


 Sign Out
Sign Out

Disodium Edetate is a non-antibiotic adjuvant entity and membrane permeability enhancer, chelator with a high affinity for calcium, zinc & other divalent ions. It does not have antimicrobial property of its own but acts as a potentiator and makes ceftriaxone sulbactam combo effective in Metallo-beta-lactamase (MBL) and other ESBL strains (TEM, SHV, AMP-C, CTX-M). It alters the porosity of bacterial cell membrane and enhances the penetration of ceftriaxone and sulbactam. It also inhibits Efflux pump by altering genes expression responsible for OMPs expression. Due to its chelation property it chelates divalent ions of lipopolysaccharide layer and makes biofilm porous and thus breaks existing biofilm and prevents biofilm formation.
Sulbactam sodium is a β-lactamase inhibitor with weak antibacterial action. Sulbactam is an irreversible inhibitor of β-lactamase; it binds the enzyme and does not allow it to interact with the antibiotic, thus extending their spectrum activity. It has maximum activity against CTX-M type of class A β-lactamases, which is the most common β-lactamases of this class. It has also got moderate activity against other class A β-lactamases including TEM & SHV. It does not induce the production of AmpC type class C beta lactamases.
ELORES, a novel antibiotic adjuvant entity comprising Ceftriaxone, Sulbactam & Disodium edetate powder for solution for injection/Infusion is a synergistic antimicrobial antibiotic adjuvant entity with marked in-vitro antibacterial activity against a broad spectrum of ESBL producing microorganisms. Presence of Disodium Edetate synergizes the activity of ceftriaxone and sulbactam as it helps in opening porin channels and allows more drug to enter periplasmic space resulting in enhanced killing. ELORES alters the membrane potential, resulting in disturbing ATP balance required for efflux pump activity and hence is effective in bacterial strains where efflux is overactive such as in P. aeruginosa and E.coli.
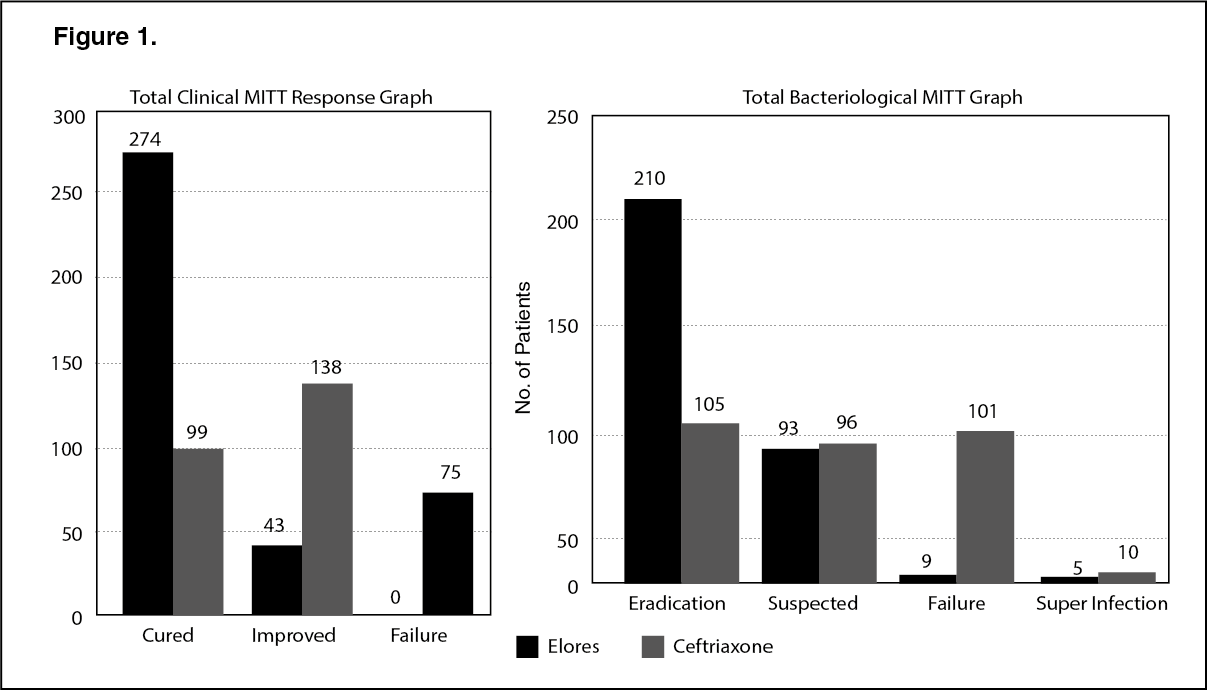
Clinical Studies: An open label, randomized, comparative, Phase III study conducted to compare the efficacy and safety of ELORES with ceftriaxone in patients with various bacterial infections like Lower respiratory tract infection, Urinary tract infection, Skin and Skin Structure Infection, Otitis Media, Bone and Joint infection, Bacterial septicemia and Surgical prophylaxis in 654 patients.
Study drugs: ELORES 3 g (ceftriaxone 2000 mg with sulbactam 1000 mg and disodium edetate 74 mg) or monotherapy with Ceftriaxone, given IV, once daily, (n = 654).
The clinical cure, treatment failures and bacteriological response of ELORES and Ceftriaxone were as follows, (see Figures 1 and 2.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image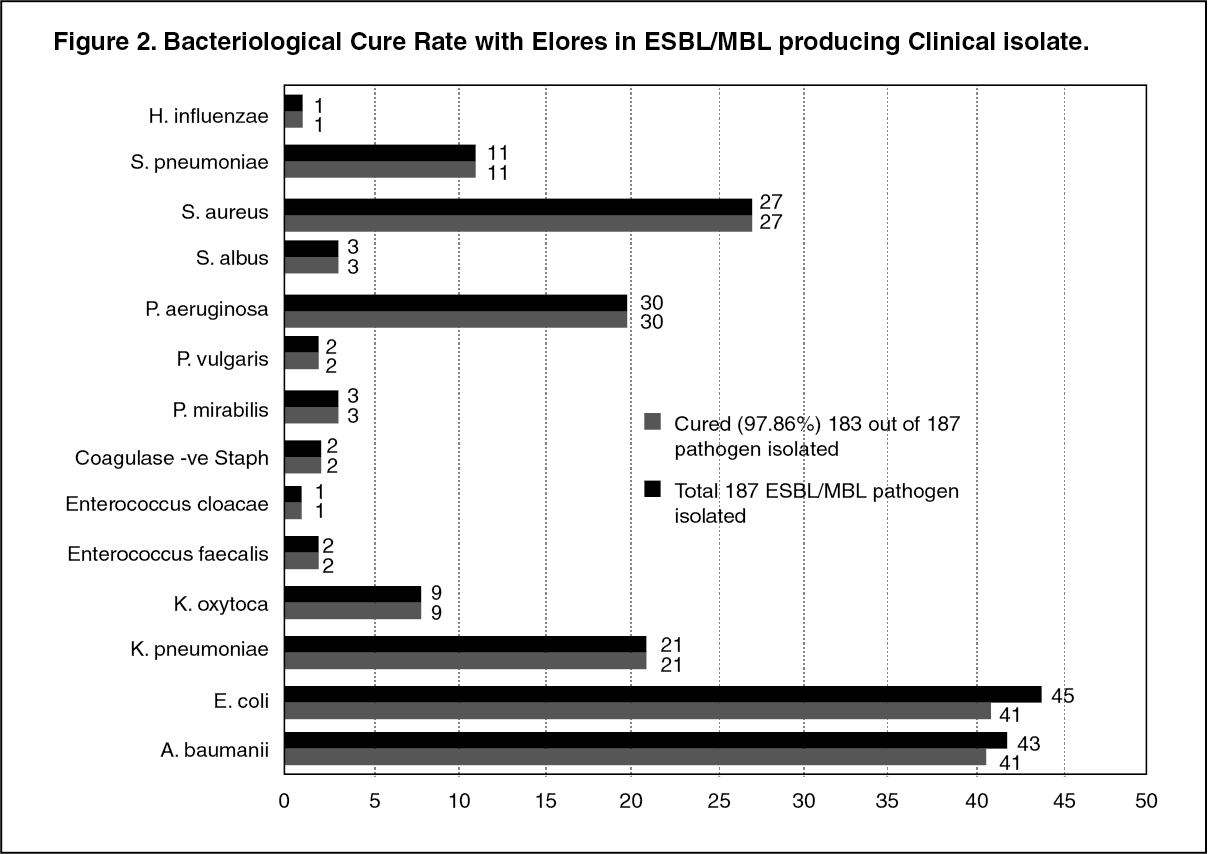 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageELORES 3 g is safe and effective option in the treatment of various ESBL/MBL resistant bacteriological infections.
PK-PD Correlation: The pharmacodynamic effect of ceftriaxone depends on the time above which plasma concentration remains above MIC. Whereas, as per the reported data on Time kill curve (TKC) and beta lactamase inhibition potential of beta lactamase inhibitors (BLI), the plasma concentration of BLI above MIC is required only up to 90 minutes, and the inhibition is maintained up to the time, the plasma concentration of beta lactam antibiotic is maintained above MIC to a maximum of 8 to 12 hrs. Based on 30 min infusion pharmacokinetic data of ELORES in human volunteers, 60 min and 90 min infusion PK data are simulated based on In-house software. It is evident from simulations that compared to 30 min and 60 min infusion, 90 minutes infusion will maintain the required Sulbactam concentration for more time. Hence, 90 min infusion regimen could be preferred for ELORES in case of treating infections where the clinical isolate exhibit intermediate sensitivity.
Pharmacokinetics: Absorption: ELORES is to be administered intravenously.
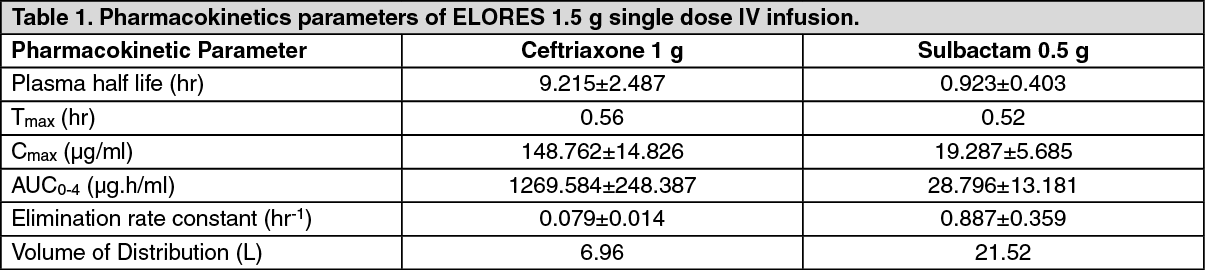
Following intravenous administration, peak serum concentrations of Ceftriaxone and Sulbactam are seen after 30 minutes. The maximum plasma conc of Ceftriaxone after a single IV dose of 1.5 g is about 148.762 µg/ml (SD ± 14.826) and is reached 0.563 hours (SD ± 0.1 69) after the dose, while that of Sulbactam sodium is 19.287 (SD ± 5.685 µg/ml) and is reached approximately 0.521 hour (SD ± 0.102) in healthy volunteers after the dose.
Distribution: Ceftriaxone distributes well in various compartments include extravascular spaces, tissue fluid, synovial fluid of inflamed joints and also passes the placental barrier. The volume of distribution of Ceftriaxone sodium is 7-12 L and Sulbactam is 18-27.6 L. Ceftriaxone is reversibly bound to albumin. The binding is 95% at plasma concentrations less than 100 mg/l with the binding percentage decreasing as the concentration increases (to 85 % at ceftriaxone plasma concentrations of 300 µg/ml). The ceftriaxone is distributed in 5.2 hours approximately in blood stream, while sulbactam reaches its half life in 0.94 hours. Sulbactam has been found to be approximately 38% reversibly bound to human serum protein.
Metabolism: Ceftriaxone does not undergo systemic metabolism but it is broken down in the small intestine by bacterial action.
Disodium Edetate molecule is not metabolized in the body, it thus passes very rapidly into the urine carrying its metallic ion with it. Disodium Edetate molecule leave the body intact.
Sulbactam is not metabolised, but is excreted primarily in the urine (glomerular filtration and tubular secretion) with a small amount being recovered in bile and faeces.
Elimination: Over 1.5 to 3 g dose range, the values of elimination half-life range from 6 to 9 hours, total plasma clearance from 0.6-1.4 l/h and renal clearance from 0.3-0.7 l/h.
Approximately 50-60 % of ceftriaxone and 70-80% of Sulbactam is eliminated as an unchanged active substance in the urine whilst the remainder is excreted via the bile into the faeces as microbiologically inactive metabolites.
ELORES concentrates in the urine arc 5-10 times higher than those found in the plasma.
ELORES cannot be removed by dialysis. This applies to both haemodialysis and peritoneal dialysis.
Urinary excretion is via glomerular filtration. No tubular secretion takes place. For this reason, no increase in the serum levels is to be expected in coincident administration of probenecid and is actually - even at higher dosage e.g. with 1-2 g probenecid - not found. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageMicrobiology: ELORES, the combination of Ceftriaxone sodium, Sulbactam sodium and Disodium Edetate is active against wide range of Gram-positive and Gram-negative aerobic ESBL pathogens, carbapenemase producing (MBL), efflux overexpressed and biofilm producing pathogens. ELORES exhibits synergistic activity against TEM, SHV, Amp C, VIM, IMP, KPC, NDM-1, Van A, Mec A, AcrAB, and Tol C genes expressing strains.
Gram-negative aerobes: Acinetobacter spp4, Enterobacter spp.3, Neisseria meningitidis*, Citrobacter koseri1, Escherichia coli*1,4, Haemophilus influenzae*, Haemophilus parainfluenzae*, Klebsiella pneumoniae*1,4, Klebsiella oxytoca*1,4, Moraxella catarrhalis*, Morganella morganii1, Proteus mirabilis*1, Proteus vulgaris1, Providencia spp.1, Salmonella spp.1, Serratia spp.1 , Shigella spp., Neisseria gonorrhoeae, Pseudomonas spp2.
Gram-positive aerobes: Staphylococcus aureus* (MSSA), Streptococcus agalactiae, Streptococcus bovis, Streptococcus pyogenes*, Streptococcus pneumoniae*.
Elores exhibits mild to moderate activity against species with acquired resistance.
Gram-positive aerobes: Staphylococcus epidermidis* (MSSE).
Gram-negative aerobes: Enterobacter spp.1,3, Citrobacter freundii1.
Inherently resistant species: Gram-positive aerobes: Enterococcus faecalis, Enterococcus faecium, Listeria monocytogenes, Staphylococcus aureus (MRSA), Staphylococcus epidermidis (MRSE).
Gram-positive anaerobes: Clostridium difficile, Peptococcus niger, Peptostreptococcus spp.
Gram-negative aerobes: Achromobacter spp., Aeromonas spp., Alcaligenes spp., Flavobacterium spp., Legionella gormanii.
Gram-negative anaerobes: Bacteroides spp.
Others: Chlamydia spp., Chlamydophila spp., Mycobacterium spp., Mycoplasma spp., Rickettsia spp., Ureaplasma urealyticum.
*Clinical efficacy has been demonstrated for ESBL producing resistant and susceptible isolates species with natural intermediate susceptibility to carbapenems.
1. Some strains produce inducible or stably derepressed chromosomally-encoded cephalosporinases and ESBLs (extended spectrum beta-lactamases) and thus are clinically resistant to cephalosporins.
2. In suspected or proven Pseudomonas infection with NDM-1.
3. Clinical efficacy has been demonstrated for susceptible isolates of Enterobacter cloacae and Enterobacter aerogenes in approved clinical indications.
4. KPC and/or MBL producing strains found resistant to carbapenems.
Susceptibility testing methods: As is recommended with all antimicrobials, the results of in vitro susceptibility tests, when available, should be provided to the physician as a periodic reports, which describe the susceptibility profile of nosocomial and community-acquired pathogens. These reports should aid the physician in selecting the most effective antimicrobial.
Dilution Techniques: Quantitative methods are used to determine antimicrobial minimum inhibitory concentrations (MICs). These MICs provide estimates of the susceptibility of bacteria to antimicrobial compounds. The MICs should be determined using a standardized procedure.
Standardized procedures are based on a dilution method (broth or agar) or equivalent with standardized inoculum concentrations and standardized concentrations of Ceftriaxone Sodium, Disodium Edetate, Sulbactam sodium powders. MIC values should be determined using serial dilutions of ceftriaxone sodium, sulbactam sodium combined with disodium edetate. MIC interpretive criteria is based on a dosage regimen of 1.5 g ELORES every 24 hrs.
Diffusion technique: Quantitative methods that require measurement of zone diameters also provide reproducible estimates of the susceptibility of bacteria to antimicrobial compounds. One such standardized procedure requires the use of standardized inoculum concentrations.
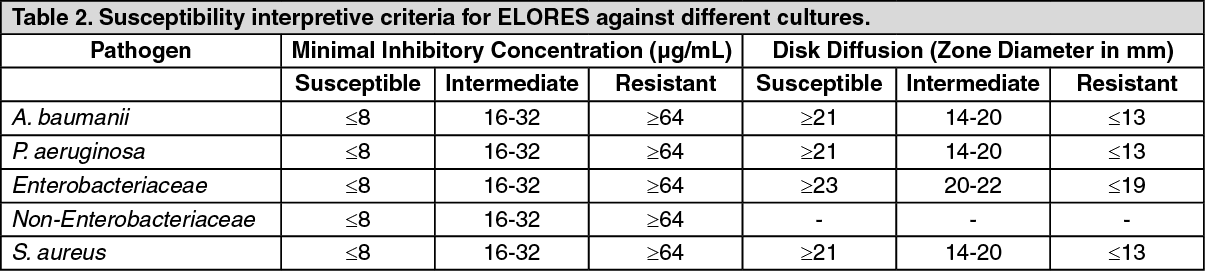
This procedure uses paper disks impregnated with 30 µg of Ceftriaxone and 15 µg of Sulbactam and 10 µg of disodium edetate to test the susceptibility of microorganisms to ELORES. The disk diffusion interpreted criteria are provided in Table 2. (See Table 2.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageA report of Susceptible (S) indicates that the pathogen is likely to respond to therapy. A report of Intermediate (I) indicates that the organism would be susceptible if the infection were confined to tissues and fluids (e.g., urine), in which high antibiotic levels were attained. A report of Resistant (R) suggests that the pathogen is not likely to respond to the therapy.