


 Sign Out
Sign Out




Powder for solution for infusion: Voriconazole requires reconstitution and dilution (see Special precautions for disposal and other handling under Cautions for Usage) prior to administration as an intravenous infusion.
Voriconazole powder for solution for infusion is not recommended for bolus injection.
It is recommended that voriconazole be administered at a maximum rate of 3 mg/kg per hour over 1 to 3 hours.
Blood products and concentrated electrolytes: Voriconazole must not be infused concomitantly with any blood product or any short-term infusion of concentrated electrolytes, even if the two infusions are running in separate intravenous lines (or cannulas). Electrolyte disturbances such as hypokalemia, hypomagnesemia and hypocalcemia should be corrected prior to initiation of voriconazole therapy (see Precautions).
Intravenous solutions containing (non-concentrated) electrolytes: Voriconazole can be infused at the same time as other intravenous solutions containing (non-concentrated) electrolytes, but must be infused through a separate line.
Total parenteral nutrition (TPN): Voriconazole can be infused at the same time as total parenteral nutrition, but must be infused in a separate line. If infused through a multiple-lumen catheter, TPN needs to be administered using a different port from the one used for voriconazole (see Incompatibilities under Cautions for Usage).
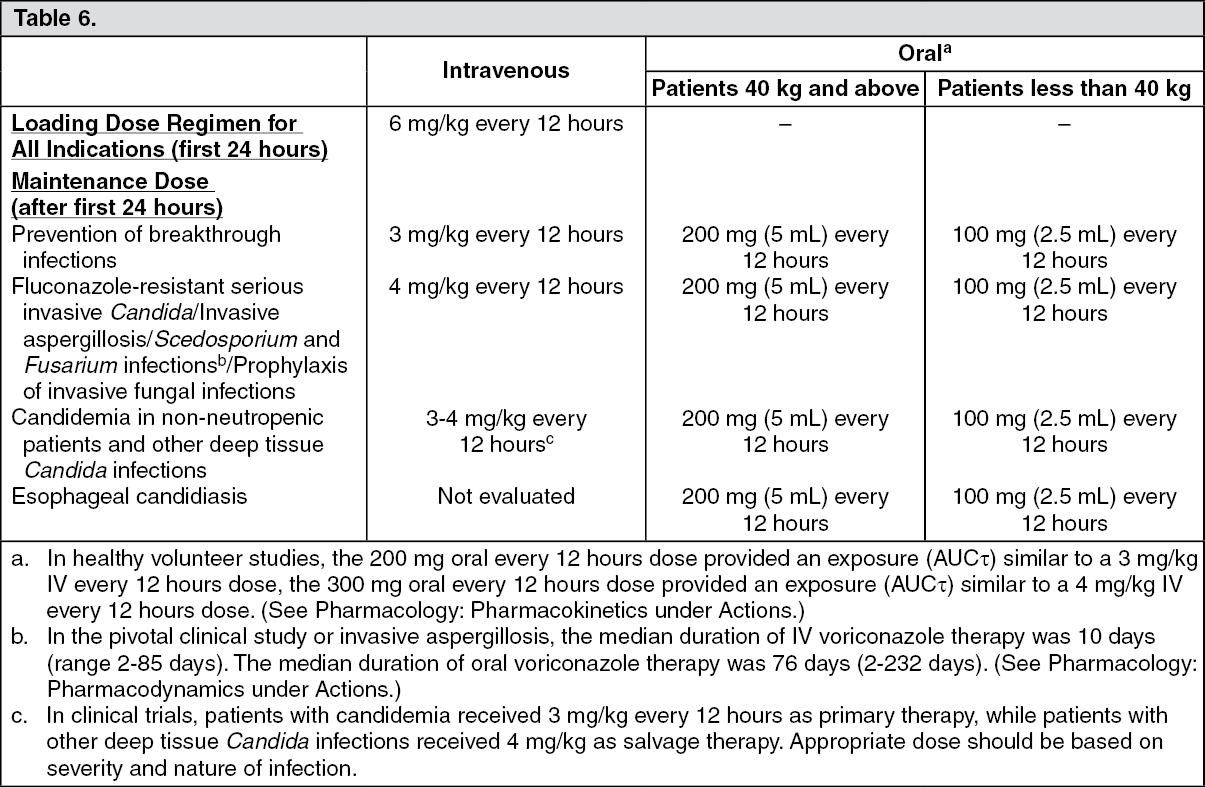
Use in adults: Therapy must be initiated with the specified intravenous loading dose regimen of voriconazole to achieve adequate plasma concentrations on Day 1. Intravenous treatment should be continued for at least 7 days before switching to oral treatment (see Pharmacology: Pharmacodynamics under Actions). Once the patient is clinically improved and can tolerate medication given by mouth, the oral tablet form or oral suspension form of voriconazole may be utilized. On the basis of the high oral bioavailability (96%), switching between intravenous and oral administration is appropriate when clinically indicated (see Pharmacology: Pharmacokinetics under Actions).
Detailed information on dosage recommendations is provided in the following table: (See Table 6).
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageDosage adjustment: Oral administration: If patient response is inadequate, the maintenance dose may be increased from 200 mg every 12 hours (similar to 3 mg/kg IV every 12 hours) to 300 mg every 12 hours (similar to 4 mg/kg IV every 12 hours) for oral administration. For patients less than 40 kg the oral dose may be increased from 100 mg to 150 mg every 12 hours.
If patients are unable to tolerate treatment at these higher doses (i.e. 300 mg oral every 12 hours), reduce the oral maintenance dose by 50 mg steps to a minimum of 200 mg every 12 hours (or 100 mg every 12 hours for patients less than 40 kg).
Phenytoin may be co-administered with voriconazole if the maintenance dose of voriconazole is increased from 200 mg to 400 mg orally, every 12 hours (from 100 mg to 200 mg orally, every 12 hours in patients less than 40 kg), see Precautions and Interactions.
When voriconazole is co-administered with adjusted doses of efavirenz, voriconazole maintenance dose should be increased to 400 mg every 12 hours (see Contraindications, Precautions and Interactions).
Treatment duration depends upon patients' clinical and mycological response.
Intravenous administration: If patient response at 3 mg/kg every 12 hours is inadequate, the intravenous maintenance dose may be increased to 4 mg/kg every 12 hours.
If patients are unable to tolerate 4 mg/kg every 12 hours, reduce the intravenous maintenance dose to a minimum of 3 mg/kg every 12 hours.
Phenytoin may be co-administered with voriconazole if the maintenance dose of voriconazole is increased to 5 mg/kg intravenously every 12 hours (see Precautions and Interactions).
Treatment duration depends upon patients' clinical and mycological response.
Use in the elderly: No dose adjustment is necessary for elderly patients.
Use in patients with renal impairment: Film-coated tablets: The pharmacokinetics of orally administered voriconazole are not affected by renal impairment. Therefore, no adjustment is necessary for oral dosing for patients with mild to severe renal impairment.
Powder for solution for infusion: In patients with moderate to severe renal dysfunction (creatinine clearance <50 mL/min), accumulation of the intravenous vehicle, sulphobutylether β-cyclodextrin sodium (SBECD), occurs. Oral voriconazole should be administered to these patients, unless an assessment of the risk benefit to the patient justifies the use of intravenous voriconazole. Serum creatinine levels should be closely monitored in these patients and, if increases occur, consideration should be given to changing to oral voriconazole therapy.
Voriconazole is hemodialyzed with a clearance of 121 mL/min. A four-hour hemodialysis session does not remove a sufficient amount of voriconazole to warrant dose adjustment.
The intravenous vehicle, SBECD, is hemodialyzed with a clearance of 55 mL/min.
Use in patients with hepatic impairment: No dose adjustment is necessary in patients with acute hepatic injury, manifested by elevated liver function tests (ALT, AST). Continued monitoring of liver function tests for further elevations is recommended.
It is recommended that the standard loading dose regimens be used but that the maintenance dose be halved in patients with mild to moderate hepatic cirrhosis (Child-Pugh A and B) receiving voriconazole.
Voriconazole has not been studied in patients with severe chronic hepatic cirrhosis (Child-Pugh C).
Voriconazole has been associated with elevations in liver function tests and clinical signs of liver damage, such as jaundice, and must only be used in patients with severe hepatic impairment if the benefit outweighs the potential risk. Patients with severe hepatic impairment must be carefully monitored for drug toxicity.
Use in pediatrics: Use in children (2 to <12 years) and young adolescents (12 to 14 years and <50 kg): The recommended dosing regimen is as follows: (See Table 7).
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageIt is recommended to initiate the therapy with intravenous regimen, and oral regimen should be considered only after there is a significant clinical improvement. It should be noted that an 8 mg/kg intravenous dose will provide voriconazole exposure approximately 2-fold higher than a 9 mg/kg oral dose.
The oral dose recommendations for children is based on studies in which voriconazole was administered as the powder for oral suspension formulation. Bioequivalence between the powder for oral suspension and tablets has not been investigated in a pediatric population. Considering the assumed limited gastro-enteric transit time in pediatrics, the absorption of tablets may be different in pediatric compared to adult patients. It is therefore, recommended to use the oral suspension formulation in children aged 2 to <12 years.
Safety and effectiveness in pediatric patients below the age of 2 years has not been established (see Pharmacology: Pharmacodynamics under Actions). Therefore, voriconazole is not recommended for children less than 2 years of age. Use in pediatric patients aged 2 to <12 years with hepatic or renal insufficiency has not been studied (see Adverse Reactions and Pharmacology: Pharmacokinetics under Actions).
Use in all other adolescents (12 to 14 years and ≥50 kg; 15 to 16 years regardless of body weight): Voriconazole should be dosed as adults.
Dosage adjustment: If patient response is inadequate, the dose may be increased by 1 mg/kg steps (or by 50 mg steps if the maximum oral dose of 350 mg was used initially). If patients are unable to tolerate treatment, reduce the dose by 1 mg/kg steps (or by 50 mg steps if the maximum oral dose of 350 mg was used initially).
Prophylaxis in adults and children: Prophylaxis should be initiated on the day of transplant and may be administered for up to 100 days. It may only be continued up to 180 days after transplantation in case of continuing immunosuppression or graft versus host disease (GvHD) (see Pharmacology: Pharmacodynamics under Actions).
Dosage: The recommended dosing regimen for prophylaxis is the same as for treatment in the respective age groups. Refer to the treatment tables previously.
Duration of prophylaxis: The safety and efficacy of voriconazole use for longer than 180 days has not been adequately studied in clinical trials.