


 Sign Out
Sign Out




Xarelto 10 mg: The safety of Xarelto has been evaluated in 4 phase III studies including 6097 patients exposed to Xarelto 10 mg undergoing major orthopedic surgery of the lower limbs (total hip or knee replacement) in 3997 hospitalized medically ill patients treated up to 39 days, and in three phase III VTE treatment trials with 4556 patients exposed either to Xarelto 15 mg twice daily for 3 weeks followed by 20 mg once daily or to 20 mg once daily treated up to 21 months.
Furthermore, safety of Xarelto has been also evaluated in 7750 patients with non-valvular atrial fibrillation from 2 phase III trials with at least 1 dose of Xarelto as well as in 10,225 ACS patients with at least 1 dose of either Xarelto 2.5mg (twice daily) or Xarelto 5 mg (twice daily) on top of either ASA or ASA plus clopidogrel or ticlopidine.
Due to the pharmacological mode of action, Xarelto may be associated with an increased risk of occult or overt bleeding from any tissue and organ which may result in post hemorrhagic anemia. The risk of bleedings may be increased in certain patient groups eg, patients with uncontrolled severe arterial hypertension and/or on concomitant medication affecting haemostasis (see Precautions). The signs, symptoms, and severity (including fatal outcome) will vary according to the location and degree or extent of the bleeding and/or anemia (see Overdosage).
Hemorrhagic complications may present as weakness, paleness, dizziness, headache or unexplained swelling, dyspnea and unexplained shock. In some cases as a consequence of anemia, symptoms of cardiac ischemia like chest pain or angina pectoris have been observed.
Known complications secondary to severe bleeding eg, compartment syndrome and renal failure due to hypoperfusion have been reported for Xarelto. Therefore, the possibility of a hemorrhage should be considered in evaluating the condition in any anticoagulated patient.
Xarelto 15 and 20 mg: The safety of rivaroxaban has been evaluated in eleven phase III studies including 32,625 patients exposed to rivaroxaban (see Table 9).
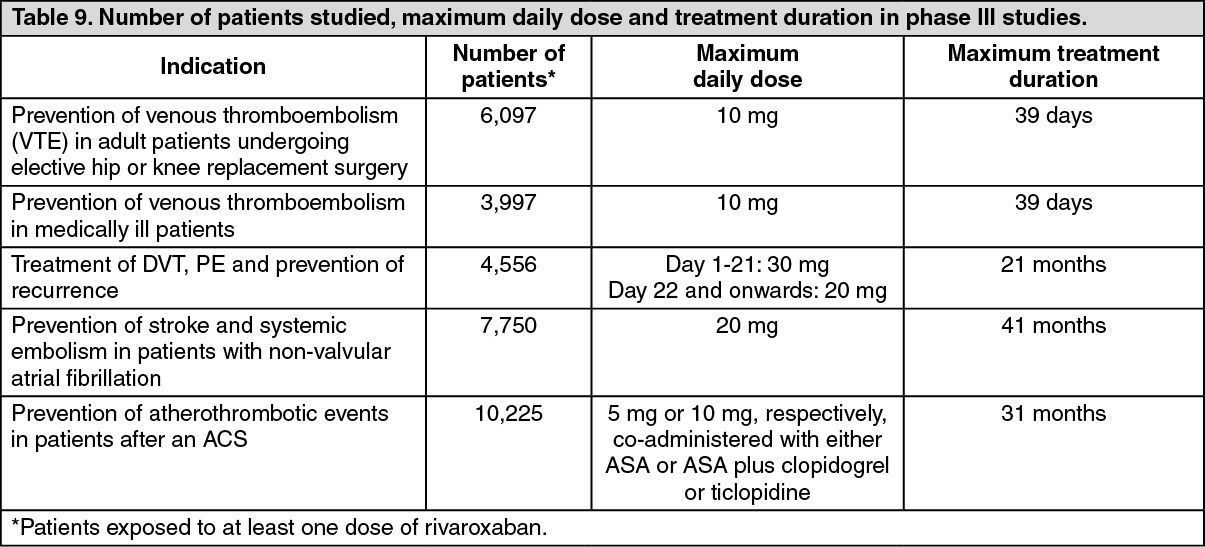 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageThe most commonly reported adverse reactions in patients receiving rivaroxaban were bleedings (see Precautions and Description of selected adverse reactions as follows). The most commonly reported bleedings (≥4%) were epistaxis (5.9%) and gastrointestinal tract haemorrhage (4.2%).
Tabulated list of Adverse Reactions: Xarelto 10 mg: The frequencies of adverse drug reactions (ADRs) reported with Xarelto are summarized in Table 8 as follows. Within each frequency grouping, undesirable effects are presented in order of decreasing seriousness. Frequencies are defined as: Very common (≥1/10), common (≥1/100 to <1/10), uncommon (≥1/1000 to <1/100), rare (≥1/10,000 to <1/1000). (See Table 10.)
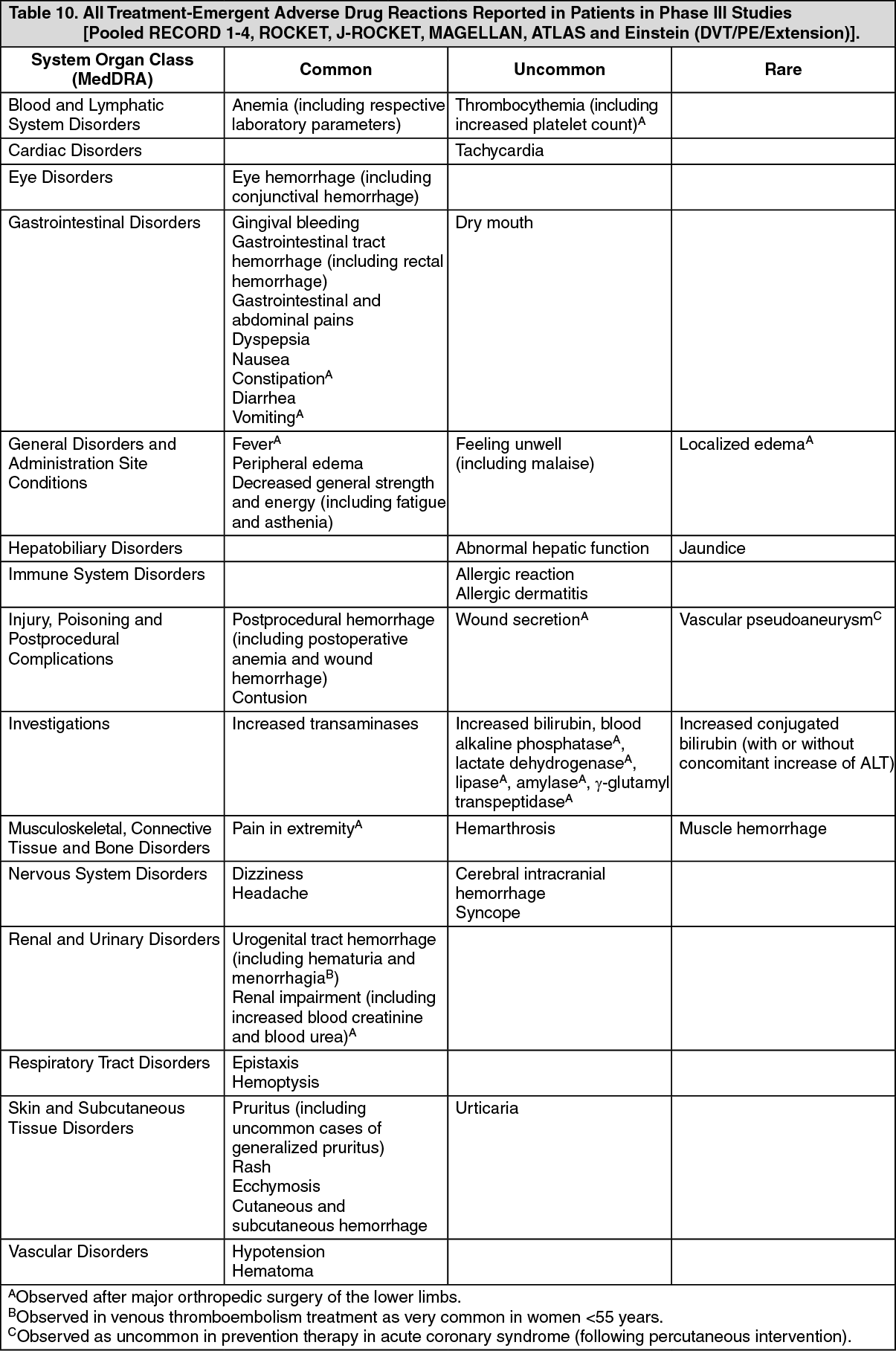 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageXarelto 15 and 20 mg: The frequencies of adverse reactions reported with Xarelto are summarised in Table 10 as follows by system organ class (in MedDRA) and by frequency. Frequencies are defined as: Very common (≥1/10), common (≥1/100 to <1/10), uncommon (≥1/1,000 to <1/100), rare (≥1/10,000 to <1/1,000), very rare (<1/10,000), Not known (cannot be estimated from the available data). (See Table 11.)
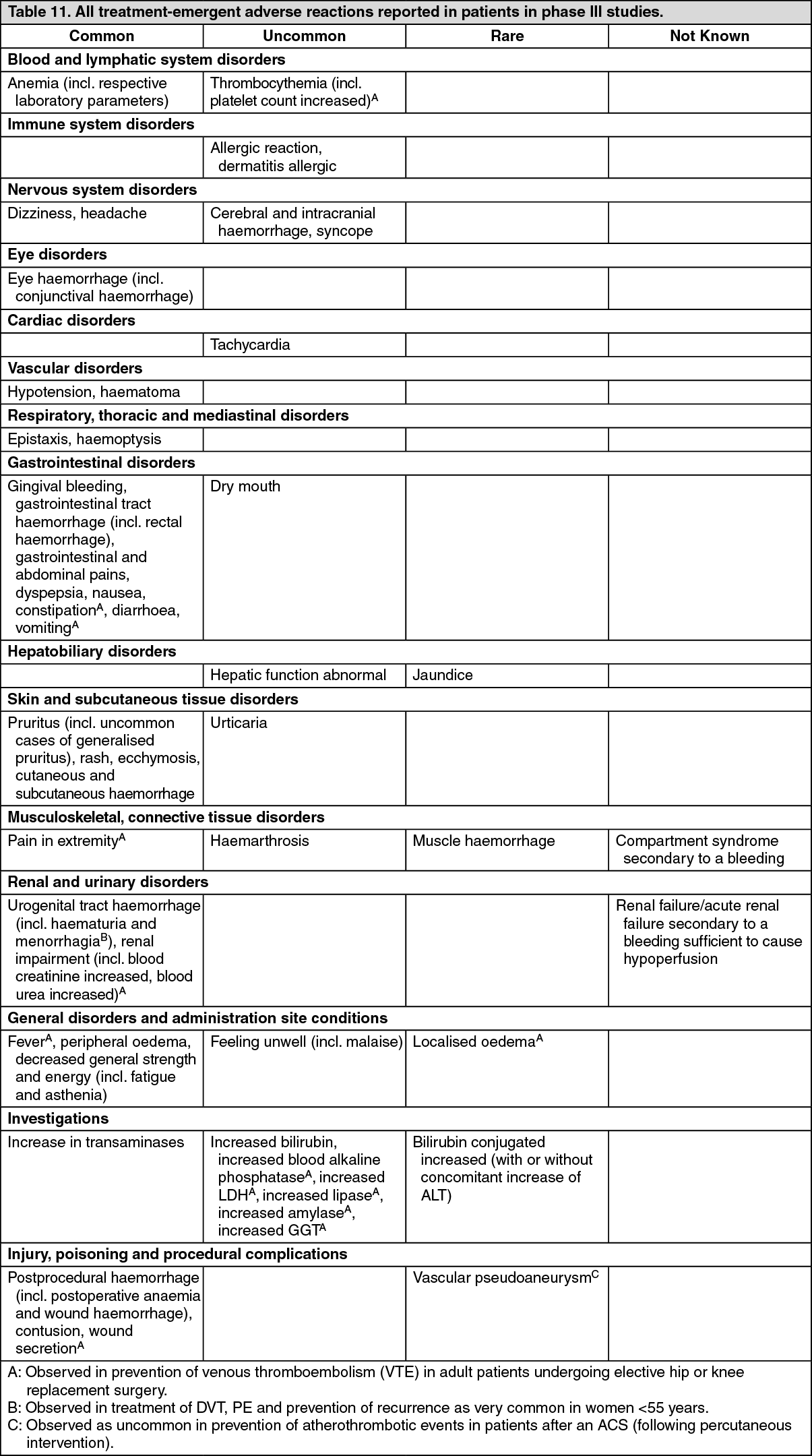 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageDescription of selected adverse reactions: Xarelto 15 and 20 mg: Due to the pharmacological mode of action, the use of Xarelto may be associated with an increased risk of occult or overt bleeding from any tissue or organ which may result in post haemorrhagic anaemia. The signs, symptoms and severity (including fatal outcome) will vary according to the location and degree or extent of the bleeding and/or anaemia (see Management of Bleeding under Overdosage). In the clinical studies, mucosal bleedings (i.e. epistaxis, gingival, gastrointestinal and genitourinary) and anemia were seen more frequently during long-term rivaroxaban treatment compared with VKA treatment. Thus, in addition to adequate clinical surveillance, laboratory testing of haemoglobin/haematocrit could be of value to detect occult bleeding, as judged to be appropriate. The risk of bleedings may be increased in certain patient groups e.g. those patients with uncontrolled severe arterial hypertension and/or on concomitant treatment affecting haemostasis (see Haemorrhagic risk under Precautions). Menstrual bleeding may be intensified and/or prolonged. Haemorrhagic complications may present as weakness, paleness, dizziness, headache or unexplained swelling, dyspnoea and unexplained shock. In some cases, as a consequence of anaemia, symptoms of cardiac ischaemia like chest pain or angina pectoris have been observed.
Known complications secondary to severe bleeding such as compartment syndrome and renal failure due to hypoperfusion have been reported for Xarelto. Therefore, the possibility of haemorrhage is to be considered in evaluating the condition in any anticoagulated patient.
Post-marketing observations: Xarelto 15 and 20 mg: The following adverse reactions have been reported post-marketing in temporal association with the use of Xarelto. The frequency of these adverse reactions reported from post-marketing experience cannot be estimated.
Immune system disorders: Angioedema and allergic oedema (In the pooled phase III trials, these events were uncommon (≥1/1,000 to <1/100)).
Hepatobiliary disorders: Cholestasis, Hepatitis (incl. hepatocellular injury) (In the pooled phase III trials, these events were rare (≥1/10,000 to <1/1,000)).
Blood and lymphatic system disorders: Thrombocytopenia (In the pooled phase III trials, these events were uncommon (≥1/1,000 to <1/100)).
Skin and subcutaneous tissue disorders: Stevens-Johnson syndrome/Toxic Epidermal Necrolysis (In the pooled phase III trials, these events were estimated as very rare (<1/10,000)).
View ADR Monitoring Form