


 Sign Out
Sign Out


Tabulated list of adverse reactions: Table 9 lists ADRs based on experience from clinical studies as well as adverse reactions, some with fatal outcome, reported from post-marketing experience. Within the organ system classes, adverse reactions are listed under headings of frequency using the following categories: very common (≥ 1/10); common (≥ 1/100 to < 1/10); uncommon (≥ 1/1,000 to < 1/100); rare (≥ 1/10,000 to < 1/1,000); very rare (< 1/10,000), not known (cannot be estimated from the available data). Within each frequency grouping, undesirable effects are presented in order of decreasing seriousness. (See Table 9.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageInfusion-related reactions: An infusion-related reaction was defined in clinical studies as any adverse event occurring during an infusion or within 1 hour after an infusion. In Phase III clinical studies, 18% of infliximab-treated patients compared with 5% of placebo-treated patients experienced an infusion-related reaction. Overall, a higher proportion of patients receiving infliximab monotherapy experienced an infusion-related reaction compared to patients receiving infliximab with concomitant immunomodulators. Approximately 3% of patients discontinued treatment due to infusion-related reactions and all patients recovered with or without medical therapy. Of infliximab-treated patients who had an infusion reaction during the induction period, through week 6, 27% experienced an infusion reaction during the maintenance period, week 7 through week 54. Of patients who did not have an infusion reaction during the induction period, 9% experienced an infusion reaction during the maintenance period.
In a clinical study of patients with rheumatoid arthritis (ASPIRE), infusions were to be administered over 2 hours for the first 3 infusions. The duration of subsequent infusions could be shortened to not less than 40 minutes in patients who did not experience serious infusion reactions. In this trial, sixty six percent of the patients (686 out of 1,040) received at least one shortened infusion of 90 minutes or less and 44% of the patients (454 out of 1,040) received at least one shortened infusion of 60 minutes or less. Of the infliximab-treated patients who received at least one shortened infusion, infusion-related reactions occurred in 15% of patients and serious infusion reactions occurred in 0.4% of patients.
In a clinical study of patients with Crohn's disease (SONIC), infusion-related reactions occurred in 16.6% (27/163) of patients receiving infliximab monotherapy, 5% (9/179) of patients receiving infliximab in combination with AZA, and 5.6% (9/161) of patients receiving AZA monotherapy. One serious infusion reaction (< 1%) occurred in a patient on infliximab monotherapy.
In post-marketing experience, cases of anaphylactic-like reactions, including laryngeal/pharyngeal oedema and severe bronchospasm, and seizure have been associated with Remicade administration (see Precautions).
Cases of transient visual loss occurring during or within 2 hours of Remicade infusion have been reported. Events (some fatal) of myocardial ischaemia/infarction and arrhythmia have also been reported, some in close temporal association with infusion of infliximab; cerebrovascular accidents have also been reported in close temporal association with infusion of infliximab.
Infusion reactions following re-administration of Remicade: A clinical study in patients with moderate to severe psoriasis was designed to assess the efficacy and safety of long-term maintenance therapy versus re-treatment with an induction regimen of Remicade (maximum of four infusions at 0, 2, 6 and 14 weeks) following disease flare. Patients did not receive any concomitant immunosuppressant therapy. In the re-treatment arm, 4% (8/219) of patients experienced a serious infusion reaction versus < 1% (1/222) on maintenance therapy. The majority of serious infusion reactions occurred during the second infusion at week 2. The interval between the last maintenance dose and the first re-induction dose ranged from 35-231 days. Symptoms included, but were not limited to, dyspnea, urticaria, facial oedema, and hypotension. In all cases, Remicade treatment was discontinued and/or other treatment instituted with complete resolution of signs and symptoms.
Delayed hypersensitivity: In clinical studies delayed hypersensitivity reactions have been uncommon and have occurred after Remicade-free intervals of less than 1 year. In the psoriasis studies, delayed hypersensitivity reactions occurred early in the treatment course. Signs and symptoms included myalgia and/or arthralgia with fever and/or rash, with some patients experiencing pruritus, facial, hand or lip oedema, dysphagia, urticaria, sore throat and headache.
There are insufficient data on the incidence of delayed hypersensitivity reactions after Remicade-free intervals of more than 1 year but limited data from clinical studies suggest an increased risk for delayed hypersensitivity with increasing Remicade-free interval (see Precautions).
In a 1-year clinical study with repeated infusions in patients with Crohn's disease (ACCENT I study), the incidence of serum sickness-like reactions was 2.4%.
Immunogenicity: Patients who developed antibodies to infliximab were more likely (approximately 2-3 fold) to develop infusion-related reactions. Use of concomitant immunosuppressant agents appeared to reduce the frequency of infusion-related reactions.
In clinical studies using single and multiple infliximab doses ranging from 1 to 20 mg/kg, antibodies to infliximab were detected in 14% of patients with any immunosuppressant therapy, and in 24% of patients without immunosuppressant therapy. In rheumatoid arthritis patients who received the recommended repeated treatment dose regimens with methotrexate, 8% of patients developed antibodies to infliximab. In psoriatic arthritis patients who received 5 mg/kg with and without methotrexate, antibodies occurred overall in 15% of patients (antibodies occurred in 4% of patients receiving methotrexate and in 26% of patients not receiving methotrexate at baseline). In Crohn's disease patients who received maintenance treatment, antibodies to infliximab occurred overall in 3.3% of patients receiving immunosuppressants and in 13.3% of patients not receiving immunosuppressants. The antibody incidence was 2-3 fold higher for patients treated episodically. Due to methodological limitations, a negative assay did not exclude the presence of antibodies to infliximab. Some patients who developed high titres of antibodies to infliximab had evidence of reduced efficacy. In psoriasis patients treated with infliximab as a maintenance regimen in the absence of concomitant immunomodulators, approximately 28% developed antibodies to infliximab (see "Infusion reactions and hypersensitivity" under Precautions).
Infections: Tuberculosis, bacterial infections, including sepsis and pneumonia, invasive fungal, viral, and other opportunistic infections have been observed in patients receiving Remicade. Some of these infections have been fatal; the most frequently reported opportunistic infections with a mortality rate of > 5% include pneumocystosis, candidiasis, listeriosis and aspergillosis (see Precautions).
In clinical studies 36% of infliximab-treated patients were treated for infections compared with 25% of placebo-treated patients.
In rheumatoid arthritis clinical studies, the incidence of serious infections including pneumonia was higher in infliximab plus methotrexate-treated patients compared with methotrexate alone especially at doses of 6 mg/kg or greater (see Precautions).
In post-marketing spontaneous reporting, infections are the most common serious adverse reaction. Some of the cases have resulted in a fatal outcome. Nearly 50% of reported deaths have been associated with infection. Cases of tuberculosis, sometimes fatal, including miliary tuberculosis and tuberculosis with extra-pulmonary location have been reported (see Precautions).
Malignancies and lymphoproliferative disorders: In clinical studies with infliximab in which 5,780 patients were treated, representing 5,494 patient years, 5 cases of lymphomas and 26 non-lymphoma malignancies were detected as compared with no lymphomas and 1 non-lymphoma malignancy in 1,600 placebo-treated patients representing 941 patient years.
In long-term safety follow-up of clinical studies with infliximab of up to 5 years, representing 6,234 patients-years (3,210 patients), 5 cases of lymphoma and 38 cases of non-lymphoma malignancies were reported.
Cases of malignancies, including lymphoma, have also been reported in the post-marketing setting (see Precautions).
In an exploratory clinical study involving patients with moderate to severe COPD who were either current smokers or ex-smokers, 157 adult patients were treated with Remicade at doses similar to those used in rheumatoid arthritis and Crohn's disease. Nine of these patients developed malignancies, including 1 lymphoma. The median duration of follow-up was 0.8 years (incidence 5.7% [95% CI 2.65%-10.6%]. There was one reported malignancy amongst 77 control patients (median duration of follow-up 0.8 years; incidence 1.3% [95% CI 0.03%-7.0%]). The majority of the malignancies developed in the lung or head and neck.
A population-based retrospective cohort study found an increased incidence of cervical cancer in women with rheumatoid arthritis treated with infliximab compared to biologics-naive patients or the general population, including those over 60 years of age (see Precautions).
In addition, post-marketing cases of hepatosplenic T-cell lymphoma have been reported in patients treated with Remicade with the vast majority of cases occurring in Crohn's disease and ulcerative colitis, and most of whom were adolescent or young adult males (see Precautions).
Heart failure: In a Phase II study aimed at evaluating Remicade in CHF, higher incidence of mortality due to worsening of heart failure were seen in patients treated with Remicade, especially those treated with the higher dose of 10 mg/kg (i.e. twice the maximum approved dose). In this study 150 patients with NYHA Class III-IV CHF (left ventricular ejection fraction ≤ 35%) were treated with 3 infusions of Remicade 5 mg/kg, 10 mg/kg, or placebo over 6 weeks. At 38 weeks, 9 of 101 patients treated with Remicade (2 at 5 mg/kg and 7 at 10 mg/kg) died compared to one death among the 49 patients on placebo.
There have been post-marketing reports of worsening heart failure, with and without identifiable precipitating factors, in patients taking Remicade. There have also been post-marketing reports of new onset heart failure, including heart failure in patients without known pre-existing cardiovascular disease. Some of these patients have been under 50 years of age.
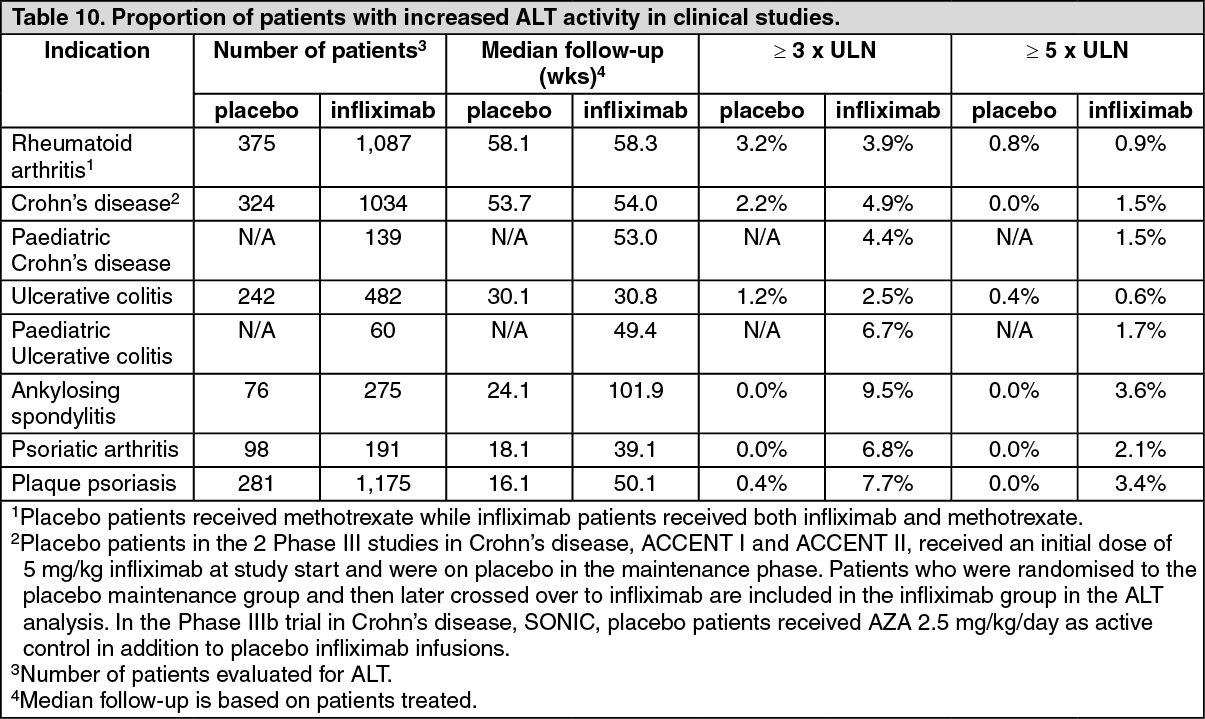
Hepatobiliary events: In clinical studies, mild or moderate elevations of ALT and AST have been observed in patients receiving Remicade without progression to severe hepatic injury. Elevations of ALT ≥ 5 x Upper Limit of Normal (ULN) have been observed (see Table 10). Elevations of aminotransferases were observed (ALT more common than AST) in a greater proportion of patients receiving Remicade than in controls, both when Remicade was given as monotherapy and when it was used in combination with other immunosuppressive agents. Most aminotransferase abnormalities were transient; however, a small number of patients experienced more prolonged elevations. In general, patients who developed ALT and AST elevations were asymptomatic, and the abnormalities decreased or resolved with either continuation or discontinuation of Remicade, or modification of concomitant therapy. In post-marketing surveillance, cases of jaundice and hepatitis, some with features of autoimmune hepatitis, have been reported in patients receiving Remicade (see Precautions). (See Table 10.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageAntinuclear antibodies (ANA)/Anti-double-stranded DNA (dsDNA) antibodies: Approximately half of infliximab-treated patients in clinical studies who were ANA negative at baseline developed a positive ANA during the study compared with approximately one fifth of placebo-treated patients. Anti-dsDNA antibodies were newly detected in approximately 17% of infliximab-treated patients compared with 0% of placebo-treated patients. At the last evaluation, 57% of infliximab-treated patients remained anti-dsDNA positive. Reports of lupus and lupus-like syndromes, however, remain uncommon (see Precautions).
Paediatric population: Paediatric Crohn's disease patients: The following adverse reactions were reported more commonly in paediatric Crohn's disease patients in the REACH study (see Pharmacology: Pharmacodynamics under Actions) than in adult Crohn's disease patients: anaemia (10.7%), blood in stool (9.7%), leucopenia (8.7%), flushing (8.7%), viral infection (7.8%), neutropenia (6.8%), bacterial infection (5.8%), and respiratory tract allergic reaction (5.8%). In addition, bone fracture (6.8%) was reported, however, a causal association has not been established. Other special considerations are discussed as follows.
Infusion-related reactions: In REACH, 17.5% of randomised patients experienced 1 or more infusion reactions. There were no serious infusion reactions, and 2 subjects in REACH had non-serious anaphylactic reactions.
Immunogenicity: Antibodies to infliximab were detected in 3 (2.9%) paediatric patients.
Infections: In the REACH study, infections were reported in 56.3% of randomised subjects treated with infliximab. Infections were reported more frequently for subjects who received q8 week as opposed to q12 week infusions (73.6% and 38.0%, respectively), while serious infections were reported for 3 subjects in the q8 week and 4 subjects in the q12 week maintenance treatment group. The most commonly reported infections were upper respiratory tract infection and pharyngitis, and the most commonly reported serious infection was abscess. Three cases of pneumonia (1 serious) and 2 cases of herpes zoster (both non-serious) were reported.
Paediatric ulcerative colitis patients: Overall, the adverse reactions reported in the paediatric ulcerative colitis trial (C0168T72) and adult ulcerative colitis (ACT 1 and ACT 2) studies were generally consistent. In C0168T72, the most common adverse reactions were upper respiratory tract infection, pharyngitis, abdominal pain, fever, and headache. The most common adverse event was worsening of ulcerative colitis, the incidence of which was higher in patients on the q12 week vs. the q8 week dosing regimen.
Infusion-related reactions: Overall, 8 (13.3%) of 60 treated patients experienced one or more infusion reactions, with 4 of 22 (18.2%) in the q8 week and 3 of 23 (13.0%) in the q12 week treatment maintenance group. No serious infusion reactions were reported. All infusion reactions were mild or moderate in intensity.
Immunogenicity: Antibodies to infliximab were detected in 4 (7.7%) patients through week 54.
Infections: Infections were reported in 31 (51.7%) of 60 treated patients in C0168T72 and 22 (36.7%) required oral or parenteral antimicrobial treatment. The proportion of patients with infections in C0168T72 was similar to that in the paediatric Crohn's disease study (REACH) but higher than the proportion in the adults ulcerative colitis studies (ACT 1 and ACT 2). The overall incidence of infections in C0168T72 was 13/22 (59%) in the every 8 week maintenance treatment group and 14/23 (60.9%) in the every 12 week maintenance treatment group. Upper respiratory tract infection (7/60 [12%]) and pharyngitis (5/60 [8%]) were the most frequently reported respiratory system infections. Serious infections were reported in 12% (7/60) of all treated patients.
In this study, there were more patients in the 12 to 17 year age group than in the 6 to 11 year age group (45/60 [75.0%]) vs.15/60 [25.0%]). While the numbers of patients in each subgroup are too small to make any definitive conclusions about the effect of age on safety events, there were higher proportions of patients with serious adverse events and discontinuation due to adverse events in the younger age group than in the older age group. While the proportion of patients with infections was also higher in the younger age group, for serious infections, the proportions were similar in the two age groups. Overall proportions of adverse events and infusion reactions were similar between the 6 to 11 and 12 to 17 year age groups.
Post-marketing experience: Post-marketing spontaneous serious adverse reactions with infliximab in the paediatric population have included malignancies including hepatosplenic T-cell lymphomas, transient hepatic enzyme abnormalities, lupus-like syndromes, and positive auto-antibodies (see Precautions and Adverse Reactions).
Additional information on special populations: Elderly: In rheumatoid arthritis clinical studies, the incidence of serious infections was greater in infliximab plus methotrexate-treated patients 65 years and older (11.3%) than in those under 65 years of age (4.6%). In patients treated with methotrexate alone, the incidence of serious infections was 5.2% in patients 65 years and older compared to 2.7% in patients under 65 (see Precautions).
View ADR Monitoring Form