Pharmacotherapeutic Group: Immunosuppressants, tumour necrosis factor alpha (TNF
α) inhibitors.
ATC Code: L04AB02.
Pharmacology: Pharmacodynamics: Mechanism of action: Infliximab is a chimeric human-murine monoclonal antibody that binds with high affinity to both soluble and transmembrane forms of TNF
α but not to lymphotoxin α (TNF
β).
Pharmacodynamic effects: Infliximab inhibits the functional activity of TNF
α in a wide variety of
in vitro bioassays. Infliximab prevented disease in transgenic mice that develop polyarthritis as a result of constitutive expression of human TNF
α and when administered after disease onset, it allowed eroded joints to heal.
In vivo, infliximab rapidly forms stable complexes with human TNF
α, a process that parallels the loss of TNF
α bioactivity.
Elevated concentrations of TNF
α have been found in the joints of rheumatoid arthritis patients and correlate with elevated disease activity. In rheumatoid arthritis, treatment with infliximab reduced infiltration of inflammatory cells into inflamed areas of the joint as well as expression of molecules mediating cellular adhesion, chemoattraction and tissue degradation. After infliximab treatment, patients exhibited decreased levels of serum interleukin 6 (IL-6) and C-reactive protein (CRP), and increased haemoglobin levels in rheumatoid arthritis patients with reduced haemoglobin levels, compared with baseline. Peripheral blood lymphocytes further showed no significant decrease in number or in proliferative responses to
in vitro mitogenic stimulation when compared with untreated patients' cells. In psoriasis patients, treatment with infliximab resulted in decreases in epidermal inflammation and normalisation of keratinocyte differentiation in psoriatic plaques. In psoriatic arthritis, short term treatment with Remicade reduced the number of T-cells and blood vessels in the synovium and psoriatic skin.
Histological evaluation of colonic biopsies, obtained before and 4 weeks after administration of infliximab, revealed a substantial reduction in detectable TNF
α. Infliximab treatment of Crohn's disease patients was also associated with a substantial reduction of the commonly elevated serum inflammatory marker, CRP. Total peripheral white blood cell counts were minimally affected in infliximab-treated patients, although changes in lymphocytes, monocytes and neutrophils reflected shifts towards normal ranges. Peripheral blood mononuclear cells (PBMC) from infliximab-treated patients showed undiminished proliferative responsiveness to stimuli compared with untreated patients, and no substantial changes in cytokine production by stimulated PBMC were observed following treatment with infliximab. Analysis of lamina propria mononuclear cells obtained by biopsy of the intestinal mucosa showed that infliximab treatment caused a reduction in the number of cells capable of expressing TNF
α and interferon γ. Additional histological studies provided evidence that treatment with infliximab reduces the infiltration of inflammatory cells into affected areas of the intestine and the presence of inflammation markers at these sites. Endoscopic studies of intestinal mucosa have shown evidence of mucosal healing in infliximab-treated patients.
Clinical efficacy and safety: Adult rheumatoid arthritis: The efficacy of infliximab was assessed in two multicentre, randomised, double-blind, pivotal clinical studies: ATTRACT and ASPIRE. In both studies concurrent use of stable doses of folic acid, oral corticosteroids (≤ 10 mg/day) and/or non-steroidal antiinflammatory drugs (NSAIDs) was permitted.
The primary endpoints were the reduction of signs and symptoms as assessed by the American College of Rheumatology criteria (ACR20 for ATTRACT, landmark ACR-N for ASPIRE), the prevention of structural joint damage, and the improvement in physical function. A reduction in signs and symptoms was defined to be at least a 20% improvement (ACR20) in both tender and swollen joint counts, and in 3 of the following 5 criteria: evaluator's global assessment, patient's global assessment, functional/disability measure, visual analogue pain scale and erythrocyte sedimentation rate or C-reactive protein. ACR-N uses the same criteria as the ACR20, calculated by taking the lowest percent improvement in swollen joint count, tender joint count, and the median of the remaining 5 components of the ACR response. Structural joint damage (erosions and joint space narrowing) in both hands and feet was measured by the change from baseline in the total van der Heijde-modified Sharp score (0-440). The Health Assessment Questionnaire (HAQ; scale 0-3) was used to measure patients' average change from baseline scores over time, in physical function.
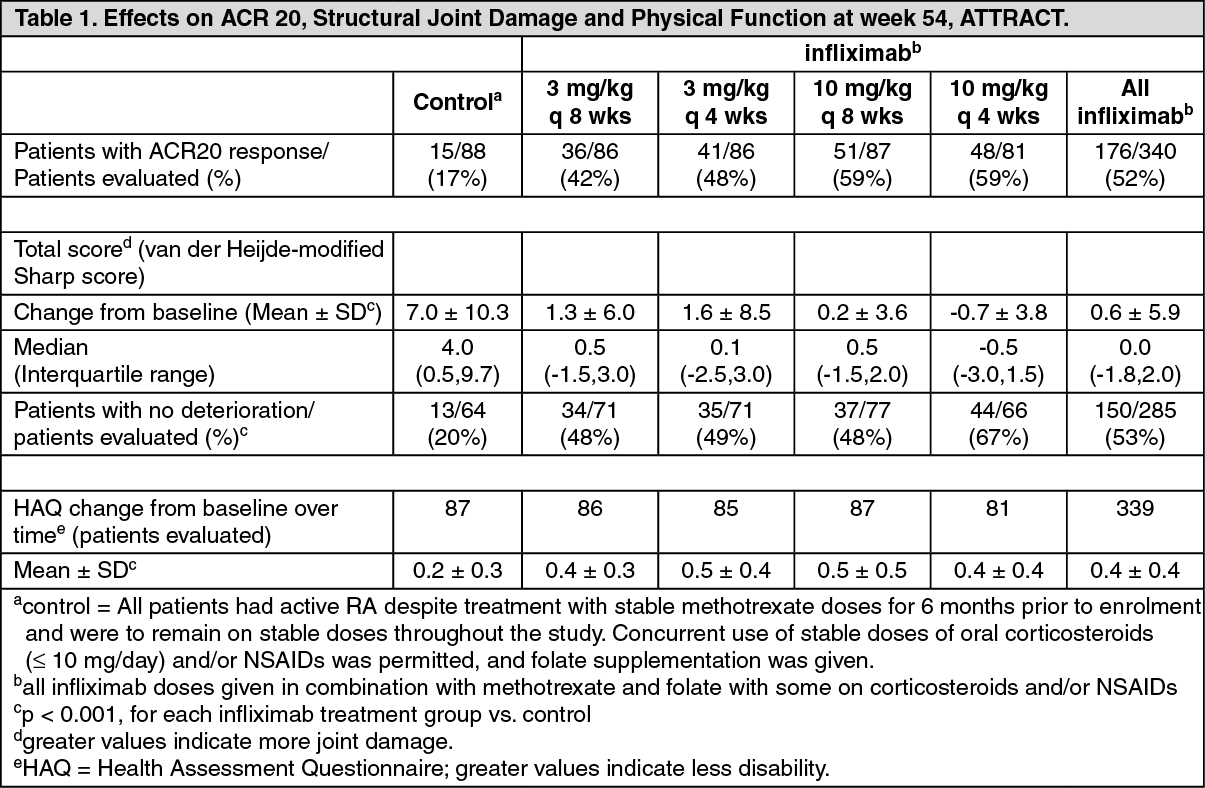
The ATTRACT study evaluated responses at 30, 54 and 102 weeks in a placebo-controlled study of 428 patients with active rheumatoid arthritis despite treatment with methotrexate. Approximately 50% of patients were in functional Class III. Patients received placebo, 3 mg/kg or 10 mg/kg infliximab at weeks 0, 2 and 6, and then every 4 or 8 weeks thereafter. All patients were on stable methotrexate doses (median 15 mg/wk) for 6 months prior to enrolment and were to remain on stable doses throughout the study.
Results from week 54 (ACR20, total van der Heijde-modified Sharp score and HAQ) are shown in Table 1. Higher degrees of clinical response (ACR50 and ACR70) were observed in all infliximab groups at 30 and 54 weeks compared with methotrexate alone.
A reduction in the rate of the progression of structural joint damage (erosions and joint space narrowing) was observed in all infliximab groups at 54 weeks (Table 1).
The effects observed at 54 weeks were maintained through 102 weeks. Due to a number of treatment withdrawals, the magnitude of the effect difference between infliximab and the methotrexate alone group cannot be defined. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
The ASPIRE study evaluated responses at 54 weeks in 1,004 methotrexate naive patients with early (≤ 3 years disease duration, median 0.6 years) active rheumatoid arthritis (median swollen and tender joint count of 19 and 31, respectively). All patients received methotrexate (optimised to 20 mg/wk by week 8) and either placebo, 3 mg/kg or 6 mg/kg infliximab at weeks 0, 2, and 6 and every 8 weeks thereafter. Results from week 54 are shown in Table 2.
After 54 weeks of treatment, both doses of infliximab + methotrexate resulted in statistically significantly greater improvement in signs and symptoms compared to methotrexate alone as measured by the proportion of patients achieving ACR20, 50 and 70 responses.
In ASPIRE, more than 90% of patients had at least two evaluable X-rays. Reduction in the rate of progression of structural damage was observed at weeks 30 and 54 in the infliximab + methotrexate groups compared to methotrexate alone. (See Table 2.)
Click on icon to see table/diagram/image
Data to support dose titration in rheumatoid arthritis come from ATTRACT, ASPIRE and the START study. START was a randomised, multicenter, double-blind, 3-arm, parallel-group safety study. In one of the study arms (group 2, n = 329), patients with an inadequate response were allowed to dose titrate with 1.5 mg/kg increments from 3 up to 9 mg/kg. The majority (67%) of these patients did not require any dose titration. Of the patients who required a dose titration, 80% achieved clinical response and the majority (64%) of these required only one adjustment of 1.5 mg/kg.
Adult Crohn's disease: Induction treatment in moderately to severely active Crohn's disease: The efficacy of a single dose treatment with infliximab was assessed in 108 patients with active Crohn's disease (Crohn's Disease Activity Index (CDAI) ≥ 220 ≤ 400) in a randomised, double-blinded, placebo-controlled, dose-response study. Of these 108 patients, 27 were treated with the recommended dosage of infliximab 5 mg/kg. All patients had experienced an inadequate response to prior conventional therapies. Concurrent use of stable doses of conventional therapies was permitted, and 92% of patients continued to receive these therapies.
The primary endpoint was the proportion of patients who experienced a clinical response, defined as a decrease in CDAI by ≥ 70 points from baseline at the 4-week evaluation and without an increase in the use of medicinal products or surgery for Crohn's disease. Patients who responded at week 4 were followed to week 12. Secondary endpoints included the proportion of patients in clinical remission at week 4 (CDAI < 150) and clinical response over time.
At week 4, following administration of a single dose, 22/27 (81%) of infliximab-treated patients receiving a 5 mg/kg dose achieved a clinical response vs. 4/25 (16%) of the placebo-treated patients (p < 0.001). Also at week 4, 13/27 (48%) of infliximab-treated patients achieved a clinical remission (CDAI < 150) vs. 1/25 (4%) of placebo-treated patients. A response was observed within 2 weeks, with a maximum response at 4 weeks. At the last observation at 12 weeks, 13/27 (48%) of infliximab-treated patients were still responding.
Maintenance treatment in moderately to severely active Crohn's disease in adults: The efficacy of repeated infusions with infliximab was studied in a 1-year clinical study (ACCENT I).
A total of 573 patients with moderately to severely active Crohn's disease (CDAI ≥ 220 ≤ 400) received a single infusion of 5 mg/kg at week 0. 178 of the 580 enrolled patients (30.7%) were defined as having severe disease (CDAI score > 300 and concomitant corticosteroid and/or immunosuppressants) corresponding to the population defined in the indication (see Indications/Uses). At week 2, all patients were assessed for clinical response and randomised to one of 3 treatment groups; a placebo maintenance group, 5 mg/kg maintenance group and 10 mg/kg maintenance group. All 3 groups received repeated infusions at week 2, 6 and every 8 weeks thereafter.
Of the 573 patients randomised, 335 (58%) achieved clinical response by week 2. These patients were classified as week-2 responders and were included in the primary analysis (see Table 3). Among patients classified as non-responders at week 2, 32% (26/81) in the placebo maintenance group and 42% (68/163) in the infliximab group achieved clinical response by week 6. There was no difference between groups in the number of late responders thereafter.
The co-primary endpoints were the proportion of patients in clinical remission (CDAI < 150) at week 30 and time to loss of response through week 54. Corticosteroid tapering was permitted after week 6. (See Table 3.)
Click on icon to see table/diagram/image
Beginning at week 14, patients who had responded to treatment, but subsequently lost their clinical benefit, were allowed to cross over to a dose of infliximab 5 mg/kg higher than the dose to which they were originally randomised. Eighty nine percent (50/56) of patients who lost clinical response on infliximab 5 mg/kg maintenance therapy after week 14 responded to treatment with infliximab 10 mg/kg.
Improvements in quality of life measures, a reduction in disease-related hospitalisations and corticosteroid use were seen in the infliximab maintenance groups compared with the placebo maintenance group at weeks 30 and 54.
Infliximab with or without AZA was assessed in a randomised, double-blind, active comparator study (SONIC) of 508 adult patients with moderate to severe Crohn's disease (CDAI ≥ 220 ≤ 450) who were naive to biologics and immunosuppressants and had a median disease duration of 2.3 years. At baseline 27.4% of patients were receiving systemic corticosteroids, 14.2% of patients were receiving budesonide, and 54.3% of patients were receiving 5-ASA compounds. Patients were randomised to receive AZA monotherapy, infliximab monotherapy, or infliximab plus AZA combination therapy. Infliximab was administered at a dose of 5 mg/kg at weeks 0, 2, 6, and then every 8 weeks. AZA was given at a dose of 2.5 mg/kg daily.
The primary endpoint of the study was corticosteroid-free clinical remission at week 26, defined as patients in clinical remission (CDAI of < 150) who, for at least 3 weeks, had not taken oral systemic corticosteroids (prednisone or equivalent) or budesonide at a dose > 6 mg/day. For results see Table 4. The proportions of patients with mucosal healing at week 26 were significantly greater in the infliximab plus AZA combination (43.9%, p < 0.001) and infliximab monotherapy groups (30.1%, p = 0.023) compared to the AZA monotherapy group (16.5%). (See Table 4.)
Click on icon to see table/diagram/image
Similar trends in the achievement of corticosteroid-free clinical remission were observed at week 50. Furthermore, improved quality of life as measured by IBDQ was observed with infliximab.
Induction treatment in fistulising active Crohn's disease: The efficacy was assessed in a randomised, double-blinded, placebo-controlled study in 94 patients with fistulising Crohn's disease who had fistulae that were of at least 3 months' duration. Thirty one of these patients were treated with infliximab 5 mg/kg. Approximately 93% of the patients had previously received antibiotic or immunosuppressive therapy.
Concurrent use of stable doses of conventional therapies was permitted, and 83% of patients continued to receive at least one of these therapies. Patients received three doses of either placebo or infliximab at weeks 0, 2 and 6. Patients were followed up to 26 weeks. The primary endpoint was the proportion of patients who experienced a clinical response, defined as ≥ 50% reduction from baseline in the number of fistulae draining upon gentle compression on at least two consecutive visits (4 weeks apart), without an increase in the use of medicinal products or surgery for Crohn's disease.
Sixty eight percent (21/31) of infliximab-treated patients receiving a 5 mg/kg dose regimen achieved a clinical response vs. 26% (8/31) placebo-treated patients (p = 0.002). The median time to onset of response in the infliximab-treated group was 2 weeks. The median duration of response was 12 weeks. Additionally, closure of all fistulae was achieved in 55% of infliximab-treated patients compared with 13% of placebo-treated patients (p = 0.001).
Maintenance treatment in fistulising active Crohn's disease: The efficacy of repeated infusions with infliximab in patients with fistulising Crohn's disease was studied in a 1-year clinical study (ACCENT II). A total of 306 patients received 3 doses of infliximab 5 mg/kg at week 0, 2 and 6. At baseline, 87% of the patients had perianal fistulae, 14% had abdominal fistulae, 9% had rectovaginal fistulae. The median CDAI score was 180. At week 14, 282 patients were assessed for clinical response and randomised to receive either placebo or 5 mg/kg infliximab every 8 weeks through week 46.
Week-14 responders (195/282) were analysed for the primary endpoint, which was time from randomisation to loss of response (see Table 5). Corticosteroid tapering was permitted after week 6. (See Table 5.)
Click on icon to see table/diagram/image
Beginning at week 22, patients who initially responded to treatment and subsequently lost their response were eligible to cross over to active re-treatment every 8 weeks at a dose of infliximab 5 mg/kg higher than the dose to which they were originally randomised. Among patients in the infliximab 5 mg/kg group who crossed over because of loss of fistula response after week 22, 57% (12/21) responded to re-treatment with infliximab 10 mg/kg every 8 weeks.
There was no significant difference between placebo and infliximab for the proportion of patients with sustained closure of all fistulas through week 54, for symptoms such as proctalgia, abscesses and urinary tract infection or for number of newly developed fistulas during treatment.
Maintenance therapy with infliximab every 8 weeks significantly reduced disease-related hospitalisations and surgeries compared with placebo. Furthermore, a reduction in corticosteroid use and improvements in quality of life were observed.
Adult ulcerative colitis: The safety and efficacy of Remicade were assessed in two (ACT 1 and ACT 2) randomised, double-blind, placebo-controlled clinical studies in adult patients with moderately to severely active ulcerative colitis (Mayo score 6 to 12; Endoscopy subscore ≥ 2) with an inadequate response to conventional therapies [oral corticosteroids, aminosalicylates and/or immunomodulators (6-MP, AZA)]. Concomitant stable doses of oral aminosalicylates, corticosteroids, and/or immunomodulatory agents were permitted. In both studies, patients were randomised to receive either placebo, 5 mg/kg Remicade, or 10 mg/kg Remicade at weeks 0, 2, 6, 14 and 22, and in ACT 1 at weeks 30, 38 and 46. Corticosteroid taper was permitted after week 8. (See Table 6.)
Click on icon to see table/diagram/image
The efficacy of Remicade through week 54 was assessed in the ACT 1 study.
At 54 weeks, 44.9% of patients in the combined infliximab treatment group were in clinical response compared to 19.8% in the placebo treatment group (p < 0.001). Clinical remission and mucosal healing occurred in a greater proportion of patients in the combined infliximab treatment group compared to the placebo treatment group at week 54 (34.6% vs. 16.5%, p < 0.001 and 46.1% vs. 18.2%, p < 0.001, respectively). The proportions of patients in sustained response and sustained remission at week 54 were greater in the combined infliximab treatment group than in the placebo treatment group (37.9% vs. 14.0%, p < 0.001; and 20.2% vs. 6.6%, p < 0.001, respectively).
A greater proportion of patients in the combined infliximab treatment group were able to discontinue corticosteroids while remaining in clinical remission compared to the placebo treatment group at both week 30 (22.3% vs. 7.2%, p < 0.001, pooled ACT 1 & ACT 2 data) and week 54 (21.0% vs. 8.9%, p = 0.022, ACT1 data).
The pooled data analysis from the ACT 1 and ACT 2 studies and their extensions, analysed from baseline through 54 weeks, demonstrated a reduction of ulcerative colitis-related hospitalisations and surgical procedures with infliximab treatment. The number of ulcerative colitis-related hospitalisations was significantly lower in the 5 and 10 mg/kg infliximab treatment groups than in the placebo group (mean number of hospitalisations per 100 subject-years: 21 and 19 vs. 40 in the placebo group; p = 0.019 and p = 0.007, respectively). The number of ulcerative colitis-related surgical procedures was also lower in the 5 and 10 mg/kg infliximab treatment groups than in the placebo group (mean number of surgical procedures per 100 subject-years: 22 and 19 vs. 34; p = 0.145 and p = 0.022, respectively).
The proportion of subjects who underwent colectomy at any time within 54 weeks following the first infusion of study agent were collected and pooled from the ACT 1 and ACT 2 studies and their extensions. Fewer subjects underwent colectomy in the 5 mg/kg infliximab group (28/242 or 11.6% [N.S.]) and the 10 mg/kg infliximab group (18/242 or 7.4% [p = 0.011]) than in the placebo group (36/244; 14.8%).
The reduction in incidence of colectomy was also examined in another randomised, double-blind study (C0168Y06) in hospitalised patients (n = 45) with moderately to severely active ulcerative colitis who failed to respond to intravenous corticosteroids and who were therefore at higher risk for colectomy. Significantly fewer colectomies occurred within 3 months of study infusion in patients who received a single dose of 5 mg/kg infliximab compared to patients who received placebo (29.2% vs. 66.7% respectively, p = 0.017).
In ACT 1 and ACT 2, infliximab improved quality of life, confirmed by statistically significant improvement in both a disease specific measure, IBDQ, and by improvement in the generic 36-item short form survey SF-36.
Adult ankylosing spondylitis: Efficacy and safety of infliximab were assessed in two multicenter, double-blind, placebo-controlled studies in patients with active ankylosing spondylitis (Bath Ankylosing Spondylitis Disease Activity Index [BASDAI] score ≥ 4 and spinal pain ≥ 4 on a scale of 1-10).
In the first study (P01522), which had a 3 month double-blind phase, 70 patients received either 5 mg/kg infliximab or placebo at weeks 0, 2, 6 (35 patients in each group). At week 12, placebo patients were switched to infliximab 5 mg/kg every 6 weeks up to week 54. After the first year of the study, 53 patients continued into an open-label extension to week 102.
In the second clinical study (ASSERT), 279 patients were randomised to receive either placebo (Group 1, n = 78) or 5 mg/kg infliximab (Group 2, n = 201) at 0, 2 and 6 weeks and every 6 weeks to week 24. Thereafter, all subjects continued on infliximab every 6 weeks to week 96. Group 1 received 5 mg/kg infliximab. In group 2, starting with the week 36 infusion, patients who had a BASDAI ≥ 3 at 2 consecutive visits, received 7.5 mg/kg infliximab every 6 weeks thereafter through week 96.
In ASSERT, improvement in signs and symptoms was observed as early as week 2. At week 24, the number of ASAS 20 responders was 15/78 (19%) in the placebo group, and 123/201 (61%) in the 5 mg/kg infliximab group (p < 0.001). There were 95 subjects from group 2 who continued on 5 mg/kg every 6 weeks. At 102 weeks there were 80 subjects still on infliximab treatment and among those, 71 (89%) were ASAS 20 responders.
In P01522, improvement in signs and symptoms was also observed as early as week 2. At week 12, the number of BASDAI 50 responders were 3/35 (9%) in the placebo group, and 20/35 (57%) in the 5 mg/kg group (p < 0.01). There were 53 subjects who continued on 5 mg/kg every 6 weeks. At 102 weeks there were 49 subjects still on infliximab treatment and among those, 30 (61%) were BASDAI 50 responders.
In both studies, physical function and quality of life as measured by the BASFI and the physical component score of the SF-36 were also improved significantly.
Adult psoriatic arthritis: Efficacy and safety were assessed in two multicenter, double-blind, placebo-controlled studies in patients with active psoriatic arthritis.
In the first clinical study (IMPACT), efficacy and safety of infliximab were studied in 104 patients with active polyarticular psoriatic arthritis. During the 16-week double-blind phase, patients received either 5 mg/kg infliximab or placebo at weeks 0, 2, 6, and 14 (52 patients in each group). Starting at week 16, placebo patients were switched to infliximab and all patients subsequently received 5 mg/kg infliximab every 8 weeks up to week 46. After the first year of the study, 78 patients continued into an open-label extension to week 98.
In the second clinical study (IMPACT 2), efficacy and safety of infliximab were studied in 200 patients with active psoriatic arthritis (≥ 5 swollen joints and ≥ 5 tender joints). Forty six percent of patients continued on stable doses of methotrexate (≤ 25 mg/week). During the 24-week double-blind phase, patients received either 5 mg/kg infliximab or placebo at weeks 0, 2, 6, 14, and 22 (100 patients in each group). At week 16, 47 placebo patients with < 10% improvement from baseline in both swollen and tender joint counts were switched to infliximab induction (early escape). At week 24, all placebo-treated patients crossed over to infliximab induction. Dosing continued for all patients through week 46.
Key efficacy results for IMPACT and IMPACT 2 are shown in Table 7 as follows: (See Table 7.)
Click on icon to see table/diagram/image
In IMPACT and IMPACT 2, clinical responses were observed as early as week 2 and were maintained through week 98 and week 54 respectively. Efficacy has been demonstrated with or without concomitant use of methotrexate. Decreases in parameters of peripheral activity characteristic of psoriatic arthritis (such as number of swollen joints, number of painful/tender joints, dactylitis and presence of enthesopathy) were seen in the infliximab-treated patients.
Radiographic changes were assessed in IMPACT 2. Radiographs of hands and feet were collected at baseline, weeks 24 and 54. Infliximab treatment reduced the rate of progression of peripheral joint damage compared with placebo treatment at the week 24 primary endpoint as measured by change from baseline in total modified vdH-S score (mean ± SD score was 0.82 ± 2.62 in the placebo group compared with -0.70 ± 2.53 in the infliximab group; p < 0.001). In the infliximab group, the mean change in total modified vdH-S score remained below 0 at the week 54 timepoint.
Infliximab-treated patients demonstrated significant improvement in physical function as assessed by HAQ. Significant improvements in health-related quality of life were also demonstrated as measured by the physical and mental component summary scores of the SF-36 in IMPACT 2.
Adult psoriasis: The efficacy of infliximab was assessed in two multicenter, randomised, double-blind studies: SPIRIT and EXPRESS. Patients in both studies had plaque psoriasis (Body Surface Area [BSA] ≥ 10% and Psoriasis Area and Severity Index [PASI] score ≥ 12). The primary endpoint in both studies was the percent of patients who achieved ≥ 75% improvement in PASI from baseline at week 10.
SPIRIT evaluated the efficacy of infliximab induction therapy in 249 patients with plaque psoriasis that had previously received PUVA or systemic therapy. Patients received either 3 or 5 mg/kg infliximab or placebo infusions at weeks 0, 2 and 6. Patients with a PGA score ≥ 3 were eligible to receive an additional infusion of the same treatment at week 26.
In SPIRIT, the proportion of patients achieving PASI 75 at week 10 was 71.7% in the 3 mg/kg infliximab group, 87.9% in the 5 mg/kg infliximab group, and 5.9% in the placebo group (p < 0.001). By week 26, twenty weeks after the last induction dose, 30% of patients in the 5 mg/kg group and 13.8% of patients in the 3 mg/kg group were PASI 75 responders. Between weeks 6 and 26, symptoms of psoriasis gradually returned with a median time to disease relapse of > 20 weeks. No rebound was observed.
EXPRESS evaluated the efficacy of infliximab induction and maintenance therapy in 378 patients with plaque psoriasis. Patients received 5 mg/kg infliximab- or placebo-infusions at weeks 0, 2 and 6 followed by maintenance therapy every 8 weeks through week 22 in the placebo group and through week 46 in the infliximab group. At week 24, the placebo group crossed over to infliximab induction therapy (5 mg/kg) followed by infliximab maintenance therapy (5 mg/kg). Nail psoriasis was assessed using the Nail Psoriasis Severity Index (NAPSI). Prior therapy with PUVA, methotrexate, cyclosporin, or acitretin had been received by 71.4% of patients, although they were not necessarily therapy resistant. Key results are presented in Table 8. In infliximab treated subjects, significant PASI 50 responses were apparent at the first visit (week 2) and PASI 75 responses by the second visit (week 6). Efficacy was similar in the subgroup of patients that were exposed to previous systemic therapies compared to the overall study population. (See Table 8.)
Click on icon to see table/diagram/image
Significant improvements from baseline were demonstrated in DLQI (p < 0.001) and the physical and mental component scores of the SF 36 (p < 0.001 for each component comparison).
Paediatric population: Paediatric Crohn's disease (6 to 17 years): In the REACH study, 112 patients (6 to 17 years, median age 13.0 years) with moderate to severe, active Crohn's disease (median paediatric CDAI of 40) and an inadequate response to conventional therapies were to receive 5 mg/kg infliximab at weeks 0, 2, and 6. All patients were required to be on a stable dose of 6-MP, AZA or MTX (35% were also receiving corticosteroids at baseline). Patients assessed by the investigator to be in clinical response at week 10 were randomised and received 5 mg/kg infliximab at either q8 weeks or q12 weeks as a maintenance treatment regimen. If response was lost during maintenance treatment, crossing over to a higher dose (10 mg/kg) and/or shorter dosing interval (q8 weeks) was allowed. Thirty two (32) evaluable paediatric patients crossed over (9 subjects in the q8 weeks and 23 subjects in the q12 weeks maintenance groups). Twenty four of these patients (75.0%) regained clinical response after crossing over.
The proportion of subjects in clinical response at week 10 was 88.4% (99/112). The proportion of subjects achieving clinical remission at week 10 was 58.9% (66/112).
At week 30, the proportion of subjects in clinical remission was higher in the q8 week (59.6%, 31/52) than the q12 week maintenance treatment group (35.3%, 18/51; p = 0.013). At week 54, the figures were 55.8% (29/52) and 23.5% (12/51) in the q8 weeks and q12 weeks maintenance groups, respectively (p < 0.001).
Data about fistulas were derived from PCDAI scores. Of the 22 subjects that had fistulas at baseline, 63.6% (14/22), 59.1% (13/22) and 68.2% (15/22) were in complete fistula response at week 10, 30 and 54, respectively, in the combined q8 weeks and q12 weeks maintenance groups.
In addition, statistically and clinically significant improvements in quality of life and height, as well as a significant reduction in corticosteroid use, were observed versus baseline.
Paediatric ulcerative colitis (6 to 17 years): The safety and efficacy of infliximab were assessed in a multicenter, randomised, open-label, parallel-group clinical study (C0168T72) in 60 paediatric patients aged 6 through 17 years (median age 14.5 years) with moderately to severely active ulcerative colitis (Mayo score of 6 to 12; endoscopic subscore ≥ 2) with an inadequate response to conventional therapies. At baseline 53% of patients were receiving immunomodulator therapy (6-MP, AZA and/or MTX) and 62% of patients were receiving corticosteroids. Discontinuation of immunomodulators and corticosteroid taper were permitted after week 0.
All patients received an induction regimen of 5 mg/kg infliximab at weeks 0, 2, and 6. Patients who did not respond to infliximab at week 8 (n = 15) received no further medicinal product and returned for safety follow-up. At week 8, 45 patients were randomised and received 5 mg/kg infliximab at either q8 weeks or q12 weeks as a maintenance treatment regimen.
The proportion of patients in clinical response at week 8 was 73.3% (44/60). Clinical response at week 8 was similar between those with or without concomitant immunomodulator use at baseline. Clinical remission at week 8 was 33.3% (17/51) as measured by the Paediatric Ulcerative Colitis Activity Index (PUCAI) score.
At week 54, the proportion of patients in clinical remission as measured by the PUCAI score was 38% (8/21) in the q8 week maintenance group and 18% (4/22) in the q12 week maintenance treatment group. For patients receiving corticosteroids at baseline, the proportion of patients in remission and not receiving corticosteroids at week 54 was 38.5% (5/13) for the q8 week and 0% (0/13) for the q12 week maintenance treatment group.
In this study, there were more patients in the 12 to 17 year age group than in the 6 to 11 year age group (45/60 vs.15/60). While the numbers of patients in each subgroup are too small to draw definitive conclusions about the effect of age, there was a higher number of patients in the younger age group who stepped up in dose or discontinued treatment due to inadequate efficacy.
Pharmacokinetics: Single intravenous infusions of 1, 3, 5, 10 or 20 mg/kg of infliximab yielded dose proportional increases in the maximum serum concentration (C
max) and area under the concentration-time curve (AUC). The volume of distribution at steady state (median V
d of 3.0 to 4.1 litres) was not dependent on the administered dose and indicated that infliximab is predominantly distributed within the vascular compartment. No time-dependency of the Pharmacokinetics was observed. The elimination pathways for infliximab have not been characterised. Unchanged infliximab was not detected in urine. No major age- or weight-related differences in clearance or volume of distribution were observed in rheumatoid arthritis patients. The pharmacokinetics of infliximab in elderly patients has not been studied. Studies have not been performed in patients with liver or renal disease.
At single doses of 3, 5, or 10 mg/kg, the median C
max values were 77, 118 and 277 micrograms/ml, respectively. The median terminal half-life at these doses ranged from 8 to 9.5 days. In most patients, infliximab could be detected in the serum for at least 8 weeks after the recommended single dose of 5 mg/kg for Crohn's disease and the rheumatoid arthritis maintenance dose of 3 mg/kg every 8 weeks.
Repeated administration of infliximab (5 mg/kg at 0, 2 and 6 weeks in fistulising Crohn's disease, 3 or 10 mg/kg every 4 or 8 weeks in rheumatoid arthritis) resulted in a slight accumulation of infliximab in serum after the second dose. No further clinically relevant accumulation was observed. In most fistulising Crohn's disease patients, infliximab was detected in serum for 12 weeks (range 4-28 weeks) after administration of the regimen.
Paediatric population: Population pharmacokinetic analysis based on data obtained from patients with ulcerative colitis (N = 60), Crohn's disease (N = 112), juvenile rheumatoid arthritis (N = 117) and Kawasaki disease (N = 16) with an overall age range from 2 months to 17 years indicated that exposure to infliximab was dependent on body weight in a non-linear way. Following administration of 5 mg/kg Remicade every 8 weeks, the predicted median steady-state infliximab exposure (area under concentration-time curve at steady state, AUC
ss) in paediatric patients aged 6 years to 17 years was approximately 20% lower than the predicted median steady-state drug exposure in adults. The median AUC
ss in paediatric patients aged 2 years to less than 6 years was predicted to be approximately 40% lower than that in adults, although the number of patients supporting this estimate is limited.
Toxicology: Preclinical safety data: Infliximab does not cross react with TNF
α from species other than human and chimpanzees. Therefore, conventional preclinical safety data with infliximab are limited. In a developmental toxicity study conducted in mice using an analogous antibody that selectively inhibits the functional activity of mouse TNF
α, there was no indication of maternal toxicity, embryotoxicity or teratogenicity. In a fertility and general reproductive function study, the number of pregnant mice was reduced following administration of the same analogous antibody. It is not known whether this finding was due to effects on the males and/or the females. In a 6-month repeated dose toxicity study in mice, using the same analogous antibody against mouse TNF
α, crystalline deposits were observed on the lens capsule of some of the treated male mice. No specific ophthalmologic examinations have been performed in patients to investigate the relevance of this finding for humans.
Long-term studies have not been performed to evaluate the carcinogenic potential of infliximab. Studies in mice deficient in TNF
α demonstrated no increase in tumours when challenged with known tumour initiators and/or promoters.



 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image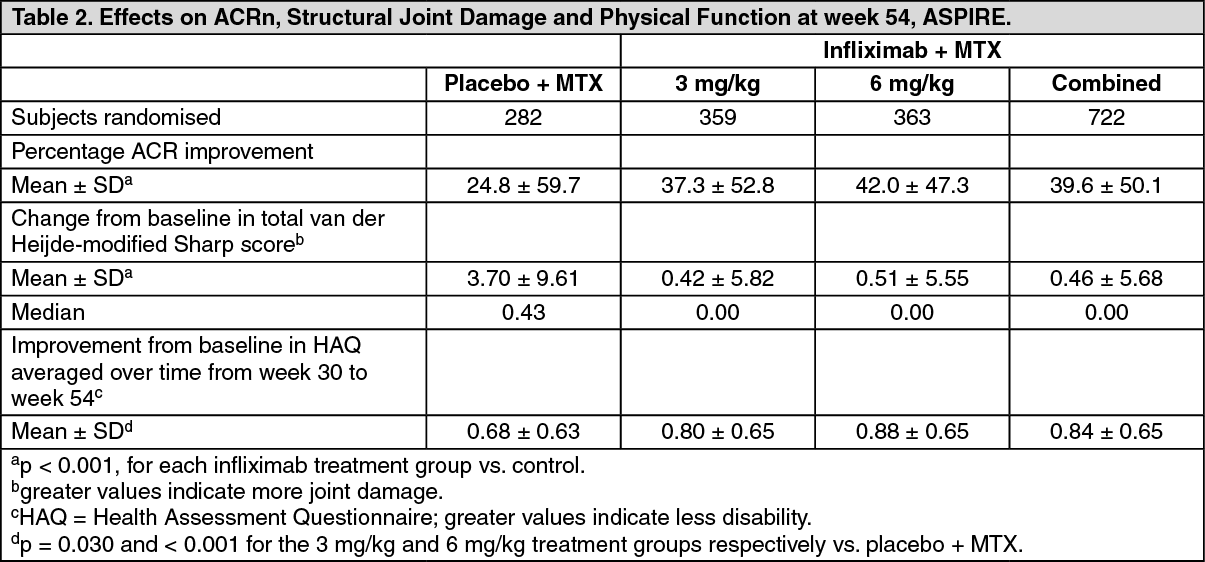 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image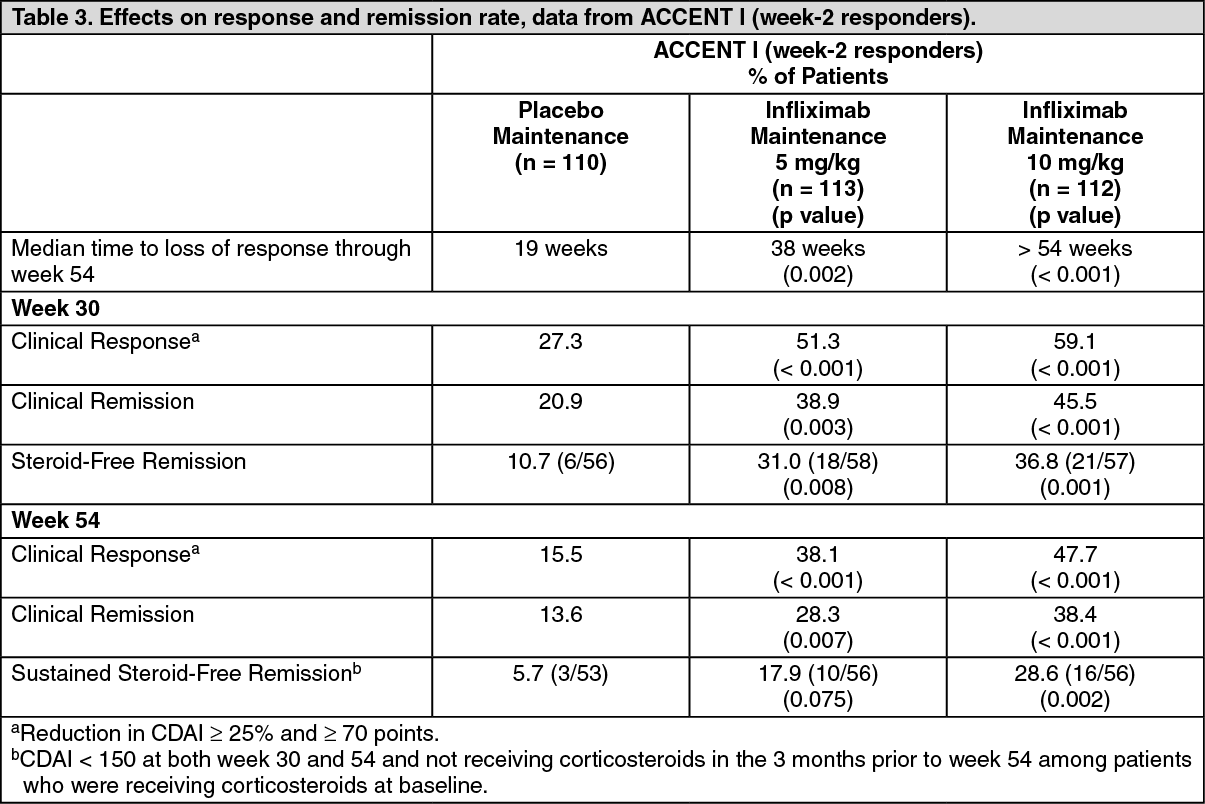 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image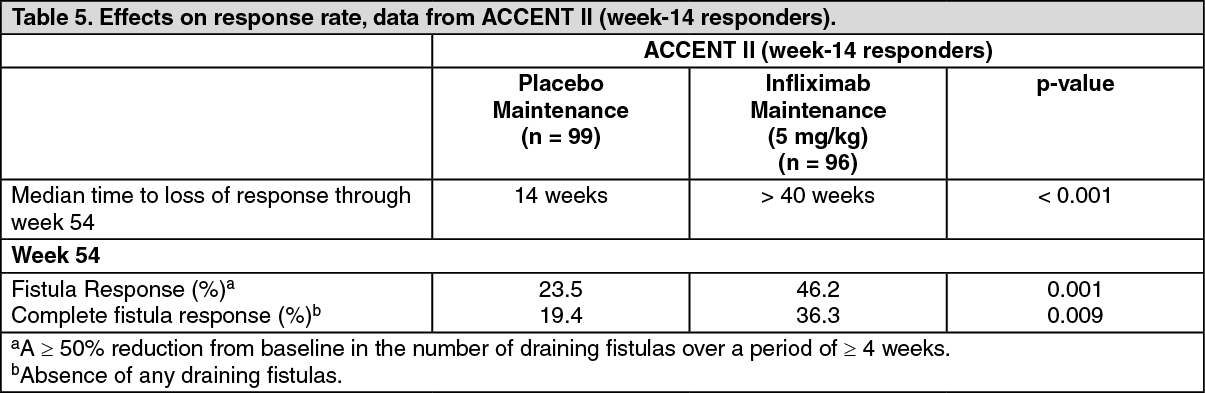 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image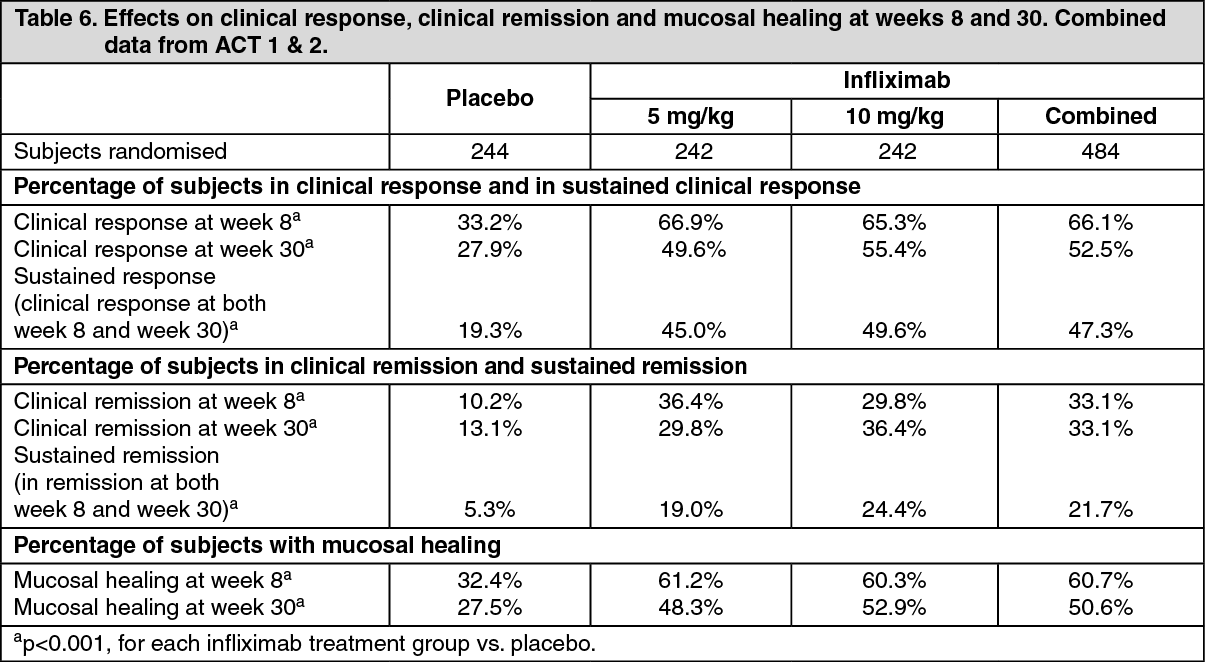 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image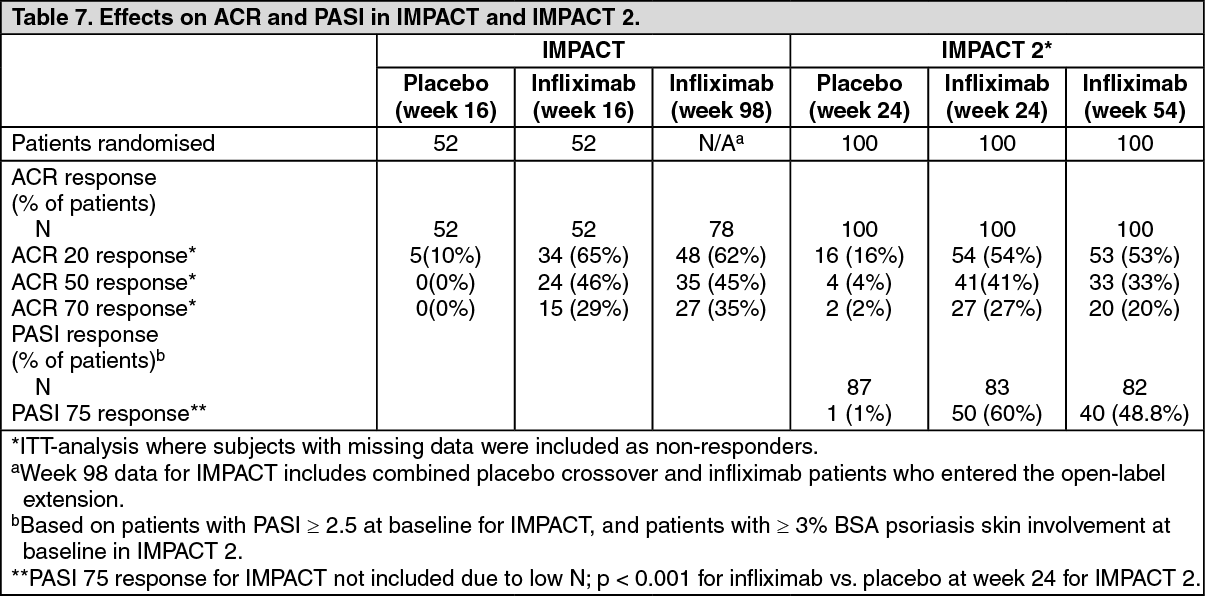 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image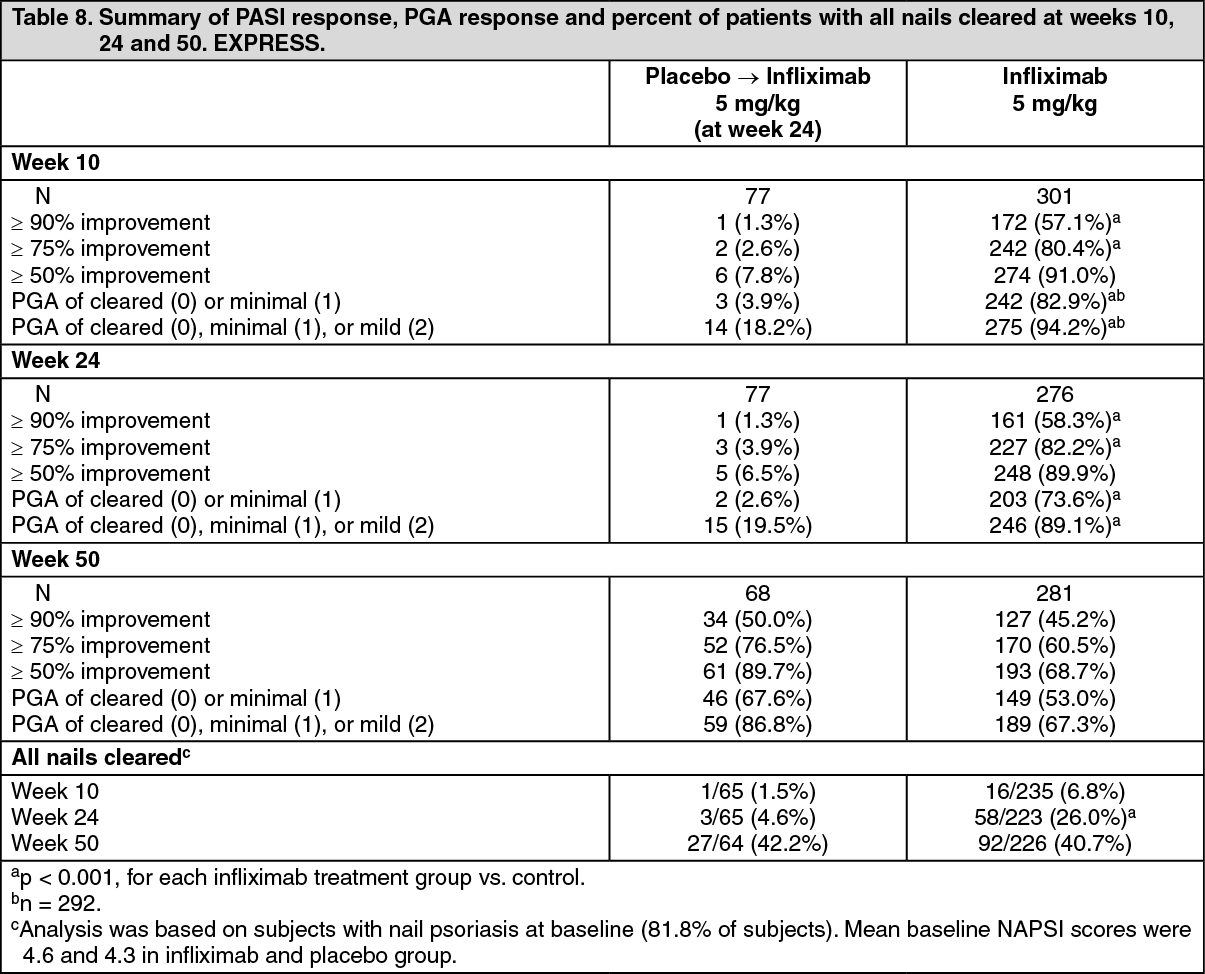 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image 100 mg2dba21bf-956d-43ae-be88-9faa000a5683.GIF)

 Sign Out
Sign Out
