Pharmacotherapeutic group: other systemic drugs for obstructive airway diseases.
ATC code: R03DX05.
Pharmacology: Pharmacodynamics: General characteristics: Omalizumab is a recombinant DNA-derived humanized monoclonal antibody that selectively binds to human immunoglobulin E (IgE). The antibody is an IgG1 kappa that contains human framework regions with the complementary-determining regions of a murine parent antibody that binds to IgE.
Patients with allergic asthma and chronic rhinosinusitis with nasal polyps (CRSwNP): IgE plays a central effector role in the pathophysiology of inflammatory diseases in the airway. The allergic cascade is initiated when IgE bound to the high affinity IgE receptor, FcεRI, on the surface of mast cells and basophils is cross-linked by allergen. This results in the degranulation of these effector cells and the release of histamines, leukotrienes, cytokines and other mediators. These mediators are causally linked to the pathophysiology of allergic asthma including airway edema, smooth muscle contraction and altered cellular activity associated with the inflammatory process. They also contribute to the signs and symptoms of allergic disease such as bronchoconstriction, mucus production, wheezing, dyspnea, chest tightness, nasal congestion, sneezing, itchy, runny nose and itchy, watery eyes. Omalizumab binds to IgE and prevents binding of IgE to FcεRI, thereby reducing the amount of free IgE that is available to trigger the allergic cascade. Treatment of atopic subjects with omalizumab resulted in a marked down-regulation of FcεRI receptors. Furthermore, the
in vitro histamine release from basophils isolated from Xolair-treated subjects was reduced by approximately 90% following stimulation with an allergen compared to pre-treatment values. Treatment with Xolair inhibits IgE-mediated inflammation, as evidenced by reduced blood and tissue eosinophils and reduced inflammatory mediators, including IL-4, IL-5, and IL-13 by innate, adaptive and non-immune cells.
Patients with allergic asthma: In clinical studies in asthma patients, free IgE levels in serum were reduced in a dose-dependent manner within one hour following the first dose and maintained between doses. Mean decrease in free IgE in serum was greater than 96% using recommended doses. Total IgE levels (i.e., bound and unbound) in serum increased after the first dose due to the formation of omalizumab:IgE complexes which have a slower elimination rate compared with free IgE. At 16 weeks after the first dose, average serum total IgE levels were five-fold higher compared with pre-treatment levels when using standard assays. After discontinuation of Xolair dosing, the Xolair induced increase in total IgE and decrease in free IgE were reversible, with no observed rebound in IgE levels after drug washout. Total IgE levels did not return to pre-treatment levels for up to one year after discontinuation of Xolair.
Patients with chronic rhinosinusitis with nasal polyps (CRSwNP): In clinical studies in patients with CRSwNP, Xolair treatment led to a reduction in serum free IgE and an increase in serum total IgE levels, similar to the observations in patients with allergic asthma. After repeated dosing every 2 or 4 weeks, with dosage and frequency according to Tables 7 and 8 (see Dosage & Administration), mean pre-dose serum free IgE levels decreased by approximately 95% and remained stable between 16 and 24 weeks of treatment. Total IgE levels in serum increased due to the formation of omalizumab-IgE complexes, which have a slower elimination rate compared with free IgE. After repeated dosing every 2 or 4 weeks, with dosage and frequency according to Tables 7 and 8 (see Dosage & Administration), mean pre-dose serum total IgE levels at Week 16 were 3- to 4-fold higher compared with pre-treatment levels, and remained stable between 16 and 24 weeks of treatment.
Patients with Chronic Spontaneous Urticaria (CSU): There are several theories for the etiology of CSU, including one that suggests an autoimmune origin. Autoimmune antibodies to IgE and its receptor, FcεRI, have been isolated from the serum of some patients with CSU. These autoantibodies can activate basophils or mast cells leading to release of histamine.
One hypothesis for the mechanism of action of omalizumab in CSU is that it lowers free IgE levels in the blood and subsequently in the skin. This leads to down-regulation of surface IgE receptors, thereby decreasing downstream signaling via the FcεRI pathway, resulting in suppressed cell activation and inflammatory responses. As a consequence, the frequency and severity of symptoms of CSU are lessened. Another hypothesis is that lowering circulating free IgE levels leads to a rapid and non-specific desensitization of cutaneous mast cells. Down-regulation of FcεRI may help to sustain the response.
In clinical studies in CSU patients, omalizumab treatment led to a dose-dependent reduction of free IgE and an increase of total IgE levels in serum, similar to the observations in allergic asthma patients. Maximum suppression of free IgE was observed 3 days after the first subcutaneous dose. After repeated dosing once every 4 weeks, pre-dose serum free IgE levels remained stable between 12 and 24 weeks of treatment. Total IgE levels in serum increased after the first dose due to the formation of omalizumab:IgE complexes which have a slower elimination rate compared with free IgE. After repeated dosing once every 4 weeks at 75 mg to 300 mg, average pre-dose serum total IgE levels at week 12 were two-to three-fold higher compared with pre-treatment levels, and remained stable between 12 and 24 weeks of treatment. After discontinuation of Xolair, free IgE levels increased and total IgE levels decreased towards pre-treatment levels over a 16-week treatment-free follow-up period.
Clinical Studies: Allergic Asthma: Adults and adolescents ≥12 years of age: The safety and efficacy of Xolair were evaluated in five randomized, double-blind, placebo-controlled, multi-center trials.
In identical 16-week studies 1 and 2, the safety and efficacy of omalizumab as add-on therapy were demonstrated in 1,071 allergic asthmatics, who were symptomatic despite treatment with inhaled corticosteroids (beclomethasone dipropionate 500 to 1,200 micrograms/day).
In both trials, omalizumab was superior to placebo with respect to the primary variable of asthma exacerbation (worsening of asthma requiring systemic corticosteroids or a doubling of the patient's baseline beclomethasone dose). The number of asthma exacerbations was significantly lower in the omalizumab group (p=0.006 and p<0.001 in studies 1 and 2, respectively). Fewer omalizumab-treated patients experienced asthma exacerbations (14.6% vs 23.3%, p=0.009 in study 1 and 12.8% vs 30.5%, p<0.001 in study 2).
In double-blind extension phases of both studies out to one year the reduction in the frequency of asthma exacerbations for omalizumab-treated patients compared to placebo-treated patients was maintained.
In studies 1 and 2, clinically meaningful improvement in asthma-related quality of life, measured by the validated Juniper's Asthma Quality of Life Questionnaire, was demonstrated in the Xolair group at the end of the 28-week core trial compared to that observed in the placebo treated group (difference from placebo p ≤0.001 in studies 1 and 2).
In study 3, the safety and corticosteroid-sparing effect of omalizumab was demonstrated in 246 patients with severe allergic asthma requiring daily treatment with high-dose inhaled corticosteroids (fluticasone ≥1,000 micrograms/day) and in whom long-acting beta2-agonists were allowed. The study included a 16-week steroid stable phase with study medication added, followed by a 16-week steroid reduction phase. The percent reduction in inhaled corticosteroid dose at the end of the treatment phase was significantly greater in omalizumab-treated patients versus placebo patients (median 60% vs. 50%, p=0.003). The proportion of omalizumab patients who were able to reduce their fluticasone dose to ≤500 micrograms/day was 60.3% versus 45.8% in the placebo group.
In study 4, the safety and efficacy of omalizumab were demonstrated in 405 patients with co-morbid allergic asthma and perennial allergic rhinitis. Eligible patients had both symptomatic allergic asthma and perennial allergic rhinitis. Patients were treated with omalizumab or placebo for 28 weeks as add-on therapy to ≥400 micrograms of Budesonide Turbohaler. Inhaled long-acting beta2-agonists (39%) and nasal corticosteroids (17%) were allowed.
The co-primary endpoints for study 4 were the incidence of asthma exacerbations (worsening of asthma requiring systemic corticosteroids or a doubling of the patient's baseline budesonide dose) and the proportion of patients in each treatment group with a ≥1.0 improvement from baseline at the end of the treatment phase in both asthma and rhinitis specific quality of life assessments (Juniper Quality of Life Assessment).
Patients treated with omalizumab had a significantly lower incidence of asthma exacerbations than patients receiving placebo (20.6% omalizumab vs 30.1% placebo, p=0.02) and there was a significantly higher proportion of omalizumab-treated than placebo patients that improved by ≥1.0 points in both asthma and rhinitis specific quality of life assessments (57.7% omalizumab vs 40.6% placebo, p<0.0001).
The reduction in exacerbations and improvements of quality of life in omalizumab-treated patients were seen in the context of statistically significant improvements in both rhinitis and asthma symptoms, and lung function, compared to placebo.
In study 5, the efficacy and safety of Xolair were demonstrated in a 28-week study involving 419 severe allergic asthmatics, ages 12 to 79 years, who had reduced lung function (Forced Expiratory Volume/1 second: FEV
1 40 to 80% predicted) and poor asthma symptom control despite receiving >1,000 micrograms of beclomethasone dipropionate (or equivalent) plus long-acting beta2-agonist. Eligible patients had experienced multiple asthma exacerbations requiring systemic corticosteroid treatment or had been hospitalised or attended an emergency room due to a severe asthma exacerbation in the past year despite continuous treatment with high-dose inhaled corticosteroids and long-acting beta2-agonist. Subcutaneous Xolair or placebo were administered as add-on therapy to >1,000 micrograms beclomethasone dipropionate (or equivalent) plus long-acting beta2-agonist. Oral corticosteroid (22%), theophylline (27%) and anti-leukotriene (35%) maintenance therapies were allowed. In the treatment phase concomitant asthma therapy was not changed.
The rate of asthma exacerbations requiring treatment with bursts of systemic corticosteroids was the primary endpoint. Omalizumab reduced the rate of asthma exacerbations by 19% (p=0.153). Further evaluations which did show statistical significance (p<0.05) in favour of Xolair included reductions in severe exacerbations (where patient's lung function was reduced to below 60% of personal best and requiring systemic corticosteroids) and asthma-related emergency visits (comprised of hospitalisations, emergency room, and unscheduled doctor visits), and improvements in Physician's overall assessment of treatment effectiveness, Asthma-related Quality of Life (AQL), asthma symptoms and lung function. A physician's overall assessment was performed in the five previously mentioned studies as a broad measure of asthma control performed by the treating physician. The physician was able to take into account Peak Expiratory Flow (PEF), day and night time symptoms, rescue medication use, spirometry and exacerbations. In all five studies, a significantly greater proportion of Xolair-treated patients were judged to have achieved either a marked improvement or complete control of their asthma compared to placebo patients.
Children 6 to <12 years of age: The primary support for safety and efficacy of Xolair in the 6 to <12 years of age group comes from one randomized, double-blind, placebo-controlled, multi-center trial (study 6) and an additional supportive study (study 7).
Study 6 was a 52-week study that evaluated the safety and efficacy of Xolair as add-on therapy in 628 allergic asthmatics who were uncontrolled despite treatment with regular inhaled corticosteroids (fluticasone DPI ≥200 mcg/day or equivalent) with or without other controller asthma medications. Eligible patients were those with a diagnosis of asthma >1 year and a positive skin prick test to at least one perennial aeroallergen and a history of clinical features of moderate to severe persistent asthma including daytime and/or night-time symptoms along with a history of experiencing exacerbations within the year prior to study entry. Long-acting beta2-agonists (67.4%), anti-leukotriene (36.6%) and oral corticosteroid (1.3%) maintenance therapies were allowed. During the first 24 weeks of treatment, a patient's steroid doses remained constant from baseline and this was followed by a 28-week period during which inhaled corticosteroid adjustment was allowed.
A clinically significant exacerbation was defined as a worsening of asthma symptoms as judged clinically by the investigator, requiring doubling of the baseline inhaled corticosteroid dose for at least 3 days and/or treatment with rescue systemic (oral or IV (intravenous)) corticosteroids for at least 3 days.
Exacerbation rates during the 52-week double-blind treatment period in Xolair patients with FEV
1 >80% at baseline had relative decreases of 43% in asthma exacerbations compared with placebo (p<0.001). Xolair patients had statistically significant reduction in the rate of asthma exacerbations irrespective of concomitant long-acting beta2-agonist use at baseline compared with placebo patients, representing a 45% decrease for long-acting beta2-agonist users and a 42% decrease for long-acting beta2-agonist non-users (p<0.001 and p=0.011, respectively).
Study 7 was a 28-week randomized, double-blind, placebo-controlled study primarily evaluating safety in 334 children, aged 6 to 12 years of age, with asthma who were well controlled with inhaled corticosteroids. During the first 16 weeks of treatment, patients' steroid doses remained constant from baseline and this was followed by a 12-week steroid dose reduction period. The study assessed percent reduction in the dose of beclomethasone dipropionate (BDP) and the proportion of patients with a reduction in the dose of BDP at 28 weeks. The percent reduction in the dose of BDP at 28 weeks was higher in the Xolair group than in the placebo group (median reduction 100% vs. 66.7%, p=0.001) as well as the proportion of patients with a reduction in the dose of BDP (p=0.002). Frequency and incidence of asthma exacerbation episodes during the steroid dose-reduction phase were also lower in the omalizumab group (mean rate 0.42 vs. 0.72, p<0.001; percent patients with exacerbations 18% vs. 39%, p<0.001). A trend for superiority of omalizumab with respect to reduction of exacerbation frequency and incidence was evident during the first 16 weeks of the 24-week treatment period. 55.7% of omalizumab patients had a complete (100%) reduction in corticosteroid dose at the end of the 28-week treatment period compared with 43.2% of placebo patients. In addition, more omalizumab patients had a ≥50% reduction in corticosteroid dose compared with placebo (80.4% vs. 69.5%. p=0.017).
A physician's overall assessment was performed in the two previously mentioned studies (6 and 7) as a broad measure of asthma control performed by the treating physician. The physician was able to take into account PEF, day and night time symptoms, rescue medication use, spirometry and exacerbations. In both studies, a significantly greater proportion of Xolair-treated patients were judged to have achieved either a marked improvement or complete control of their asthma compared to placebo patients.
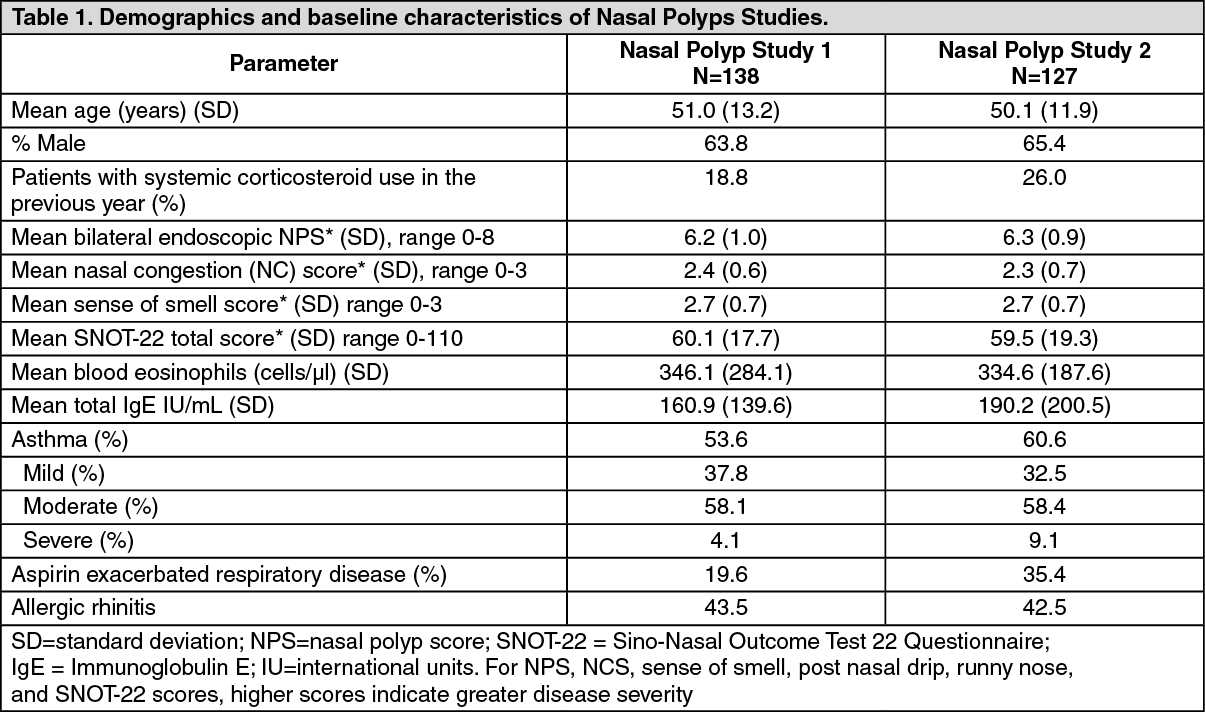
Chronic rhinosinusitis with nasal polyps (CRSwNP): The safety and efficacy of Xolair were evaluated in two randomized, multi-center, double-blind, placebo-controlled clinical trials that enrolled patients with chronic rhinosinusitis with nasal polyps (study 1, N=138; study 2, N=127). Patients received Xolair or placebo subcutaneously every 2 or 4 weeks, with dosage and frequency according to Tables 7 and 8 (see Dosage & Administration). All patients received background intranasal mometasone therapy throughout the study. Prior sino-nasal surgery or prior systemic corticosteroid usage were not required for inclusion in the studies. Patients received Xolair or placebo for 24 weeks followed by a 4-week follow-up period. Demographics and baseline characteristics, including allergic comorbidities, are described in Table 1. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
The co-primary endpoints were bilateral nasal polyp score (NPS) and average daily nasal congestion score (NCS) at Week 24. NPS was measured via endoscopy at baseline and pre-specified time points and scored (range 0-4 per nostril) for a total NPS (range 0/best-8/worst). Nasal congestion was measured by a daily NCS (range 0/best-3/worst). Patients were required to have NPS ≥ 5 and weekly average of NCS > 1 prior to randomization, despite use of intranasal mometasone. The mean NPS at baseline was balanced between the two treatment groups in both studies.
In both nasal polyps studies 1 and 2, patients who received Xolair had a statistically significant greater improvement from baseline at Week 24 in NPS and weekly average NCS than patients who received placebo. Results from Nasal Polyps Study 1 and 2 are shown in Table 2.
The greater improvements in NPS and NCS in the Xolair group compared to the placebo group were observed as early as the first assessment at Week 4 in both studies as seen in Figure 1. The LS mean difference in change from baseline at Week 4 in NPS in Xolair compared to placebo was -0.92 (95% CI: -1.37, -0.48) in study 1 and -0.52 (95% CI: -0.94, -0.11) in study 2. The LS mean difference in change from baseline at Week 4 in NCS in Xolair compared to placebo was -0.25 (95% CI: -0.46, -0.04) in study 1 and -0.26 (95% CI: -0.45, -0.07) in study 2. However, statistical tests at this time point were not pre-specified. (See Table 2 and Figure 1.)
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
A key secondary endpoint was the assessment of the change from baseline at Week 24 of the total nasal symptom score (TNSS). Patient-reported TNSS was the sum of four equally weighted individual daily symptom scores: NCS, sense of smell score, posterior rhinorrhea score, and anterior rhinorrhea score. The TNSS ranged from 0/best-12/worst. Xolair significantly improved the average daily TNSS compared to placebo. The LS mean difference for change from baseline to Week 24 was -1.91 points (95% CI: -2.85, -0.96; p=0.0001) in study 1 and -2.09 points (95% CI: -3.00, -1.18; p<0.0001) in study 2.
Xolair significantly improved SNOT-22 (Sino-Nasal Outcome Test), which combines measures of sino-nasal symptoms with psychological and sleep dysfunction measures. The SNOT-22, ranged from 0 to 110 (0/best-110/worst). The LS mean difference for change from baseline to Week 24 in SNOT-22 in Xolair compared to placebo was -16.12 (95% CI: -21.86, -10.38; p<0.0001) in study 1 and -15.04 (95% CI: -21.26, -8.82; p<0.0001) in study 2.
Xolair also significantly improved the average daily UPSIT (University of Pennsylvania Sell Identification Test) compared to placebo. The UPSIT ranged from 0 to 40 (0/worst-40/best). The LS mean difference for change from baseline to Week 24 in Xolair compared to placebo was 3.81 points (95% CI: 1.38, 6.24; p=0.0024) in study 1 and 3.86 points (95% CI: 1.57, 6.15; p=0.0011) in study 2.
The effect on TNSS and SNOT-22 was observed as early as the first assessment at week 4 in both studies. Additionally, the effect on UPSIT was observed at the first assessment at week 8 in both studies. The LS mean difference for change from baseline at Week 4 in TNSS in Xolair compared to placebo was -0.97 (95%: -1.61, -0.33) in study 1 and -1.18 (95% Cl: -1.76, -0.59) in study 2. The LS mean difference in change from baseline at Week 4 in SNOT-22 in Xolair compared to placebo was -10.43 (95% CI: -15.08, -5.79) in study 1 and -8.84 (95% CI: -13.84, -3.84) in study 2. The LS mean difference in change from baseline at Week 8 in UPSIT in Xolair compared to placebo was 3.72 (95% Cl: 1.54, 5.90) in study 1 and 5.12 (95% Cl: 2.57, 7.67) in study 2. These analyses were not pre-specified.
Additional secondary endpoint analyses included Week 16 assessments of NPS and NCS. Xolair significantly improved the NPS at week 16, (range 0/best-8/worst) compared to placebo. The LS mean difference for change from baseline to Week 16 in Xolair compared to placebo was -1.01 (95% CI: -1.43, -0.60; p<0.0001) in study 1 and -0.91 (95% CI: -1.39, -0.44; p=0.0002) in study 2. Xolair significantly improved the NCS at week 16, (range 0/best-3/worst) compared to placebo. The LS mean difference for change from baseline to Week 16 in average daily NCS in Xolair compared to placebo was -0.57 (95% CI: -0.83, -0.31; p<0.0001) in study 1 and of -0.59 (95% CI: -0.87, -0.30; p<0.0001) in study 2.
In a pre-specified pooled analysis of rescue treatment (systemic corticosteroids for ≥3 consecutive days or nasal polypectomy) during the 24-week treatment period, the proportion of patients requiring rescue treatment was lower in Xolair compared to placebo (2.3% versus 6.2%, respectively). The odds-ratio of having taken rescue treatment in Xolair compared to placebo was 0.38 (95% CI: 0.10, 1.49). There were no sino-nasal surgeries reported in either study.
Chronic Spontaneous Urticaria (CSU): The clinical Phase III development program for CSU included three randomized, double-blind, placebo-controlled, parallel-group, multi-center studies: Q4881g, Q4882g and Q4883g.
Studies Q4881g and Q4882g evaluated efficacy and safety of administration of 75 mg, 150 mg, or 300 mg Xolair every 4 weeks for 24 and 12 weeks respectively, with a 16-week treatment-free follow-up period in patients (12 to 75 years) with refractory CSU despite H1 antihistamine treatment.
Study Q4883g evaluated safety and efficacy of 300 mg Xolair administered every 4 weeks for 24 weeks, with a 16-week treatment-free follow-up period in patients (12 to 75 years) with refractory CSU despite H1 and/or H2 antihistamine and/or leukotriene receptor antagonist (LTRA) treatment. (See Table 3.)
Click on icon to see table/diagram/image
In studies Q4881g and Q4882g the 75 mg dose did not consistently meet either the primary efficacy endpoint (change from baseline to week 12 in weekly itch severity score) or a number of secondary endpoints. It was deemed not efficacious and therefore not further presented.
Change from baseline to week 12 in weekly itch severity score: The primary efficacy endpoint, change from baseline to week 12 in weekly itch severity score was met by both the 150 mg and 300 mg doses in studies Q4881g and Q4882g and by the 300 mg dose in Q4883g (secondary endpoint: see Table 4).
Click on icon to see table/diagram/image
Figure 2 shows the mean weekly itch severity score over time in study Q4881g. The mean weekly itch severity scores significantly decreased in both treatment groups with a maximum effect around week 12 that was sustained over the 24-week treatment period. In studies Q4883g (300 mg over the 24-week treatment period) and Q4882g (150 mg and 300 mg over the 12-week treatment period) the results were similar to those of study Q4881g.
In all three studies (see Figure 2 for study Q4881g), the mean weekly itch severity score for both doses increased gradually during the 16-week treatment-free follow-up period, consistent with symptom re-occurrence. Mean values at the end of the follow-up period were similar to the placebo group, but lower than respective mean baseline values. (See Figure 2.)
Click on icon to see table/diagram/image
Time to Minimal Important Difference (MID) response of 5 points in weekly ISS up to week 12: In studies Q4881g and Q4882g, the times to attain MID of 5 points on the weekly itch severity score were statistically significantly shorter for patients in the 300 mg treatment groups, compared to the placebo groups with p-value <0.0001. A shorter time was also observed for the 150 mg treatment groups compared to placebo with p=0.0301 in study Q4881g and p=0.0101 in study Q4882g. The median times for attaining MID response were 1 week in the 300 mg treatment group, 2 weeks in the 150 mg groups and 4 weeks for placebo.
Similar results were observed in study Q4883g with p<0.0001 (median time to MID response was 2 weeks in the 300 mg treatment group and 5 weeks in the placebo group).
Change from baseline to week 12 in UAS7: In the phase III studies the omalizumab 150 mg and 300 mg treatment groups showed a statistically significant difference from placebo in mean change from baseline to week 12 in UAS7 (Figure 3 for study Q4881g). Statistical significance (p<0.0001) was achieved in all three studies for the 300 mg treatment group, and in studies Q4881g (p=0.0008) and Q4882g (p=0.0001) for the 150 mg treatment group.
Figure 3 shows mean UAS7 over time in study Q4881g, displaying a significant decrease from baseline in both treatment groups with a maximum effect around week 12. The magnitude of the effect was maintained during the 24-week treatment period. In studies Q4882g (150 mg and 300 mg over the 12-week treatment period) and Q4883g (300 mg over 24-week treatment period) the results were similar to those of study Q4881g.
In all three studies (see Figure 3 for study Q4881g), the UAS7 for both omalizumab treatment groups increased gradually during the 16-week treatment-free follow-up period, consistent with symptom re-occurrence. Mean values at the end of the follow-up period were similar to the placebo group but lower than respective mean baseline values. (See Figure 3.)
Click on icon to see table/diagram/image
Proportion of patients with UAS7 ≤6 at week 12: The proportions of patients with a UAS7 ≤6 at week 12 are shown in Figure 4. The response rates ranged from 52 to 66% (300 mg dose), all were statistically significantly higher compared to 11 - 19% in the placebo group (p<0.0001). The response rates for the 150 mg dose show a notable difference (40 to 43%; p≤0.001) compared to placebo. (See Figure 4.)
Click on icon to see table/diagram/image
Proportion of patients with UAS7 = 0 at week 12: The proportion of patients with a complete response shown by a UAS7 = 0 at week 12 ranged from 34 to 44% (300 mg dose, statistically significant, all p<0.0001) compared to 5 to 9% in the placebo groups. In the 150 mg treatment groups, a clinically notable difference compared to placebo was observed ranging from 15 to 22% (Figure 5). (See Figure 5.)
Click on icon to see table/diagram/image
Changes from baseline in the weekly number of hives score at week 12: In all three phase III studies, the difference from placebo in mean changes from baseline in the weekly number of hives score at week 12 for the 300 mg treatment groups was statistically significant displaying a decrease in number of hives score compared to placebo (-11.35 in Q4881g, -11.97 in Q4882g and -10.46 in Q4883g versus -4.37, -5.22 and -4.49 for the corresponding placebo groups; all p<0.0001). For the 150 mg treatment groups, the mean changes were -7.78 (p=0.0017) in Q4881g and -9.75 (p<0.0001) in Q4882g.
Proportion of angioedema-free days from week 4 to week 12: In all three Phase III studies, the 300 mg treatment groups consistently achieved the highest mean proportion of angioedema-free days from week 4 to week 12 (91 to 96%). The increase in the proportion of angioedema-free days compared to placebo was statistically significant (p<0.001) (Figure 6). In the 150 mg treatment group, the mean proportions of angioedema-free days for the same time period for studies Q4881g and Q4882 were 89.6% and 91.6% respectively. The corresponding placebo values for the same studies were 88.2% and 89.2%. In both of these studies, the differences from placebo did not achieve statistical significance for the 150 mg dose. (See Figure 6.)
Click on icon to see table/diagram/image
Change from baseline to week 12 in overall Dermatology Life Quality Index (DLQI): In all three Phase III studies, the change from baseline to week 12 in the overall DLQI for the 300 mg treatment group was statistically significantly (p<0.001) greater compared to placebo. The 150 mg omalizumab group showed a clinically notable difference to placebo in study Q4882g (p=0.022) (Figure 7). (See Figure 7.)
Click on icon to see table/diagram/image
Efficacy after 24 weeks of treatment: Table 5 shows the results after 24 weeks of treatment. Similar magnitudes of response are seen as at 12 weeks. (See Table 5.)
Click on icon to see table/diagram/image
Pharmacokinetics: General characteristics: Absorption: After subcutaneous administration, omalizumab is absorbed with an average absolute bioavailability of 62%. The pharmacokinetics of omalizumab are linear at doses greater than 0.5 mg/kg.
Administration of Xolair manufactured as a lyophilized or liquid formulation resulted in similar serum concentration-time profiles of omalizumab.
Distribution:
In vitro, omalizumab forms complexes of limited size with IgE. Precipitating complexes and complexes larger than one million Daltons in molecular weight are not observed
in vitro or
in vivo.
Tissue distribution studies in cynomolgus monkeys showed no specific uptake of
125I-omalizumab by any organ or tissue.
Elimination: Clearance of omalizumab involves IgG clearance processes as well as clearance via specific binding and complex formation with its target ligand, IgE. Liver elimination of IgG includes degradation in the liver reticuloendothelial system (RES) and endothelial cells. Intact IgG is also excreted in bile. In studies with mice and monkeys, omalizumab:IgE complexes were eliminated by interactions with Fcgamma receptors within the RES at rates that were generally faster than IgG clearance.
Patients with Allergic Asthma: Absorption: Following a single subcutaneous dose in adult and adolescent patients with asthma, omalizumab was absorbed slowly, reaching peak serum concentrations after an average of 7 to 8 days. Following multiple doses of omalizumab, areas under the serum concentration-time curve from Day 0 to Day 14 at steady state were up to 6-fold of those after the first dose.
Distribution: The apparent volume of distribution of omalizumab in patients with asthma following subcutaneous administration was 78 ± 32 mL/kg.
Elimination: In asthma patients, omalizumab serum elimination half-life averaged 26 days, with apparent clearance averaging 2.4 ± 1.1 mL/kg/day. Doubling of body weight approximately doubled apparent clearance.
Age, Race/Ethnicity, Gender, Body Mass Index: The population pharmacokinetics of omalizumab were analysed to evaluate the effects of demographic characteristics. Analyses of these data suggest that no dose adjustments are necessary in asthma patients for age (6 to 76 years), race, ethnicity, gender or body mass index.
Patients with chronic rhinosinusitis with nasal polyps (CRSwNP): The population pharmacokinetics analyses of omalizumab suggested that pharmacokinetics of omalizumab in CRSwNP were consistent with that in asthma. Graphical covariate analyses were performed to evaluate the effects of demographic characteristics and other factors on omalizumab exposure and clinical responses. These analyses demonstrate that no dose adjustments are necessary for age (18 to 75 years) or gender. Race and ethnicity data are too limited in CRSwNP to inform dose adjustment.
Patients with Chronic Spontaneous Urticaria (CSU): Absorption: Following a single subcutaneous dose in adult and adolescent patients with CSU, omalizumab was absorbed slowly, reaching peak serum concentrations after an average of 6 to 8 days.
In patients with CSU, omalizumab exhibited linear pharmacokinetics across the dose range of 75 mg to 600 mg given as a single subcutaneous dose. Following doses of 75 mg, 150 mg or 300 mg every 4 weeks, trough serum concentrations of omalizumab increased proportionally with the dose level.
Distribution: Based on population pharmacokinetic, distribution of omalizumab in CSU patients was similar to that in patients with allergic asthma.
Elimination: In patients with CSU, based on population pharmacokinetic simulations, omalizumab serum elimination half-life at steady state averaged 24 days and apparent clearance at steady state averaged 240 mL/day (corresponding to 3.0 mL/kg/day for an 80 kg patient).
Age, Race/Ethnicity, Gender, Body Weight, Body Mass Index, Baseline IgE, anti-FcεRI autoantibodies, co-medications: The effects of demographic covariates and other factors on omalizumab exposure were evaluated using population pharmacokinetics. In addition, covariate effects were evaluated by analyzing the relationship between omalizumab concentrations and clinical responses. These analyses suggest that no dose adjustments are necessary in patients with CSU for age (12 to 75 years), race/ethnicity, gender, body weight, body mass index, baseline IgE, anti-FcεRI autoantibodies or concomitant use of H2 antihistamines or leukotriene receptor antagonists (LTRAs).
Patients with renal or hepatic impairment: There are no pharmacokinetic or pharmacodynamic data in patients with renal or hepatic impairment in allergic asthma and CSU patients (see PRECAUTIONS).
Toxicology: Non-Clinical Safety Data: There was no evidence of a systemic anaphylactic response due to mast-cell degranulation in either adult or juvenile cynomolgus monkeys. Circulating omalizumab:IgE antibody complexes were present in all monkey studies, however there was no evidence of immune complex-mediated disease in any organ (including the kidney) following omalizumab administration. Omalizumab: IgE complexes do not fix complement or mediate complement-dependent cytotoxicity.
Chronic administration of omalizumab at dose levels of up to 250 mg/kg (at least 14-fold the highest recommended clinical dose in mg/kg) was well tolerated in non-human primates (both adult and juvenile animals), with the exception of a dose-related decrease in platelet counts that occurred in several non-human primate species, at serum concentrations generally in excess of maximum human exposure in pivotal clinical trials. Juvenile monkeys were more sensitive to the platelet effects than adult monkeys. In addition, acute hemorrhage and inflammation were observed at injection sites in cynomolgus monkeys, consistent with a localized immune response to repeated subcutaneous administration of a heterologous protein. Formal carcinogenicity studies have not been conducted with omalizumab.
Antibodies to omalizumab were detected in some monkeys following subcutaneous or intravenous administration. This was not unexpected based on administration of a heterologous protein. Some animals could not be evaluated because of high serum omalizumab concentrations, high IgE levels, or both. However, the animals maintained high serum omalizumab concentrations throughout the treatment periods of the studies, and there was no apparent toxicity due to the presence of anti-omalizumab antibodies.
Reproduction, milk excretion and fertility studies in animals are described in USE IN PREGNANCY & LACTATION.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image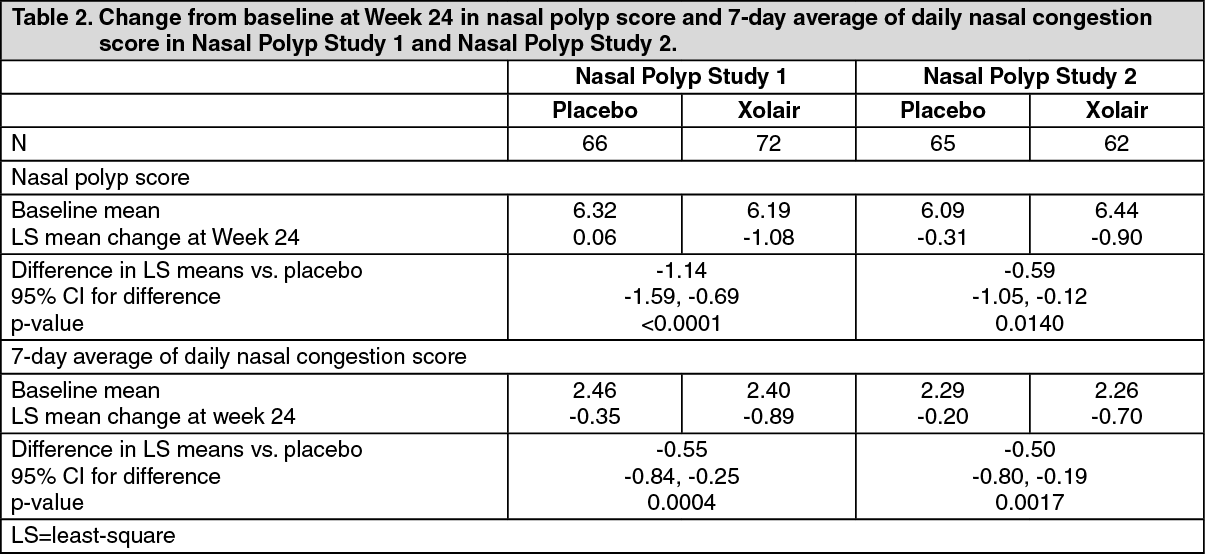 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image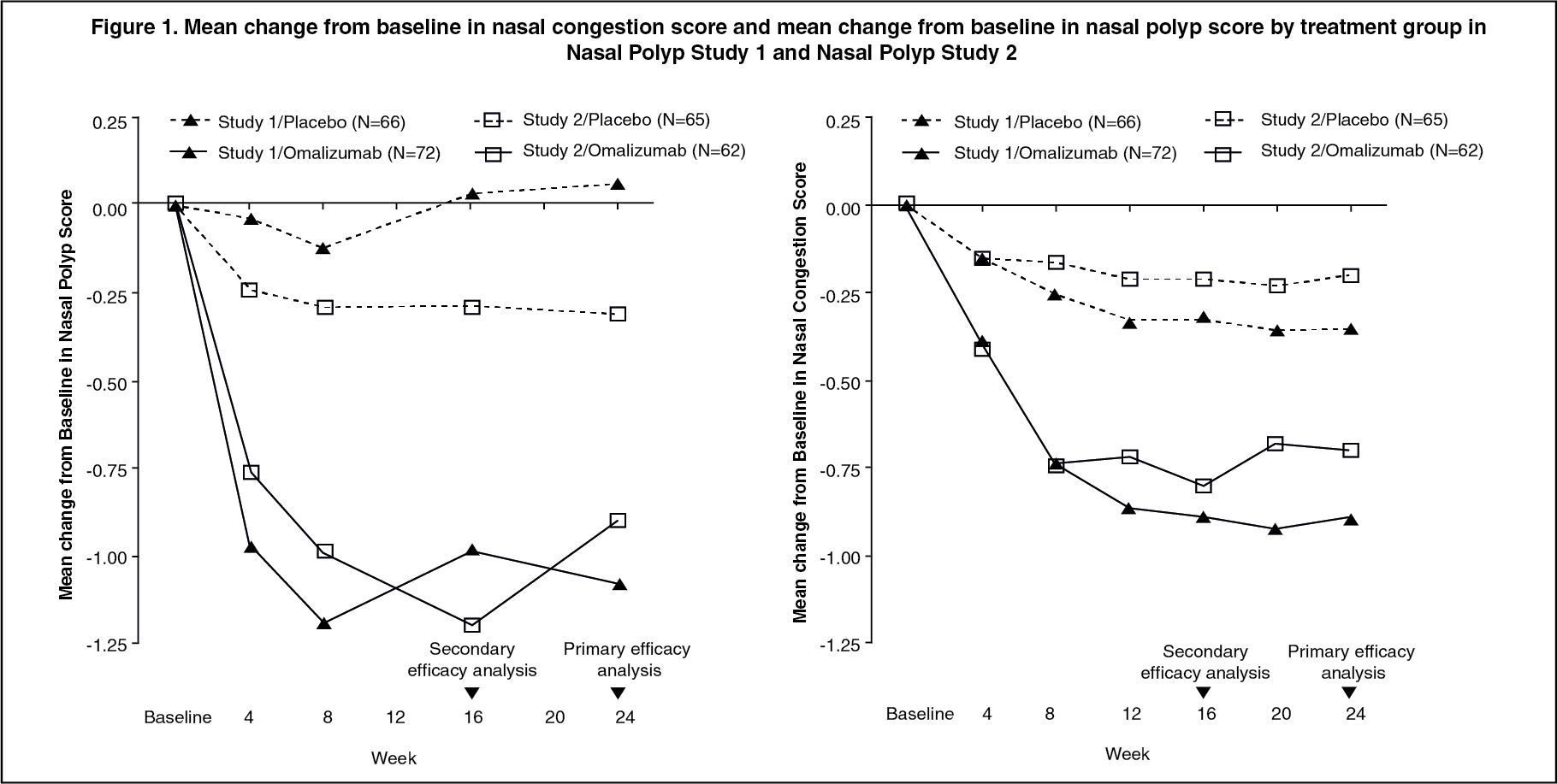 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image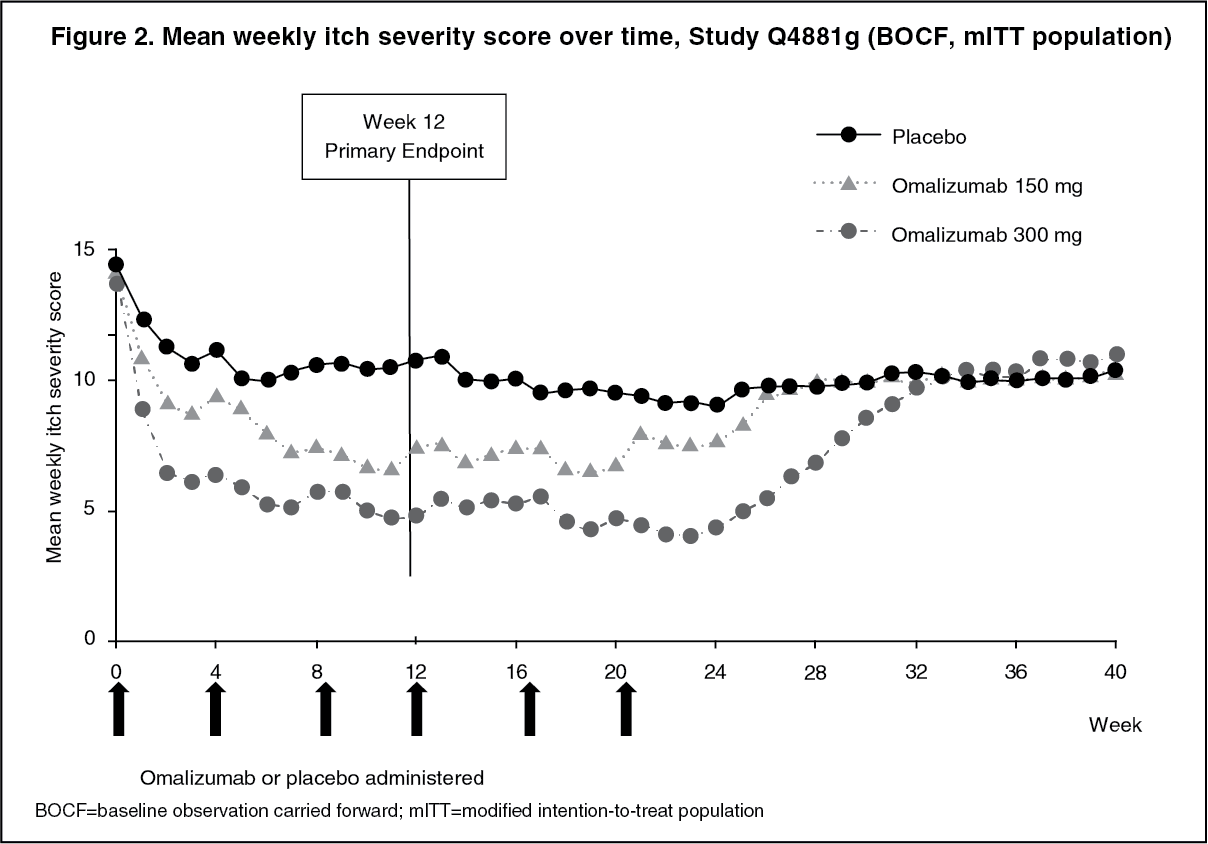 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image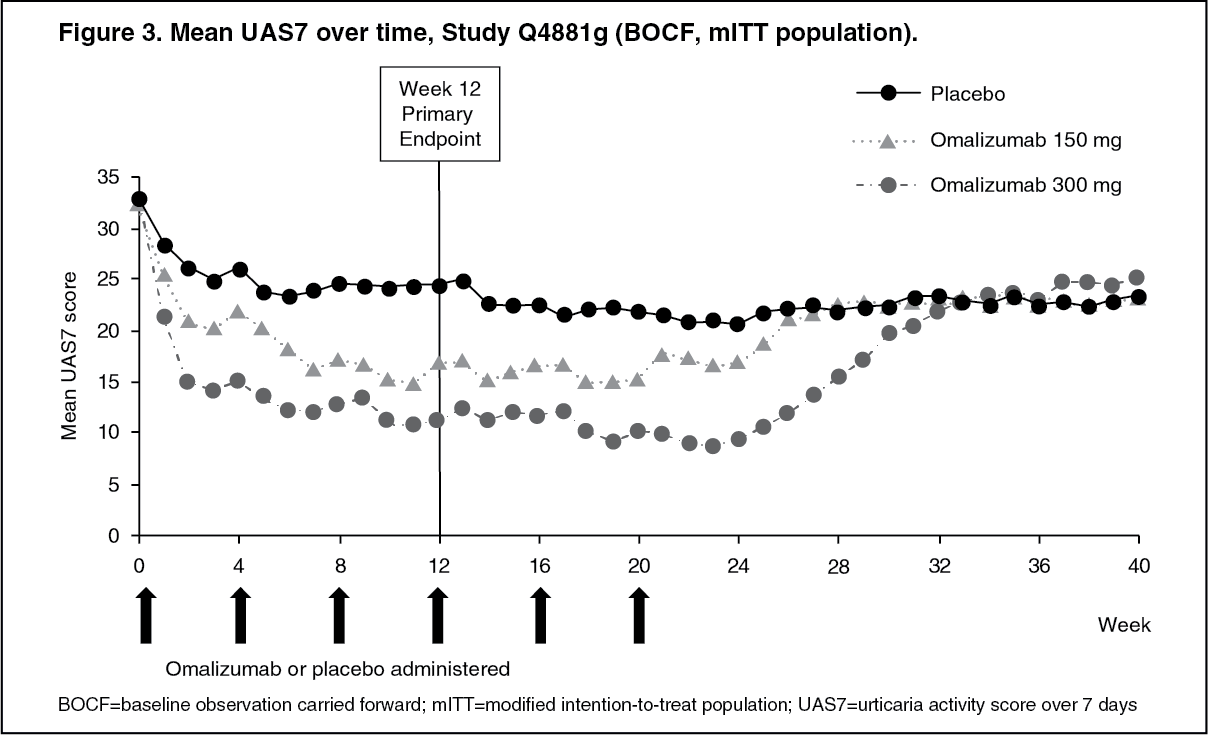 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image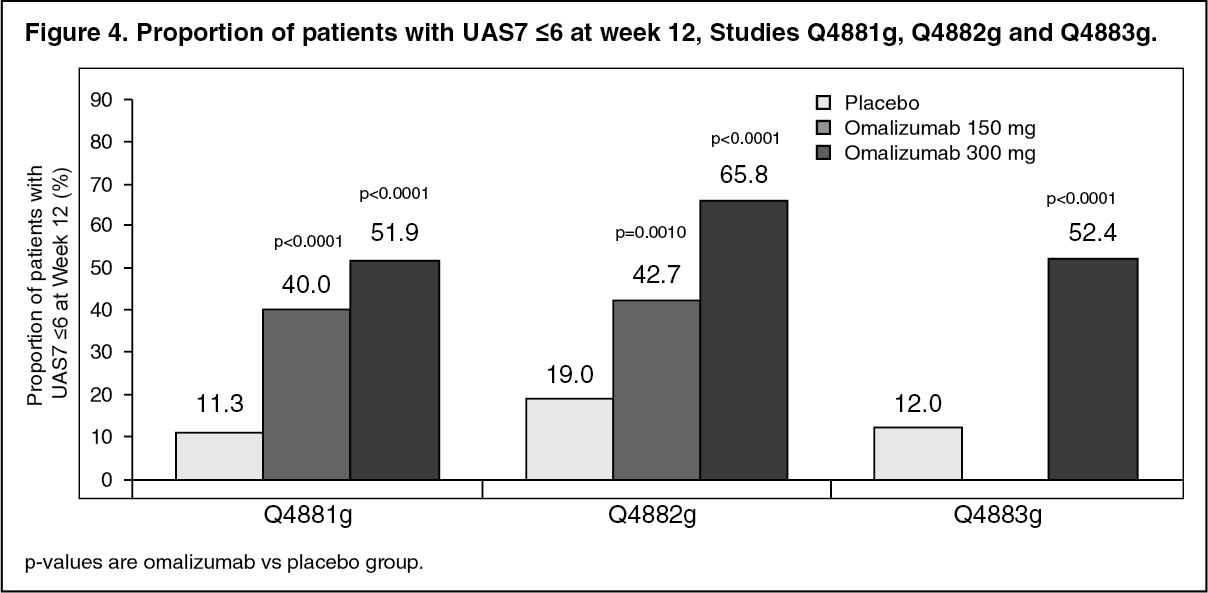 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image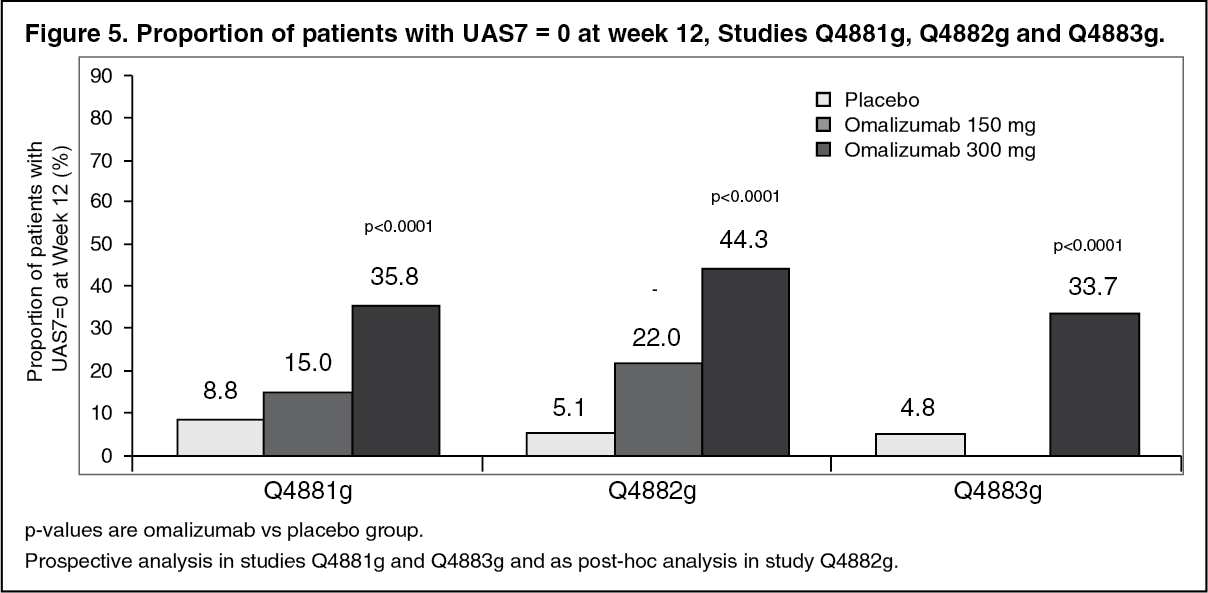 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image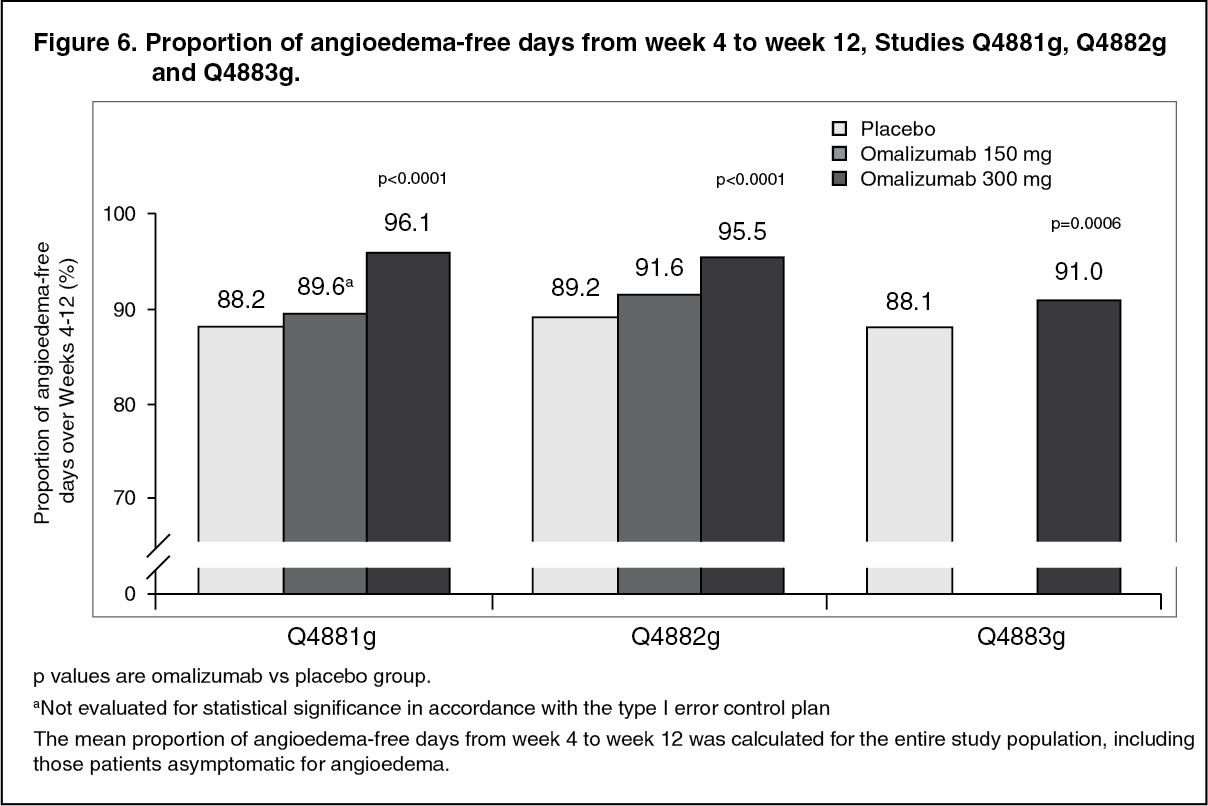 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image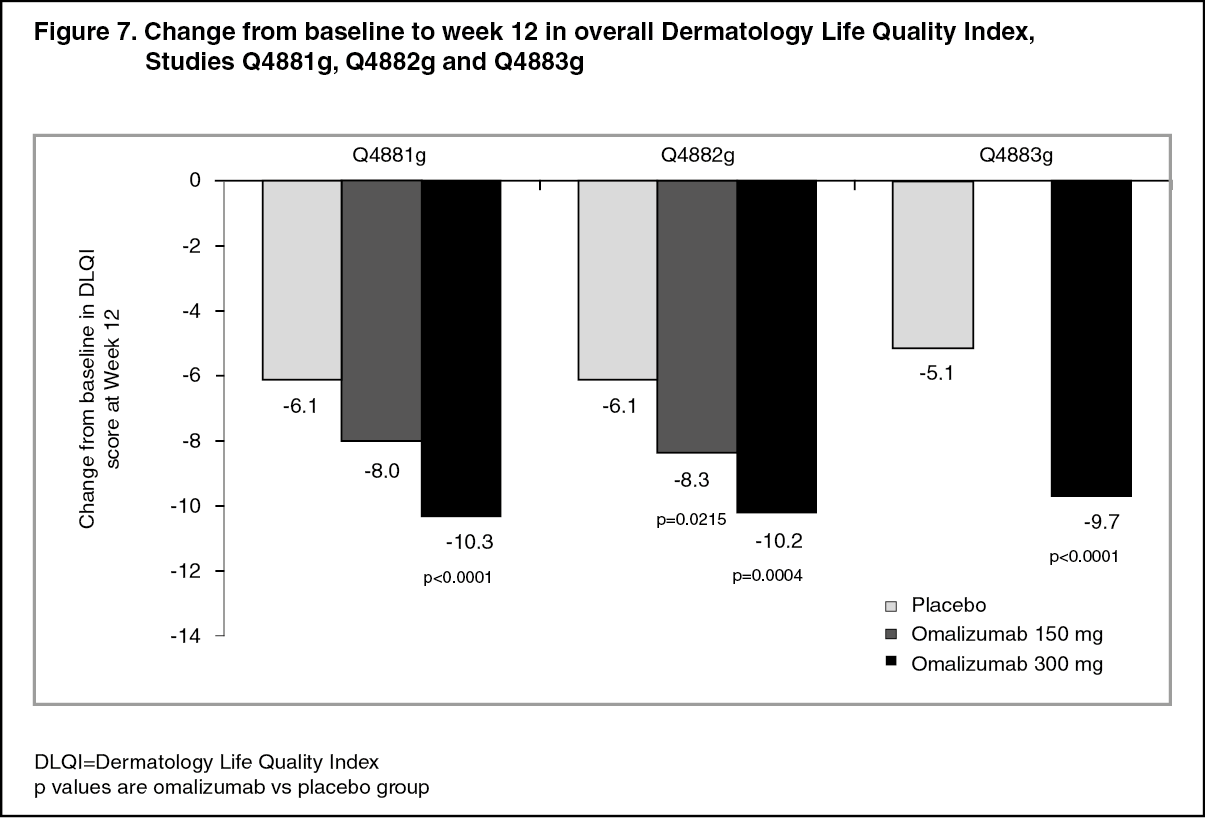 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image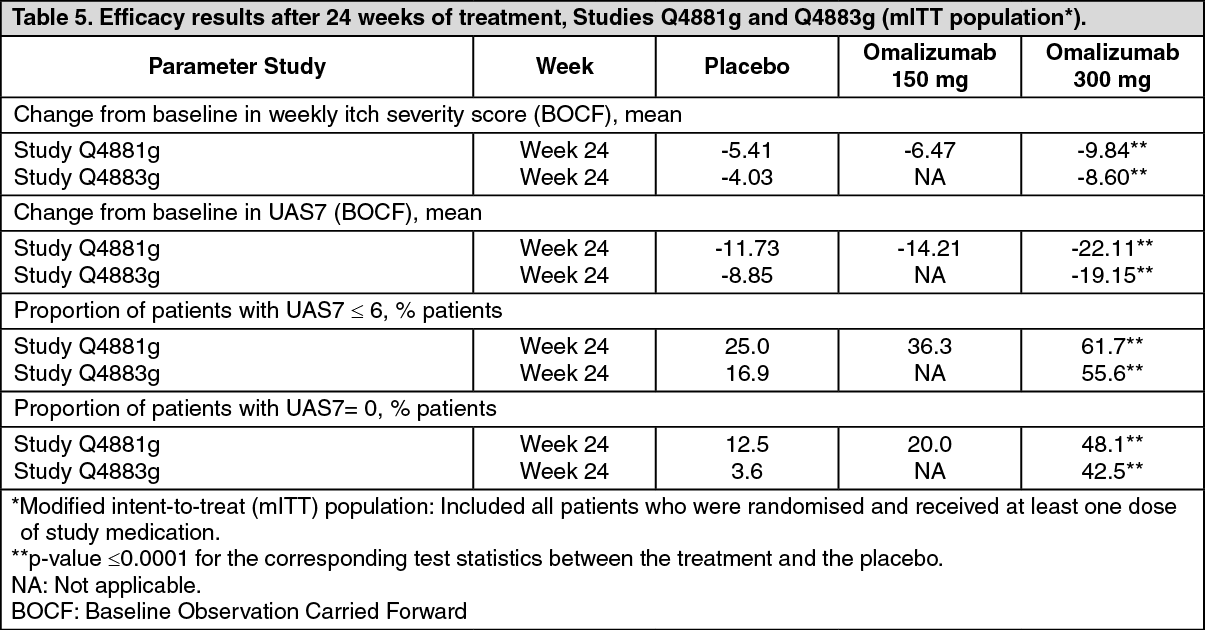 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image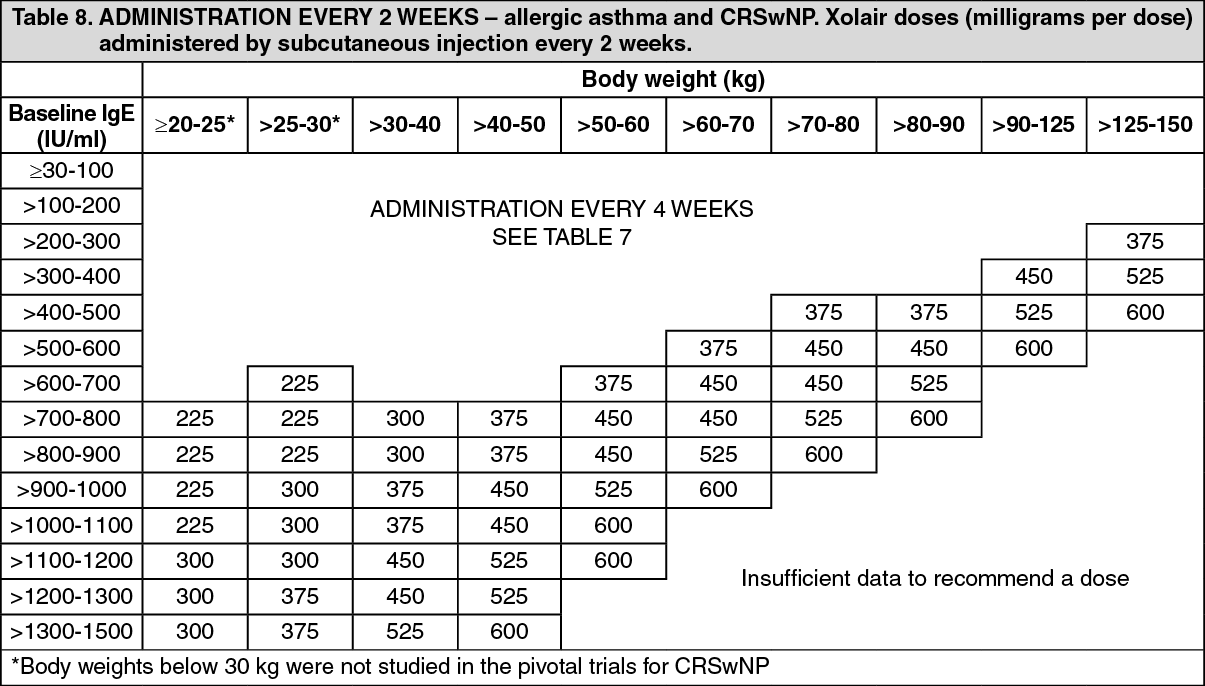 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image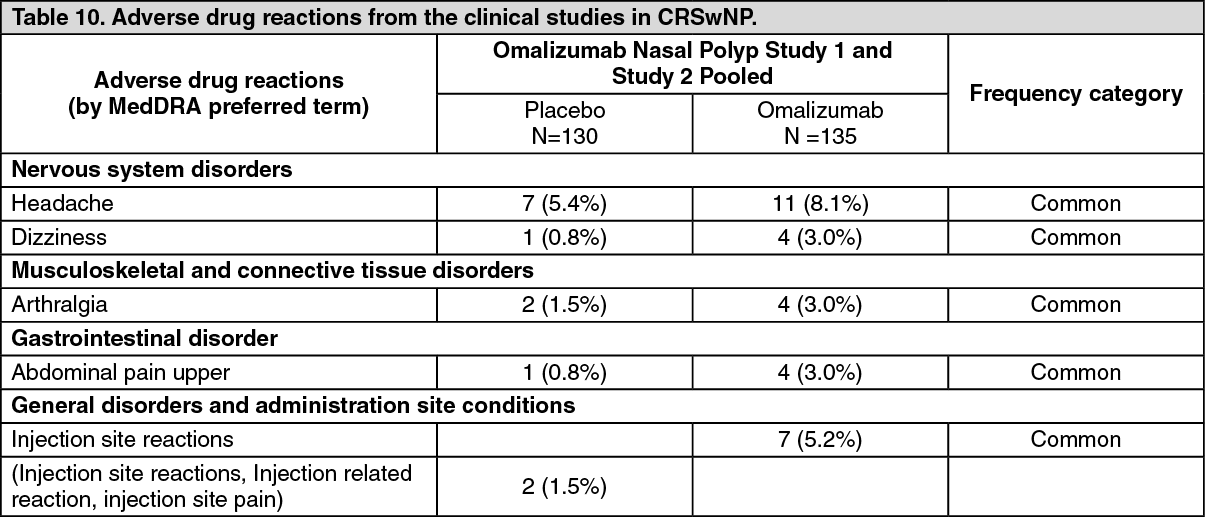 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image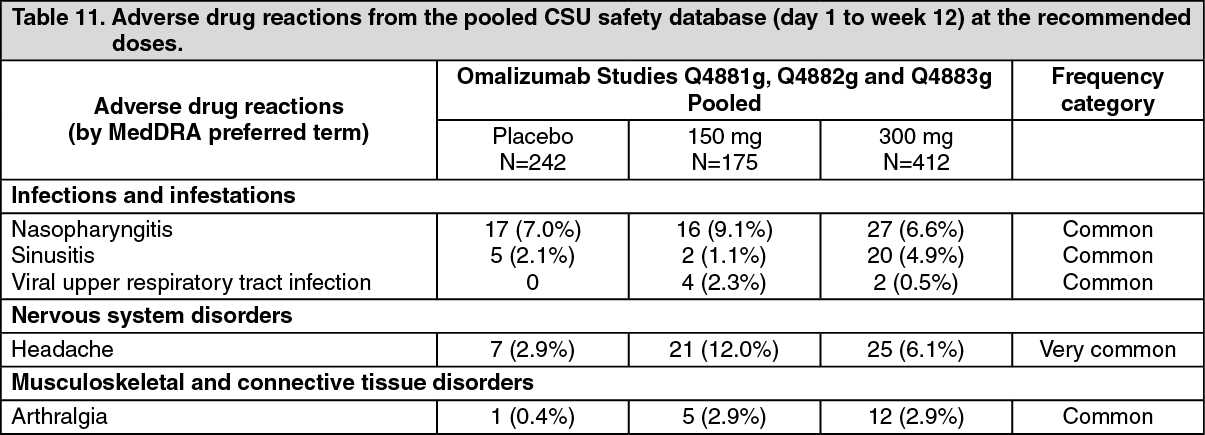 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out
