


 Sign Out
Sign Out


Clinical Trial Experience: Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and also may not reflect rates observed in practice.
Complicated Intra-abdominal Infections and Complicated Urinary Tract Infections, including Pyelonephritis: ZERBAXA was evaluated in Phase 3 comparator-controlled clinical trials of cIAI and cUTI, which included a total of 1015 patients treated with ZERBAXA (1.5 g every 8 hours, adjusted based on renal function where appropriate) and 1032 patients treated with comparator (levofloxacin 750 mg daily in cUTI or meropenem 1 g every 8 hours in cIAI) for up to 14 days. The mean age of treated patients was 48 to 50 years (range 18 to 92 years), across treatment arms and indications. In both indications, about 25% of the subjects were 65 years of age or older. Most patients (75%) enrolled in the cUTI trial were female, and most patients (58%) enrolled in the cIAI trial were male. Most patients (>70%) in both trials were enrolled in Eastern Europe and were White.
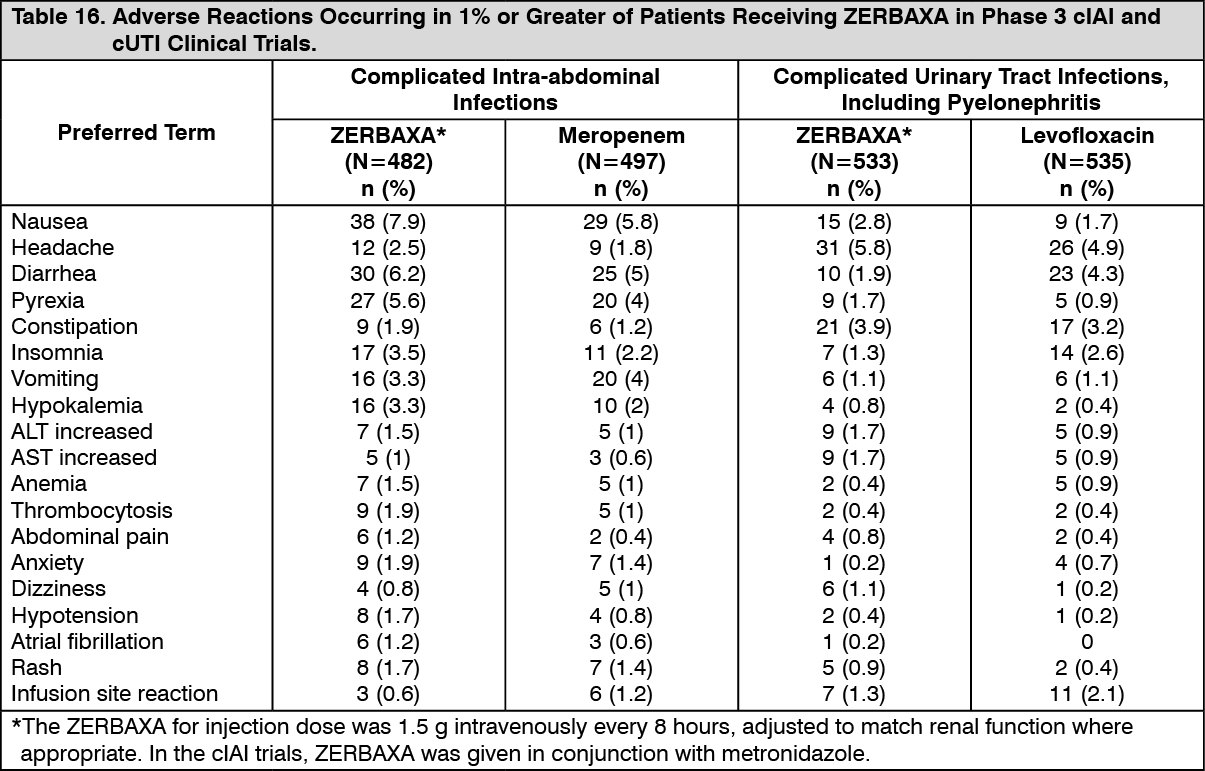
The most common adverse reactions (5% or greater in either indication) occurring in patients receiving ZERBAXA were nausea, diarrhea, headache, and pyrexia. Table 16 lists adverse reactions occurring in 1% or greater of patients receiving ZERBAXA in Phase 3 cIAI and cUTI clinical trials. (See Table 16.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageTreatment discontinuation due to adverse events occurred in 2.0% (20/1015) of patients receiving ZERBAXA and 1.9% (20/1032) of patients receiving comparator drugs. Renal impairment (including the terms renal impairment, renal failure, and renal failure acute) led to discontinuation of treatment in 5/1015 (0.5%) subjects receiving ZERBAXA and none in the comparator arms.
Increased Mortality: In the cIAI trials (Phase 2 and 3), death occurred in 2.5% (14/564) of patients receiving ZERBAXA and in 1.5% (8/536) of patients receiving meropenem. The causes of death varied and included worsening and/or complications of infection, surgery and underlying conditions.
Less Common Adverse Reactions in Phase 3 cIAI and cUTI Clinical Trials: The following selected adverse reactions were reported in ZERBAXA-treated subjects at a rate of less than 1%: Cardiac disorders: tachycardia, angina pectoris.
Gastrointestinal disorders: gastritis, abdominal distension, dyspepsia, flatulence, ileus paralytic.
Infections and infestations: candidiasis including oropharyngeal and vulvovaginal, fungal urinary tract infection.
Investigations: increased serum gamma-glutamyl transpeptidase (GGT), increased serum alkaline phosphatase, positive Coombs test.
Metabolism and nutrition disorders: hyperglycemia, hypomagnesemia, hypophosphatemia.
Nervous system disorders: ischemic stroke.
Renal and urinary system: renal impairment, renal failure.
Respiratory, thoracic and mediastinal disorders: dyspnea.
Skin and subcutaneous tissue disorders: urticaria.
Vascular disorders: venous thrombosis.
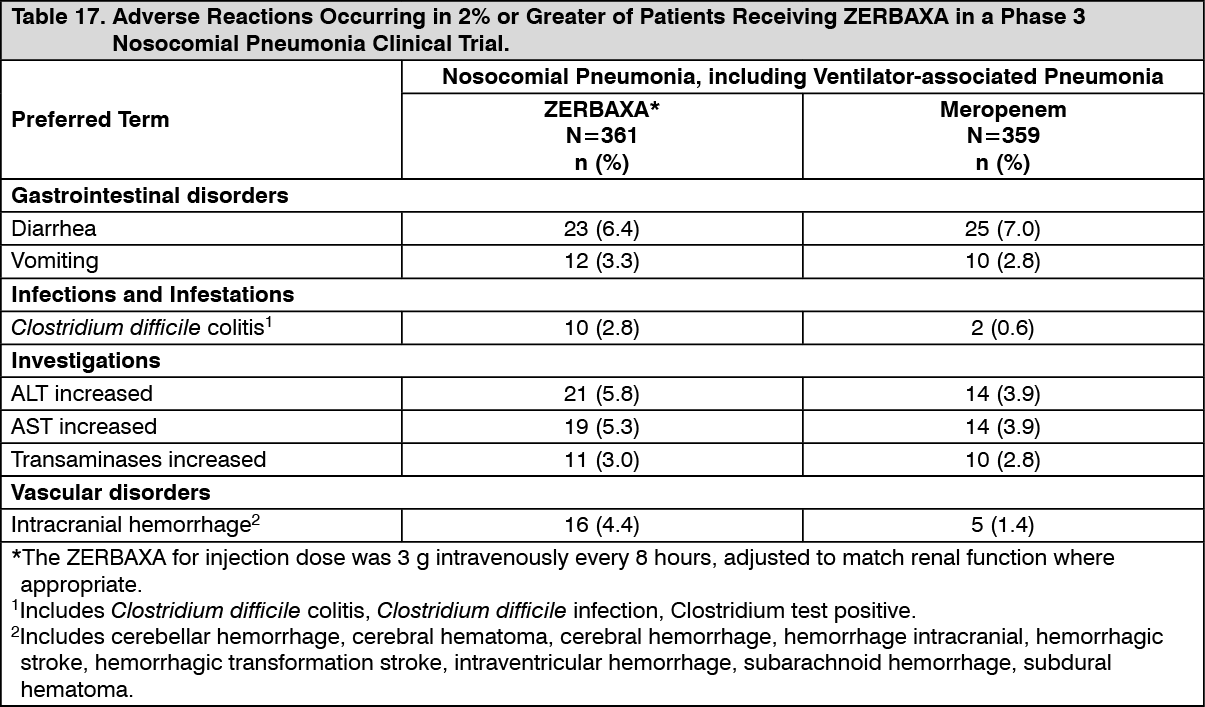
Nosocomial Pneumonia, including Ventilator-associated Pneumonia: ZERBAXA was evaluated in a Phase 3 comparator-controlled clinical trial for nosocomial pneumonia, which included a total of 361 patients treated with ZERBAXA (3 g every 8 hours, adjusted based on renal function where appropriate) and 359 patients treated with comparator (meropenem 1 g every 8 hours) for up to 14 days. The mean age of treated patients was 60 years (range 18 to 98 years), across treatment arms. About 44% of the subjects were 65 years of age or older. Most patients (71%) enrolled in the trial were male. All subjects were mechanically ventilated and 92% were in an intensive care unit (ICU) at randomization. The median APACHE II score was 17 and 33% of subjects had a baseline APACHE II score of ≥20, indicating a high severity of illness for many patients enrolled in this trial. Table 17 lists adverse reactions occurring in 2% or greater of patients receiving ZERBAXA in a Phase 3 nosocomial pneumonia clinical trial. (See Table 17.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageTreatment discontinuation due to treatment-related adverse events occurred in 1.1% (4/361) of patients receiving ZERBAXA and 1.4% (5/359) of patients receiving meropenem.
Less Common Adverse Reactions in a Phase 3 Nosocomial Pneumonia Clinical Trial: The following selected adverse reactions were reported in ZERBAXA-treated subjects at a rate of less than 2%: Infections and infestations: Clostridium difficile infection.
Investigations: liver function test abnormal, blood alkaline phosphatase increased, gamma-glutamyltransferase increased, Clostridium test positive, Coombs direct test positive.
Laboratory Values: The development of a positive direct Coombs test may occur during treatment with ZERBAXA. The incidence of seroconversion to a positive direct Coombs test was 0.2% in patients receiving ZERBAXA and 0% in patients receiving the comparator in the cUTI and cIAI clinical trials. The incidence of seroconversion to a positive direct Coombs test was 31.2% in patients receiving ZERBAXA and 3.6% in patients receiving meropenem in the nosocomial pneumonia clinical trial. In clinical studies, there was no evidence of hemolysis in patients who developed a positive direct Coombs test in any treatment group.
View ADR Monitoring Form