


 Sign Out
Sign Out




Duration of Treatment: The duration of treatment depends on the type of major orthopaedic surgery.
Hip Replacement Surgery: 5 weeks is recommended.
Knee Replacement Surgery: 2 weeks is recommended.
Dose of 10 mg once daily and duration specified for each type of surgery is not to be exceeded.
Missed Dose: If a dose is missed, the patient should take the Xarelto 10-mg dose immediately and continue on the following day with the once daily intake as before.
Xarelto 15 and 20 mg: Posology: Prevention of stroke and systemic embolism: The recommended dose is 20 mg once daily, which is also the recommended maximum dose.
Therapy with Xarelto should be continued long-term provided the benefit of prevention of stroke and systemic embolism outweighs the risk of bleeding (see Precautions).
If a dose is missed, the patient should take Xarelto immediately and continue on the following day with the once daily intake as recommended. The dose should not be doubled within the same day to make up for a missed dose.
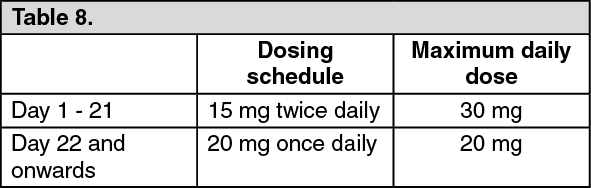
Treatment of DVT, treatment of PE and prevention of recurrent DVT and PE: The recommended dose for the initial treatment of acute DVT or PE is 15 mg twice daily for the first three weeks followed by 20 mg once daily for the continued treatment and prevention of recurrent DVT and PE, as indicated in the table as follows. (See Table 8.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageThe duration of therapy should be individualised after careful assessment of the treatment benefit against the risk for bleeding (see Precautions). Short duration of therapy (at least 3 months) should be based on transient risk factors (e.g. recent surgery, trauma, immobilisation) and longer durations should be based on permanent risk factors or idiopathic DVT or PE.
If a dose is missed during the 15 mg twice daily treatment phase (day 1 - 21), the patient should take Xarelto immediately to ensure intake of 30 mg Xarelto per day. In this case, two 15 mg tablets may be taken at once. The patient should continue with the regular 15 mg twice daily intake as recommended on the following day.
If a dose is missed during the once daily treatment phase (day 22 and onwards), the patient should take Xarelto immediately, and continue on the following day with the once daily intake as recommended. The dose should not be doubled within the same day to make up for a missed dose.
Converting from Vitamin K Antagonists (VKA) to Xarelto: When converting patients from VKAs to Xarelto, INR values will be falsely elevated after the intake of Xarelto. The INR is not valid to measure the anticoagulant activity of Xarelto and therefore should not be used (see Interactions).
Xarelto 15 and 20 mg: For patients treated for prevention of stroke and systemic embolism, VKA treatment should be stopped and Xarelto therapy should be initiated when the International Normalized Ratio (INR) is ≤ 3.0.
For patients treated for DVT, PE and prevention of recurrence, VKA treatment should be stopped and Xarelto therapy should be initiated once the INR is ≤ 2.5.
Converting from Xarelto to Vitamin K antagonists (VKA): There is a potential for inadequate anticoagulation during the transition from Xarelto to VKA. Continuous adequate anticoagulation should be ensured during any transition to an alternate anticoagulant. It should be noted that Xarelto can contribute to an elevated INR.
In patients converting from Xarelto to VKA, VKA should be given concurrently until the INR is ≥ 2.0. For the first two days of the conversion period, standard initial dosing of VKA should be used followed by VKA dosing, as guided by INR testing. While patients are on both Xarelto and VKA, the INR should not be tested earlier than 24 hours after the previous dose but prior to the next dose of Xarelto. Once Xarelto is discontinued INR testing may be done reliably at least 24 hours after the last dose (see Interactions and Pharmacology: Pharmacokinetics under Actions).
Converting from parenteral anticoagulants to Xarelto: For patients currently receiving a parenteral anticoagulant, discontinue the parenteral anticoagulant and start Xarelto 0 to 2 hours before the time that the next scheduled administration of the parenteral medicinal product (e.g. low molecular weight heparins) would be due or at the time of discontinuation of a continuously administered parenteral medicinal product (e.g. intravenous unfractionated heparin).
Converting from Xarelto to parenteral anticoagulants: Xarelto 10 mg: Discontinue Xarelto and give the 1st dose of parenteral anticoagulant at the time that the next Xarelto dose would be taken.
Xarelto 15 and 20 mg: Give the first dose of parenteral anticoagulant at the time the next Xarelto dose would be taken.
Special populations: Renal impairment: Xarelto 10 mg: No dose adjustment is required if Xarelto is administered in patients with mild (CrCl ≤80-50 mL/min) or moderate (CrCl: <50-30 mL/min) renal impairment (see Pharmacology: Pharmacokinetics under Actions).
Limited clinical data for patients with severe renal impairment (CrCl <30-15 mL/min) indicate that rivaroxaban plasma levels are significantly increased in this patient population. Therefore, Xarelto must be used with caution in these patients (see Pharmacology: Pharmacokinetics under Actions and Precautions)
Use of Xarelto is not recommended in patients with CrCl <15 mL/min. (see Pharmacology: Pharmacokinetics under Actions and Precautions).
Xarelto 15 and 20 mg: Limited clinical data for patients with severe renal impairment (creatinine clearance 15 - 29 ml/min) indicate that rivaroxaban plasma concentrations are significantly increased. Therefore, Xarelto is to be used with caution in these patients. Use is not recommended in patients with creatinine clearance < 15 ml/min (see Precautions and Pharmacology: Pharmacokinetics under Actions).
In patients with moderate (creatinine clearance 30 - 49 ml/min) or severe (creatinine clearance 15 - 29 ml/min) renal impairment, the following dosage recommendations apply: For the prevention of stroke and systemic embolism in patients with non-valvular atrial fibrillation, the recommended dose is 15 mg once daily (see Pharmacology: Pharmacokinetics under Actions).
For the treatment of DVT, treatment of PE and prevention of recurrent DVT and PE: Patients should be treated with 15 mg twice daily for the first 3 weeks. Thereafter, the recommended dose is 20 mg once daily. A reduction of the dose from 20 mg once daily to 15 mg once daily should be considered if the patient's assessed risk for bleeding outweighs the risk for recurrent DVT and PE. The recommendation for the use of 15 mg is based on PK modelling and has not been studied in this clinical setting (see Precautions, Pharmacology: Pharmacodynamics and Pharmacokinetics under Actions).
No dose adjustment is necessary in patients with mild renal impairment (creatinine clearance 50 - 80 ml/min) (see Pharmacology: Pharmacokinetics under Actions).
Hepatic Impairment: Xarelto 10 mg: Xarelto 10 mg is contraindicated in patients with hepatic disease which is associated with coagulopathy leading to a clinically relevant bleeding risk (see Contraindications).
No dose adjustment is necessary in patients with other hepatic diseases (see Pharmacology: Pharmacokinetics under Actions).
Limited clinical data in patients with moderate hepatic impairment (Child-Pugh B) indicate a significant increase in the pharmacological activity. No clinical data are available for patients with severe hepatic impairment (Child-Pugh C) (see Pharmacology: Pharmacokinetics under Actions and Contraindications).
Xarelto 15 and 20 mg: Xarelto is contraindicated in patients with hepatic disease associated with coagulopathy and clinically relevant bleeding risk including cirrhotic patients with Child Pugh B and C (see Contraindications and Pharmacology: Pharmacokinetics under Actions).
Elderly population: No dose adjustment (see Pharmacology: Pharmacokinetics under Actions).
Body Weight: No dose adjustment (see Pharmacology: Pharmacokinetics under Actions).
Gender: No dose adjustment (see Pharmacology: Pharmacokinetics under Actions).
Paediatric population: The safety and efficacy of Xarelto in children aged 0 to 18 years have not been established. No data are available. Therefore, Xarelto is not recommended for use in children below 18 years of age.
Patients undergoing cardioversion: Xarelto can be initiated or continued in patients who may require cardioversion.
For transesophageal echocardiogram (TEE) guided cardioversion in patients not previously treated with anticoagulants, Xarelto treatment should be started at least 4 hours before cardioversion to ensure adequate anticoagulation (see Pharmacology: Pharmacodynamics and Pharmacokinetics under Actions). For all patients, confirmation should be sought prior to cardioversion that the patient has taken Xarelto as prescribed. Decisions on initiation and duration of treatment should take established guideline recommendations for anticoagulant treatment in patients undergoing cardioversion into account.
Patients with non-valvular atrial fibrillation who undergo PCI (percutaneous coronary intervention) with stent placement: There is limited experience of a reduced dose of 15 mg Xarelto once daily (or 10 mg Xarelto once daily for patients with moderate renal impairment [creatinine clearance 30 - 49 ml/min]) in addition to a P2Y12 inhibitor for a maximum of 12 months in patients with non-valvular atrial fibrillation who require oral anticoagulation and undergo PCI with stent placement (see Precautions and Pharmacology: Pharmacodynamics under Actions).
Method of administration: For oral use.
Xarelto 10 mg: One (1) 10-mg tablet of Xarelto should be taken once daily.
Xarelto 10 mg tablets may be taken with or without food.
The initial dose should be taken within 6-10 hrs after surgery provided that hemostasis has been established.
For patients who are unable to swallow whole tablets, Xarelto tablet may be crushed and mixed with water or apple puree immediately prior to use, and administered orally.
The crushed Xarelto tablet may also be given through gastric tubes after confirmation of the correct gastric placement of the tube. The crushed tablet should be administered in a small amount of water via a gastric tube after which it should be flushed with water (see Pharmacology: Pharmacokinetics under Actions).
Xarelto 15 and 20 mg: The tablets are to be taken with food (see Pharmacology: Pharmacokinetics under Actions).
For patients who are unable to swallow whole tablets, Xarelto tablet may be crushed and mixed with water or apple puree immediately prior to use, and administered orally. After the administration of crushed Xarelto 15 mg or 20 mg film-coated tablets, the dose should be immediately followed by food.
The crushed Xarelto tablet may also be given through gastric tubes after confirmation of the correct gastric placement of the tube. The crushed tablet should be administered in a small amount of water via a gastric tube after which it should be flushed with water. After the administration of crushed Xarelto 15 mg or 20 mg film-coated tablets, the dose should then be immediately followed by enteral feeding (Pharmacology: Pharmacokinetics under Actions).