Each ml contains: Fentanyl Citrate USP equivalent to Fentanyl 50 mcg.
Pharmacology: Pharmacodynamics: Fentanyl is a synthetic opiate with a clinical potency of 50 to 100 times that of morphine. Its onset of action is rapid and its duration of action is short. In man, a single IV dose of 0.5-1 mg/70 kg body weight immediately produces a pronounced state of surgical analgesia, respiratory depression, bradycardia and other typical morphine-like effects. The duration of action of the peak effects is about 30 minutes. All potent morphine-like drugs produce relief from pain, ventilatory depression, emesis, constipation, physical dependence, certain vagal effects and varying degrees of sedation. Fentanyl, however, differs from morphine not only by its short duration of action but also by its lack of emetic effect and minimal hypotensive activity in animals.
Pharmacokinetics: Some pharmacokinetic parameters for fentanyl are as follows: Urinary excretion = 8%; Bound in plasma = 80%; Clearance (ml/min/kg) = 13±2; Volume of distribution (litres/kg) = 4.0±0.4; Estimates of terminal half-life range from 141 to 853 minutes.
Renal impairment: Data obtained from a study administering IV fentanyl in patients undergoing renal transplantation suggest that the clearance of fentanyl may be reduced in this patient population. If patients with renal impairment receive fentanyl, they should be observed carefully for signs of fentanyl toxicity and the dose reduced if necessary.
Obese Patients: An increase in clearance of fentanyl is observed with increased body weight. In patients with a BMI>30, clearance of fentanyl increases by approximately 10% per 10 kg increase of the fat free mass (lean body mass).
Fentanyl Citrate Injection is indicated: For use as a narcotic analgesic supplement in general or regional anaesthesia.
For administration with a neuroleptic such as droperidol as an anaesthetic premedication for the induction of anaesthesia and as an adjunct in the maintenance of general and regional anaesthesia.
For use as an anaesthetic agent with oxygen in selected high risk patients undergoing major surgery.
Route of administration: Intravenous administration either as a bolus or by infusion.
Intramuscular administration.
Fentanyl should be given only in an environment where airway can be controlled and by personnel who can control the airway.
To avoid bradycardia, it is recommended to administer a small intravenous dose of an anti-cholinergic just before anaesthetic induction.
Dosage: The dosage of Fentanyl should be individualized according to age, body weight, physical status, underlying pathological condition, use of other drugs, and type of surgery and anesthesia.
To avoid bradycardia, it is recommended to administer a small intravenous dose of an anti-cholinergic just before induction.
Use as an analgesic supplement to general anesthesia: Low dose: 2 μg/kg. Fentanyl in small doses is most useful for minor, but painful, surgery.
Moderate dose: 2-20 μg/kg. Where surgery becomes more complicated, a larger dose will be required. The duration of activity is dependent on dosage.
High dose: 20-50 μg/kg. During major surgical procedures, in which surgery is longer, and during which the stress response would be detrimental to the well-being of the patient, dosages of 20-50 μg/kg of Fentanyl with nitrous oxide/oxygen have been shown to have an attenuating effect.
When dosages in this range have been used during surgery, post-operative ventilation and observation are essential in view of the possibility of extended post-operative respiratory depression. Supplemental doses of 25-250 μg (0.5-5 ml) should be tailored to the needs of the patient and to the anticipated time until completion of the operation.
Use as an anesthetic agent: When attenuation of the response to surgical stress is especially important, doses of 50-100 μg/kg may be administered with oxygen and a muscle relaxant. This technique provides anaesthesia without necessitating the use of additional anaesthetic agents. In certain cases, doses up to 150 μg/kg may be required to produce this anaesthetic effect.
Fentanyl has been used in this fashion for open heart surgery and certain other major surgical procedures in patients for whom protection of the myocardium from excess oxygen demand is particularly indicated.
Elderly (65 years of age and older): The initial dose should be reduced in the elderly and in debilitated patients. The effect of the initial dose should be taken into account in determining supplemental doses. As with other opioids, the dose should be reduced in elderly or debilitated patients.
Pediatrics: For induction and maintenance in children aged 2-12 years, a dose of 2-3 μg/kg is recommended.
Symptoms: The manifestations of fentanyl overdosage are generally an extension of its pharmacological action. Depending on the individual sensitivity, the clinical picture is determined primarily by the degree of respiratory depression which varies from bradypnoea to apnoea.
Treatment: Hypoventilation or apnoea: O2 administration, assisted or controlled respiration.
Respiratory depression: Specific opioid antagonist. This does not preclude the use of immediate countermeasures. The respiratory depression may last longer than the effect of the antagonist; additional doses of the latter may therefore be required.
Muscular rigidity: Intravenous neuromuscular blocking agent to facilitate assisted or controlled respiration.
The patient should be carefully observed; body warmth and adequate fluid intake should be maintained. If hypotension is severe or if it persists, the possibility of hypovolaemia should be considered and, if present, it should be controlled with appropriate parenteral fluid administration.
1. Risks from Concomitant Use with Benzodiazepines: Profound sedation, respiratory depression, coma, and death may result from the concomitant use of with benzodiazepines. Observational studies have demonstrated that concomitant use of opioids and benzodiazepines increases the risk of drug-related mortality compared to use of opioids alone. Because of these risks, reserve concomitant prescribing of these drugs for use in patients for whom alternative treatment options are inadequate. If the decision is made to newly prescribe a benzodiazepine and an opioid together, prescribe the lowest effective dosages and minimum durations of concomitant use.
If the decision is made to prescribe a benzodiazepine in a patient already receiving an opioid, prescribe a lower initial dose of the benzodiazepine than indicated in the absence of an opioid, and titrate based on clinical response. If the decision is made to prescribe an opioid in a patient already taking a benzodiazepine, prescribe a lower initial dose of the opioid, and titrate based on clinical response. Follow patients closely for signs and symptoms of respiratory depression and sedation. Advise both patients and caregivers about the risks of respiratory depression and sedation when is used with benzodiazepines. Advise patients not to drive or operate heavy machinery until the effects of concomitant use of the benzodiazepine have been determined. Screen patients for risk of substance use disorders, including opioid abuse and misuse, and warn them of the risk for overdose and death associated with the use of benzodiazepines (See Interactions).
2. Serotonin Syndrome with Concomitant Use of Serotonergic Drugs: Cases of serotonin syndrome, a potentially life-threatening condition, have been reported during concurrent use of with serotonergic drugs (See Interactions). This may occur within the recommended dosage range. Serotonin syndrome symptoms may include mental-status changes (e.g. agitation, hallucinations, coma), autonomic instability (e.g. tachycardia, labile blood pressure, hyperthermia), neuromuscular aberrations (e.g. hyperreflexia, incoordination) and/or gastrointestinal symptoms (e.g. nausea, vomiting, diarrhoea) and can be fatal (See Interactions). The onset of symptoms generally occurs within several hours to a few days of concomitant use, but may occur later than that. Discontinue if serotonin syndrome is suspected.
3. Adrenal Insufficiency: Cases of adrenal insufficiency have been reported with opioid use, more often following greater than one month of use. Presentation of adrenal insufficiency may include non-specific symptoms and signs including nausea, vomiting, decreased appetite, fatigue, weakness, dizziness, and low blood pressure. If adrenal insufficiency is suspected, confirm the diagnosis with diagnostic testing as soon as possible. If adrenal insufficiency is diagnosed, treat with physiologic replacement dosing of corticosteroids. Wean the patient off of the opioid to allow adrenal function to recover and continue corticosteroid treatment until adrenal function recovers. Other opioids may be tried as some cases reported use of a different opioid without recurrence of adrenal insufficiency. The information available does not identify any particular opioids as being more likely to be associated with adrenal insufficiency.
4. Sexual Function/Reproduction: Long term use of opioids may be associated with decreased sex hormone levels and symptoms such as low libido, erectile dysfunction, or infertility.
Respiratory Depression: As with all potent opioids, profound analgesia is accompanied by marked respiratory depression, which may persist into or recur in the early postoperative period. Care should be taken after large doses or infusions of fentanyl to ensure that adequate spontaneous breathing has been established and maintained before discharging the patient from the recovery area.
Significant respiratory depression will occur following the administration of fentanyl in doses in excess of 200 micrograms. This, and the other pharmacological effects of fentanyl, can be reversed by specific opioid antagonists, but additional doses may be necessary because the respiratory depression may last longer than the duration of action of the opioid antagonist.
Resuscitation equipment and opioid antagonists should be readily available.
Hyperventilation during anaesthesia may alter the patient's response to CO2, thus affecting respiration postoperatively.
Administration in labour may cause respiratory depression in the new-born infant.
Cardiac disease: Bradycardia, and possibly cardiac arrest, can occur if the patient has received an insufficient amount of anticholinergic, or when fentanyl is combined with non-vagolytic muscle relaxants. Bradycardia can be antagonised by atropine.
Muscle rigidity: Muscular rigidity (morphine-like effect) may occur.
Rigidity, which may also involve the thoracic muscles, can be avoided by the following measures: slow IV injection (usually sufficient for lower doses); premedication with benzodiazepines; use of muscle relaxants.
Non-epileptic (myo)clonic movements can occur.
Precautions: Fentanyl should be given only in an environment where the airway can be controlled and by personnel who can control the airway.
Special dosing conditions: The use of rapid bolus injections of opioids should be avoided in patients with compromised intracerebral compliance; in such patients the transient decrease in the mean arterial pressure has occasionally been accompanied by a transient reduction of the cerebral perfusion pressure.
It is recommended to reduce dosage in the elderly and debilitated patients. In uncontrolled hypothyroidism, pulmonary disease, decreased respiratory reserve, alcoholism and hepatic or renal impairment the dosage should be titrated with care and prolonged post-operative monitoring is required.
Patients on chronic opioid therapy or with a history of opioid abuse may require higher doses.
Myasthenia gravis: In patients with myasthenia gravis, careful consideration should be applied in the use of certain anticholinergic agents and neuromuscular-blocking pharmaceutical agents prior to, and during, the administration of a general anaesthetic regimen which includes administering intravenous fentanyl.
Interaction with neuroleptics: If fentanyl is administered with a neuroleptic, the user should be familiar with the special properties of each drug, particularly the difference in duration of action. When such a combination is used, there is a higher incidence of hypotension. Neuroleptics can induce extrapyramidal symptoms that can be controlled with anti-Parkinson agents.
Bile duct: As with other opioids, due to the anticholinergic effects administration of fentanyl may lead to increases of bile duct pressure and in isolated cases spasms of the Sphincter of Oddi might be observed.
Intestinal motility: As with other opioids, fentanyl can have inhibitory effect on intestinal motility. This should be considered in the pain management of intensive care patients with inflammatory or obstructive intestinal diseases.
Serotonin Syndrome: Caution is advised when fentanyl is co-administered with drugs that affect the serotonergic neurotransmitter systems.
The development of a potentially life-threatening serotonin syndrome may occur with the concomitant use of serotonergic drugs such as Selective Serotonin Re-uptake Inhibitors (SSRIs) and Serotonin Norepinephrine Re-uptake Inhibitors (SNRIs), and with drugs which impair metabolism of serotonin (including Monoamine Oxidase Inhibitors [MAOIs]). This may occur within the recommended dose.
Serotonin syndrome may include mental-status changes (e.g., agitation, hallucinations, coma), autonomic instability (e.g., tachycardia, labile blood pressure, hyperthermia), neuromuscular abnormalities (e.g., hyperoreflexia, incoordination, rigidity), and/or gastrointestinal symptoms (e.g., nausea, vomiting, diarrhoea).
If serotonin syndrome is suspected, rapid discontinuation of fentanyl should be considered.
Effects on ability to drive and use machines: Where early discharge is envisaged, patients should be advised not to drive or to operate machinery for at least 24 hours following administration.
This medicine can impair cognitive function and can affect a patient's ability to drive safely.
When prescribing this medicine, patients should be told: "The medicine is likely to affect your ability to drive"; "Do not drive until you know how the medicine affects you"; It is an offence to drive
while under the influence of this medicine.
However, patient would not be
committing an offence (called 'statutory defence') if: The medicine has been prescribed to treat a medical or dental problem and; Patient has taken it according to the instructions given by the prescriber and the information provided with the medicine and; it was not affecting the ability to drive safely.
Use in Children: Techniques that involve analgesia in a spontaneously breathing child should only be used as part of an anaesthetic technique, or given as part of a sedation/analgesia technique, with experienced personnel in an environment that can manage sudden chest wall rigidity requiring intubation, or apnoea requiring airway support.
Pregnancy: There are no adequate data from the use of fentanyl in pregnant women. Fentanyl can cross the placenta in early pregnancy. The potential risk for humans is unknown.
Administration during childbirth (including Caesarean section) is not recommended because fentanyl crosses the placenta and may suppress spontaneous respiration in the newborn period. If fentanyl is administered, assisted ventilation equipment must be immediately available for the mother and infant if required. An opioid antagonist for the child must always be available.
Lactation: Fentanyl is excreted into human milk. Therefore breast-feeding or use of expressed breast milk is not recommended within 24 hours of treatment. The risk/benefit of breast-feeding following fentanyl administration should be considered.
Fertility: There are no clinical data on the effects of fentanyl on male or female fertility. In animal studies, some tests on rats showed reduced female fertility at maternal toxic doses.
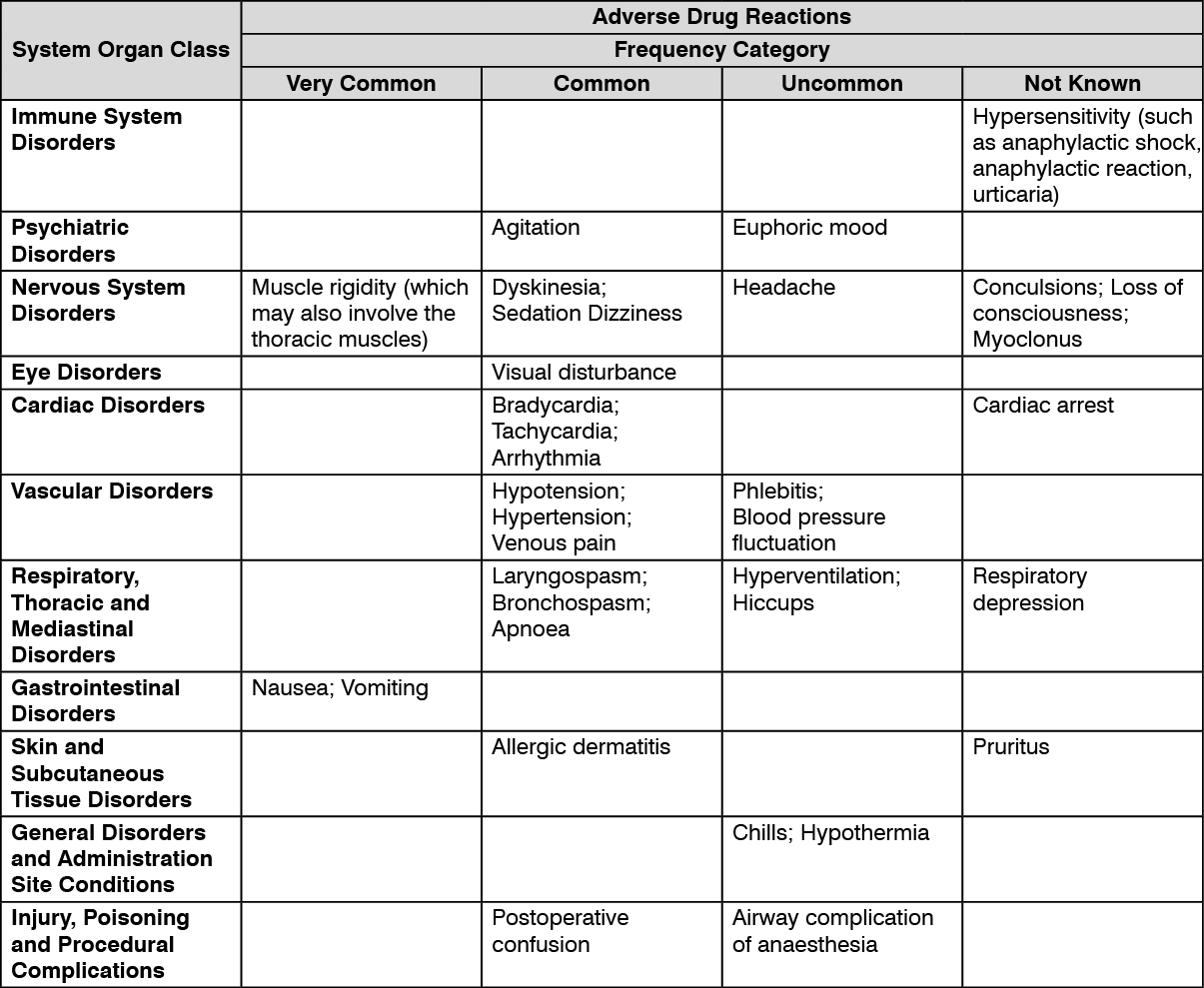
(See table.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
When a neuroleptic is used with fentanyl, the following adverse reactions may be observed: chills and/or shivering, restlessness, postoperative hallucinatory episodes and extrapyramidal symptoms.
Postmarketing Experience: Serotonin syndrome (See Precautions); Adrenal insufficiency (See Precautions).
Androgen deficiency: Cases of androgen deficiency have occurred with chronic use of opioids. Chronic use of opioids may influence the hypothalamic-pituitary-gonadal axis, leading to androgen deficiency that may manifest as low libido, impotence, erectile dysfunction, amenorrhea, or infertility. The causal role of opioids in the clinical syndrome of hypogonadism is unknown because the various medical, physical, lifestyle, and psychological stressors that may influence gonadal hormone levels have not been adequately controlled for in studies conducted to date. Patients presenting with symptoms of androgen deficiency should undergo laboratory evaluation. Infertility: Chronic use of opioids may cause reduced fertility in females and males of reproductive potential. It is not known whether these effects on fertility are reversible.
Effect of other drugs on fentanyl.
Central Nervous System (CNS) depressants: The use of opioid premedication, barbiturates, benzodiazepines, neuroleptics, general anaesthetics and other non-selective CNS depressants (e.g. alcohol) may enhance or prolong the respiratory depression of fentanyl.
When patients have received other CNS-depressants, the dose of fentanyl required may be less than usual. Concomitant use with fentanyl in spontaneously breathing patients may increase the risk of respiratory depression, profound sedation, coma, and death.
The pharmacological effects of fentanyl citrate can be reversed by naloxone.
Antipsychotics: Droperidol: The concomitant use of droperidol can result in a higher incidence of hypotension.
Antihypertensive: Clonidine : Co-administration of clonidine may enhance fentanyl effects and especially prolong fentanyl-induced respiratory depression.
Cytochrome P450 3A4 (CYP3A4) inhibitors: Fentanyl, a high clearance drug, is rapidly and extensively metabolised mainly by CYP3A4. When IV fentanyl is used, the concomitant use of a CYP3A4 inhibitor may result in a decrease in fentanyl clearance. With single-dose IV fentanyl administration, the period of risk for respiratory depression may be prolonged, which may require special patient care and longer observation. With multiple-dose fentanyl administration, the risk for acute and/or delayed respiratory depression may be increased, and a dose reduction of fentanyl may be required to avoid accumulation of fentanyl.
Oral ritonavir (a potent CYP3A4 inhibitor) reduced the clearance of a single IV fentanyl dose by two thirds, although peak plasma concentrations of IV fentanyl were not affected. However itraconazole (another potent CYP3A4 inhibitor) at 200 mg/day given orally for 4 days had no significant effect on the pharmacokinetics of a single dose of IV fentanyl.
Co-administration of fluconazole or voriconazole (moderate CYP3A4 inhibitors) and fentanyl may result in an increased exposure and/or prolonged exposure to fentanyl.
Bradycardia and possibly cardiac arrest can occur when fentanyl is combined with non-vagolytic muscle relaxants (e.g. vecuronium).
Serotonergic Drugs: Coadministration of fentanyl with a serotonergic agent, such as a Selective Serotonin Re-uptake Inhibitor (SSRI) or a Serotonin Norepinephrine Re-uptake Inhibitor (SNRI) or a Monoamine Oxidase Inhibitor (MAOI), may increase the risk of serotonin syndrome, a potentially life-threatening condition.
Effect of fentanyl on other drugs: Following the administration of fentanyl, the dose of other CNS depressant drugs should be reduced. This is particularly important after surgery, because profound analgesia is accompanied by marked respiratory depression, which can persist or recur in the postoperative period. Administration of a CNS depressant, such as a benzodiazepine, during this period may disproportionally increase the risk for respiratory depression.
Plasma concentrations of etomidate increased considerably (by a factor 2-3) when combined with fentanyl. The total plasma clearance and volume of distribution of etomidate is decreased by a factor of 2 to 3 without a change in half-life when administered with fentanyl.
Simultaneous administration of fentanyl and intravenous midazolam results in an increase in the terminal plasma half-life and a reduction in the plasma clearance of midazolam. When these drugs are co-administered with fentanyl their dose may need to be reduced.
Incompatibilities: The injectable solution must not be mixed with other products.
If desired, Fentanyl may be mixed with 0.9 % sodium chloride and 5 % glucose solutions.
Such dilutions are compatible with plastic infusion sets. These should be used within 24 hours of preparation.
Fentanyl citrate is reportedly physically incompatible with pentobarbital sodium, methohexital sodium, thiopental sodium and nafcilline.
Special Precautions for Disposal and Other Handling: The injection is for single patient use and should be used immediately after opening. The injection should not be used if particles are present. Any unused portion should be discarded.
The product can be used either undiluted or diluted. Dilution ranges tested with 0.9 % sodium chloride and 5 % glucose solutions are 1:1 and 1:25. Hence the maximal dilution must not exceed 1 part fentanyl with 25 parts 0.9 % sodium chloride and 5 % glucose solutions.
Keep the ampoules in the outer carton. Store below 30°C, protected from light.
Chemical and physical in-use stability has been demonstrated for 24 hours at 20-25°C.
From a microbiological point of view, the product should be used immediately.
Shelf-life: Shelf-life of the product as package for sale: 24 Months.
Shelf-life after first opening: use immediately.
Shelf-life after dilution: 24 hours at 20 to 25°C.
N02AB03 - fentanyl ; Belongs to the class of phenylpiperidine derivative opioids. Used to relieve pain.
Trofentyl soln for inj 50 mcg/mL
2 mL x 5 × 1's


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out
