Combination Use with Cisplatin: Malignant Pleural Mesothelioma: Recommended Dose: 500 mg/m
2 administered as IV infusion over 10 min on day 1 of each 21-day cycle. Recommended Dose of Cisplatin: 75 mg/m
2 infused over 2 hrs beginning approximately 30 min after the end of pemetrexed administration. Patients should receive hydration consistent with local practice prior to and/or after receiving cisplatin.
Single-Agent Use: Nonsquamous Non-Small Cell Lung Cancer: Recommended Dose: 500 mg/m
2 administered as an IV infusion over 10 min on day 1 of each 21-day cycle.
Premedication Regimen: Corticosteroid skin rash has been reported more frequently in patients not pre-treated with a corticosteroid. Pre-treatment with dexamethasone (or equivalent) reduces the incidence and severity of ocutaneous reaction. In clinical trials, dexamethasone 4 mg was given by mouth twice daily the day before and the day after pemetrexed administration.
Vitamin Supplementation: To reduce toxicity, patients treated with pemetrexed must be instructed to take a low-dose oral folic acid preparation or multivitamin with folic acid on a daily basis. At least 5 daily doses of folic acid must be taken during the 7-day period preceding the 1st dose of pemetrexed and dosing should continue during the full course of therapy and for 21 days after the last dose of pemetrexed. Patients must also receive 1 IM injection of vitamin B12
during the week preceding the 1st dose of pemetrexed. In clinical trials, the dose of folic acid studied ranged from 350-100 mcg and the dose of vitamin B12 was 1000 mcg. The most commonly used dose of oral folic acid clinical trials was 400 mcg (see Warnings).
Monitoring: Complete blood cell counts, including platelet counts, should be performed on all patients receiving pemetrexed. Patients should be monitored for nadir and recovery, which were tested in the clinical study before each dose on days 8 and 15 of each cycle. Patients should not begin a new cycle of treatment unless the ANC is ≥1500 cells/mm
1, the platelet count is ≥100,000 cells/mm
3 and creatinine clearance is ≥45 mL/min. Periodic chemistry tests should be performed to evaluate renal and hepatic function.
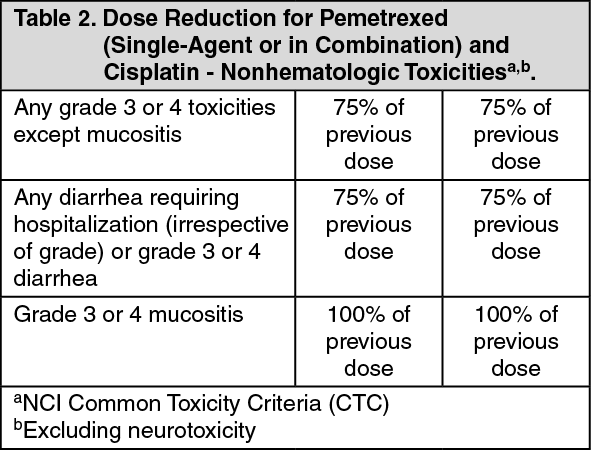
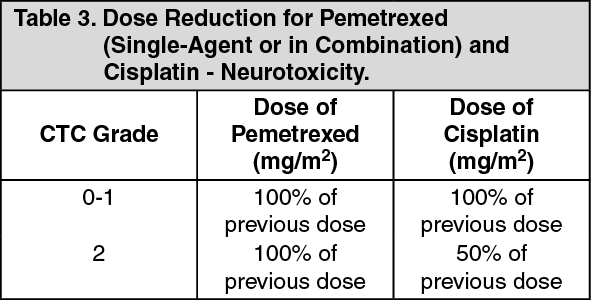
Dose Reduction Recommendations: Dose adjustments at the start of a subsequent cycle should be based on nadir hematologic counts or maximum nonhematologic toxicity form the preceding cycle of therapy. Treatment may be delayed to allow sufficient time for recovery. Upon recovery, patients should be retreated using the guidelines as shown in Tables 1, 2 and 3.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Administration:
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Administration: Reconstitute each 100 mg vial with 4.2 mL of sodium chloride 0.9% injection (preservative free).
Reconstitute each 500-mg vial with 20 mL of sodium chloride 0.9% injection (preservative free).
An appropriate quantity of reconstituted pemetrexed solution must be further diluted into a solution of sodium chloride 0.9% injection so that the total volume of solution is 100 mL. Pemetrexed is administered as an IV infusion over 10 min.



 Sign Out
Sign Out