


 Sign Out
Sign Out

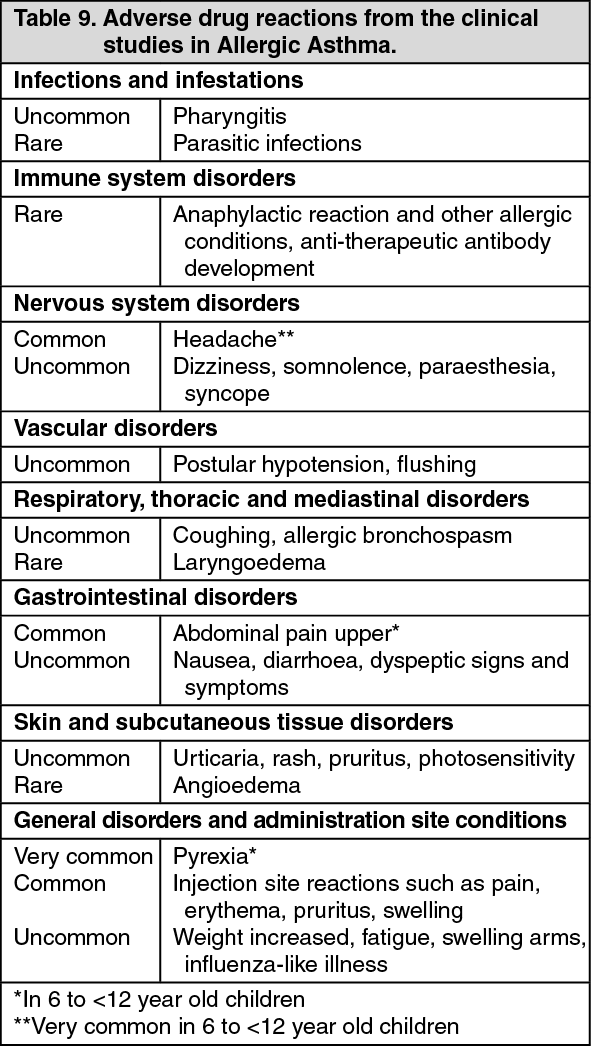
Tabulated summary of adverse drug reactions from the clinical studies: Table 9 lists the adverse drug reactions recorded in clinical studies in the total allergic asthma safety population treated with Xolair by system organ class and by frequency. Frequencies are defined as: very common (≥1/10); common (>1/100 to <1/10); uncommon (>1/1,000 to <1/100); rare (≥1/10,000 to <1/1,000); very rare (<1/10,000). (See Table 9.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageThe frequencies of adverse drug reactions in the active treatment group were very similar to those observed in the control group.
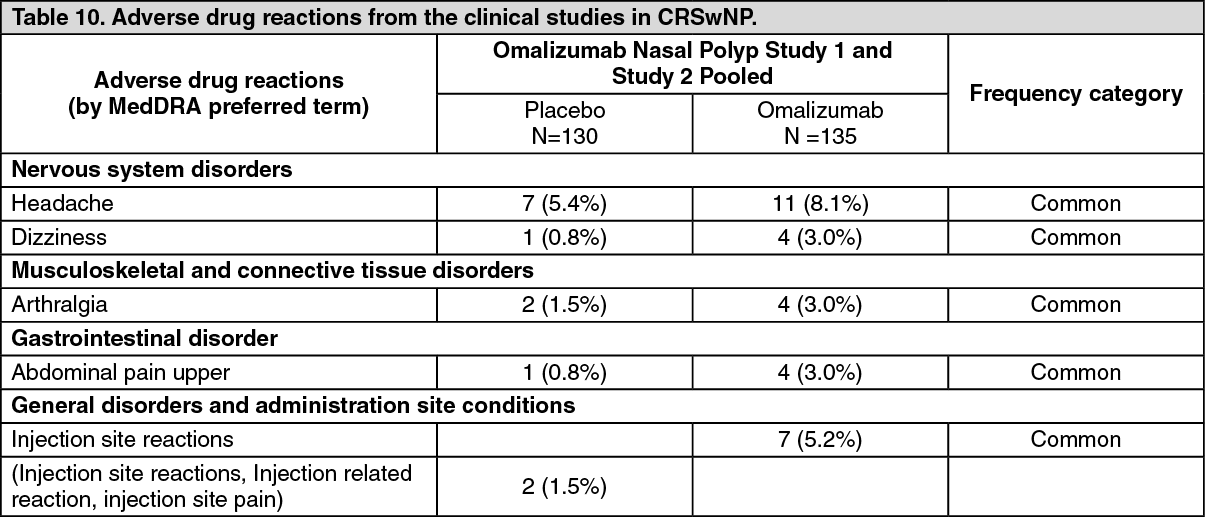
Chronic rhinosinusitis with nasal polyps (CRswNP): Summary of the safety profile: The data described as follows reflect data from two placebo-controlled studies in patients ≥18 years of age. In these studies, patients received either Xolair 150 to 600 mg every 2 or 4 weeks or placebo. All patients received background intranasal mometasone therapy. The safety profile in patients with CRSwNP was consistent with that in allergic asthma and CSU. The most frequently (>3%) reported adverse drug reactions, which were higher in frequency in comparison to placebo are shown in Table 10.
Tabulated summary of adverse drug reactions from the clinical studies: Table 10 lists the adverse drug reactions recorded in clinical studies in the total nasal polyp safety population treated with Xolair by system organ class and by frequency. Frequencies are defined as: very common (≥1/10); common (≥1/100 to <1/10); uncommon (≥1/1,000 to <1/100); rare (≥1/10,000 to <1/1,000); very rare (<1/10,000). (See Table 10.)
 Click on icon to see table/diagram/image
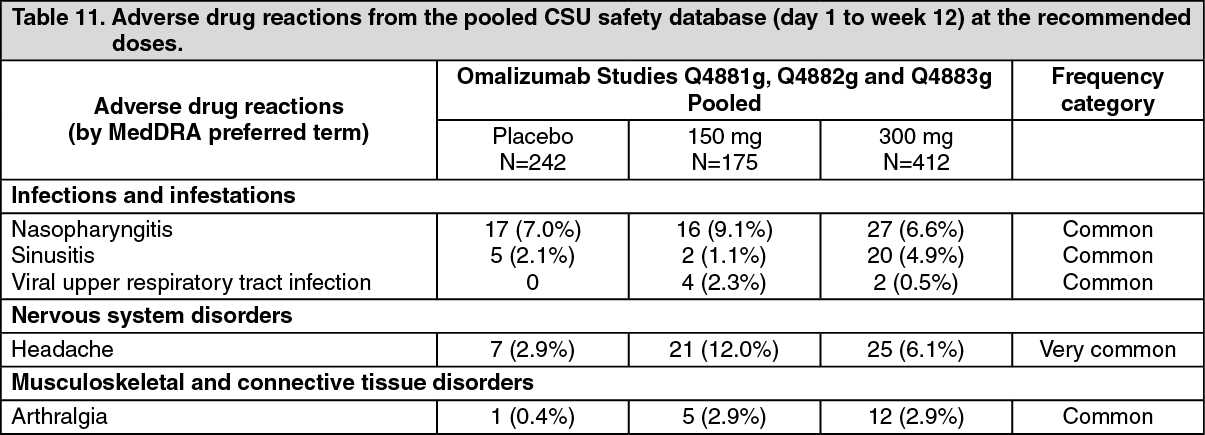
Click on icon to see table/diagram/imageChronic Spontaneous Urticaria (CSU): Summary of the safety profile: The safety and tolerability of omalizumab were investigated with the doses of 75 mg, 150 mg and 300 mg every four weeks in 975 CSU patients, 242 of whom received placebo. 733 patients were treated with omalizumab for up to 12 weeks and 490 patients for up to 24 weeks. 175 and 412 patients were treated for up to 12 weeks and 87 and 333 patients were treated for up to 24 weeks at the recommended doses of 150 mg and 300 mg respectively.
During clinical studies with adult and adolescent patients (12 years of age and older) the most commonly reported adverse drug reactions observed were headache and nasopharyngitis.
Tabulated summary of adverse drug reactions from the clinical studies at the recommended doses (150 mg and 300 mg): Adverse drug reactions (events occurring in ≥1% of patients in any treatment group and ≥2% more frequently in any omalizumab treatment group than in the placebo group after medical review) reported at the recommended doses (150 mg and 300 mg) in the three pooled Phase III studies are listed by MedDRA system organ class (Table 11). Within each system organ class, the adverse drug reactions are ranked by frequency, with the most frequent reactions listed first. The corresponding frequency category for each adverse reaction is based on the following convention (CIOMS III): very common (≥1/10); common (≥1/100 to <1/10); uncommon (≥1/1,000 to <1/100); rare (≥1/10,000 to <1/1000); very rare (<1/10,000). (See Table 11.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageAdditional events reported anytime during the day 1 to week 24 treatment period (studies Q4881g and Q4883g) that met the criteria of adverse drug reactions: Infections and infestations: upper respiratory tract infections (placebo 3.1%, 150 mg 3.4%, 300 mg 5.7%), urinary tract infection (placebo 1.8%, 150 mg 4.6%, 300 mg 2.4%).
Nervous system disorders: sinus headache (placebo 0%, 150 mg 2.3%, 300 mg 0.3%).
Musculoskeletal and connective tissue disorders: myalgia (placebo 0%, 150 mg 2.3%, 300 mg 0.9%), pain in extremity (placebo 0%, 150 mg 3.4%, 300 mg 0.9%), musculoskeletal pain (placebo 0%, 150 mg 2.3%, 300 mg 0.9%).
General disorders and administration site conditions: pyrexia (placebo 1.2%, 150 mg 3.4%, 300 mg 0.9%).
Injection site reactions: injection site reactions occurred during the studies in more omalizumab-treated patients than placebo patients (2.7% at 300 mg, 0.6% at 150 mg, 0.8% with placebo). They included: swelling, erythema, pain, bruising, itching, bleeding and urticaria.
Adverse drug reactions from spontaneous reports (frequency not known): The following adverse drug reactions have been identified from post-marketing experience with Xolair via spontaneous reporting. Because these reactions are reported voluntarily from a population of uncertain size, it is not possible to reliably estimate their frequency which is therefore categorized as not known. Adverse drug reactions are listed according to system organ classes in MedDRA. Within each system organ class, ADRs are presented in order of decreasing seriousness: Immune system disorders (see PRECAUTIONS): Anaphylaxis and anaphylactoid reactions have been reported following the first or subsequent administrations; serum sickness.
Skin and subcutaneous tissue disorders: Alopecia.
Blood and lymphatic system disorders: Idiopathic severe thrombocytopenia.
Respiratory, thoracic and mediastinal disorders: Churg Strauss syndrome (i.e., Eosinophilic Granulomatosis with Polyangiitis).
Musculoskeletal and connective tissue disorders: Arthralgia, myalgia, joint swelling.
Description of adverse drug reactions of special interest: Anaphylaxis: In post-marketing reports, the frequency of anaphylaxis in patients exposed to Xolair use was estimated to be 0.2% based on a total number of anaphylactic reactions observed from an estimated exposure of over 500,000 patient years.
Thrombocytopenia: In clinical trials few patients experienced platelet counts below the lower limit of the normal laboratory range. None of these changes were associated with bleeding episodes or a decrease in hemoglobin. No pattern of persistent decrease in platelet counts has been reported in humans (patients greater than 6 years of age), as was observed in non-human primates (see Pharmacology: Toxicology: NON-CLINICAL SAFETY DATA under Actions). Thrombocytopenia has been reported in post-marketing experience.
Parasitic infections: In allergic asthma patients at chronic high risk of helminth infection, a placebo-controlled trial showed a slight numerical increase in infection rate with omalizumab that was not statistically significant. The course, severity, and response to treatment of infections were unaltered (see PRECAUTIONS).
Description of select adverse events: The following adverse events have been reported in patients treated with Xolair, however, the causality of the adverse events and Xolair use has not been established.
Malignancies: During initial clinical trials in adults and adolescents 12 years of age and older, there was a numerical imbalance in cancers arising in the active treatment group, compared with the control group. The number of observed cases was uncommon (<1/100) in both the active and the control group. In a subsequent observational study comparing 5,007 Xolair-treated and 2,829 non-Xolair-treated patients followed for up to 5 years, the incidence rates of primary malignancies per 1,000 patient years were 16.01 (295/18,426 patient years) and 19.07 (190/9,963 patients years), respectively, which does not indicate an increased malignancy risk (rate ratio 0.84, 95% confidence interval, 0.62 to 1.13). In a further analysis of randomized, double-blind, placebo-controlled clinical trials including 4,254 patients on Xolair and 3,178 patients on placebo, Xolair treatment was not associated with an increased malignancy risk based on incidence rates per 1,000 patient years of 4.14 (14/3,382 patient years) for Xolair-treated patients and 4.45 (11/2,474 patient years) for placebo patients (rate ratio 0.93, 95% confidence interval 0.39 to 2.27). The overall observed incidence rate of malignancy in the Xolair clinical trial program was comparable to that reported in the general population.
There were no cases of malignancy in clinical trials in the 6 to <12 years of age group with omalizumab; there was a single case of malignancy in the control group.
Arterial Thromboembolic Events (ATE): In controlled clinical trials and during interim analyses of an observational study, a numerical imbalance of ATEs was observed. ATE included stroke, transient ischemic attack, myocardial infarction, unstable angina, and cardiovascular death (including death from unknown cause). In the final analysis of the observational study, the rate of ATE per 1,000 patient years was 7.52 (115/15,286 patients years) for Xolair-treated patients and 5.12 (51/9,963 patient years) for control patients. In a multivariate analysis controlling for available baseline cardiovascular risk factors, the hazard ratio was 1.32 (95% confidence interval 0.91 to 1.91). In a separate analysis of pooled clinical trials including all randomized double-blind, placebo-controlled clinical trials of 8 or more weeks duration, the rate of ATE per 1,000 patient years was 2.69 (5/1,856 patients years) for Xolair-treated patients and 2.38 (4/1,680 patient years) for placebo patients (rate ratio 1.13, 95% confidence interval 0.24 to 5.71).
View ADR Monitoring Form