesthesia and every 12 hours thereafter for a total of 6 grams is recommended.
For pediatric patients above 3 months of age, administration of 50 to 100 mg/kg/day in equally divided doses every 6 to 8 hours has been successful for most infections susceptible to cefuroxime. The higher dosage of 100 mg/kg/day (not to exceed the maximum adult dosage) should be used for the more severe or serious infections. In bone and joint infections, 150 mg/kg/day (not to exceed the maximum adult dosage) is recommended in equally divided doses every 8 hours. In cases of bacterial meningitis, a larger dosage is recommended, 200 to 240 mg/kg/day in equally divided doses every 6 to 8 hours. The total daily dose for pediatric patients should not exceed 6 grams.
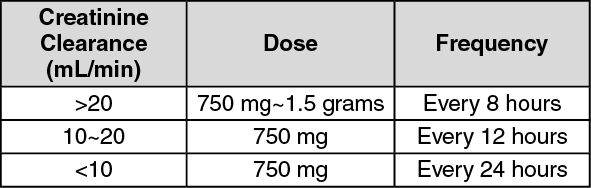
Impaired Renal Function:
A reduced dosage must be employed when renal function is impaired. Dosage should be determined by the degree of renal impairment. (See table.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
In pediatric patients with renal insufficiency, the frequency of dosing should be modified consistent with the recommendations for adults.
1.5 g: Overdosage of the drug can cause cerebral irritation leading to convulsions. Serum levels of cefuroxime can be reduced by hemodialysis and peritoneal dialysis.
750 mg: Cefuroxime is contraindicated in patients with renal impairment, during 1st trimester of pregnancy, elderly and in rare cases it causes hypersensitivity.
1.5 g: This product is contraindicated in patients with known allergy to the cephalosporin group of antibiotics.
750 mg: Should not be administered in renal impairment, dosage reduction is necessary. It should not be administered to patients who are hypersensitive with to it or with other cephalosporins. It may interfere with the Jaffe method of measuring creative concentrations and produces false results. It gives positive results for Coombs' test and reactions for glucose using copper reduction reactions.
1.5 g: This drug has cross allergy with penicillin. It should be given with caution to penicillin-allergic patients and is not recommended in patients who have had an anaphylactic shock to penicillin.
Evaluation of renal status during therapy is recommended, especially in seriously ill patients receiving the maximum doses.
The total daily dose of the drug should be reduced in patients with renal insufficiency. It should be given with caution to patients receiving concurrent treatment with potent diuretics or aminoglycoside antibiotics, as these regimens have been reported to induce renal impairment. So for this kind of patients, evaluation of renal status during therapy is recommended.
It should be notified that this drug can induce pseudomembranous colitis. After the diagnosis of pseudomembranous colitis has been established, appropriate therapeutic measures should be initiated. Mild cases of pseudomembranous colitis usually respond to drug discontinuation alone. In moderate to severe cases, consideration should be given to management with fluids and electrolytes, protein supplementation and treatment with an antibacterial drug clinically effective against Clostridium difficile colitis.
Mild-to-moderate hearing loss has been reported in a few pediatric patients treated with this drug.
Laboratory test interactions: Positive Coombs' test may occur which may interfere with blood cross matching. A false-positive reaction for glucose in the urine may occur with copper reduction tests (Benedict's or Fehling's solution or with CLINITEST tablets) but not with enzyme-based tests for glycosuria. A
false-negative result may occur in the ferricyanide test to determine blood plasma glucose levels in patients receiving this drug.
Use in pregnancy & lactation: This drug should be used during pregnancy only if the therapeutic benefit outweighs the risk to the patient. Since cefuroxime is excreted in human milk, caution should be exercised when this drug is administered to a nursing woman.
Use in children: Accumulation of other members of the cephalosporin class in newborn infants (with resulting prolongation of drug half-life) has been reported. Safety and effectiveness in pediatric patients below 3 months of age have not been established, so it is not recommended to be used in these patients.
Use in the elderly: Dosage in elderly patients of 65 years and over should be reduced to 2/3~1/2 of the usual adult dose. The total daily dose should not exceed 3 grams.
750 mg: Gastrointestinal disturbances e.g. diarrhea, nausea and vomiting. There have been rare reports of erythema multiforme, including Stevens-Johnson syndrome and toxic epidermal necrolysis.
1.5 g: Cefuroxime is generally well tolerated. The most common adverse reactions are as follows:
Location reactions: Thrombophlebitis.
Gastrointestinal: Diarrhea, nausea, pseudomembranous colitis, etc.
Hypersensitivity reactions: Rash, pruritus and urticaria commonly occur. Rare cases of anaphylaxis, drug fever, erythema multiforme, interstitial nephritis, toxic epidermal necrolysis, and Stevens-Johnson syndrome have occurred.
Blood: A decrease in hemoglobin and hematocrit, transient eosinophilia, transient neutropenia and leukopenia have been observed. There have been rare reports of thrombocytopenia.
Hepatic: Transient rise in ALT and AST, alkaline phosphatase, lactate dehydrogenase (LDH), and bilirubin levels has been noted.
Others: Vomiting, abdominal pain, colitis, vaginitis including vaginal candidiasis, hepatic dysfunction including cholestasis, aplastic anemia, hemolytic anemia, hemorrhage, triggering seizures, prolonged prothrombin time, pancytopenia, and agranulocytosis.
750 mg: Probenecid reduces the renal clearance of cefuroxime.
1.5 g: Nephrotoxicity has been reported following concomitant administration of aminoglycoside antibiotics and cephalosporins.
A false-positive reaction for glucose in the urine may occur with copper reduction tests (Benedict's or Fehling's solution or with CLINITEST tablets) but not with enzyme-based tests for glycosuria. As a false-negative result may occur in the ferricyanide test, it is recommended that either the glucose oxidase or hexokinase method be used to determine blood plasma glucose levels in patients receiving this drug. Cefuroxime does not interfere with the assay of serum and urine creatinine by the alkaline picrate method.
Cefuroxime is incompatible with the following drugs: amikacin sulfate, gentamicin, kanamycin, tobramycin, neomycin, aureomycin hydrochloride, tetracycline hydrochloride, colistin sodium methanesulfonate, polymyxin B sulfate, erythromycin gluconate, erythromycin lactobionate, lincomycin, soluble barbiturates, calcium chloride, calcium glucoheptonate, diphenhydramine hydrochloride as well as other antihistamines, lidocaine, norepinephrine, metaraminol, ritalin, succinylcholine, etc. And it may also be incompatible with the following drugs occasionally: penicillin, methicillin, hydrocortisone sodium succinate, phenytoin sodium, prochlorperazine, vitamin B group, vitamin C and protein hydrolysate.
Concurrent treatment of this drug with potent diuretics (e.g. furosemide, ethacrynic acid and bumetanide), antineoplastics (e.g. carmustine and streptozotocin), or aminoglycoside antibiotics may increase the risk of nephrotoxicity.
Clavulanic acid may increase the antibacterial activity of cefuroxime against some cefuroxime-resistant beta-lactamase producing Gram-negative bacilli.
750 mg: Store at temperatures not exceeding 25°C.
1.5 g: Store at temperatures not exceeding 30°C. Protect from light.
Shelf-Life: 1.5 g: 24 months.
J01DC02 - cefuroxime ; Belongs to the class of second-generation cephalosporins. Used in the systemic treatment of infections.
Cefuvex powd for inj 1.5 g
10 × 1's (P495/vial)
Cefuvex powd for inj 750 mg
10 × 1's (P285/vial)


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image


 Sign Out
Sign Out
