


 Sign Out
Sign Out

Action in humans: Inhibition of gastric acid secretion: When PARIET was administered to healthy adult male volunteers at 10 mg or 20 mg once a day, gastrin-stimulated acid output was significantly decreased compared with the 1st day of administration. The mean percentages of acid output reduction compared with the day before starting administration on day 1 and on day 7 were, at 10 mg once a day, 73% and 80%, and at 20 mg once a day, 88-89% and 99%, respectively.
Increase reaction of intragastric pH: When PARIET was administered to healthy adult male volunteers at 10 mg or 20 mg once a day, intragastric pH was significantly increased. The percentage of holding times above pH 4 and pH 3 in 24 hr on day 4 after treatment with 10 mg was 73% and 80% respectively, and for treatment with 20 mg was 78% and 83%, respectively.
Action in animals: Inhibition of H+, K+-ATPase (in vitro): Sodium rabeprazole strongly inhibits H+, K+-ATPase in preparations made from pig gastric mucosa.
Inhibition of gastric acid secretion: Sodium rabeprazole inhibits gastric acid secretion stimulated by dibutyl cyclic-AMP in isolated rabbit gastric glands (in vitro).
Sodium rabeprazole exhibits strong inhibition of gastric acid secretion stimulated by histamine or pentagastrin in chronic gastric fistula dogs as well as basal gastric acid secretion and histamine-stimulated gastric acid secretion in rats.
Compared to other proton pump inhibitors, the reversal of the antisecretory effect is more rapid with sodium rabeprazole and the increase in blood gastrin levels is less in dogs and rats.
Antiulcer action: In rats, sodium rabeprazole demonstrated a strong antiulcer action against various experimental ulcers and therapeutic activity in experimental gastric mucosal lesions (induced by cold restraint stress, water immersion stress, pyloric ligation, cysteamine or ethanol-hydrochloride).
Adjunctive effect on Helicobacter pylori Eradication: Susceptibility testing of H. pylori isolates was performed for amoxicillin and clarithromycin using agar dilution methodology, and minimum inhibitory concentrations (MICs) were determined.
Standardized susceptibility test procedures require the use of laboratory control microorganisms to control the technical aspects of the laboratory procedures.
Incidence of Antibiotic-Resistant Organisms Among Clinical Isolates: Pretreatment Resistance: Clarithromycin pretreatment resistance rate (MIC ≥ 1 mcg/mL) to H. pylori was 9% (51/560) at baseline in all treatment groups combined. A total of > 99% (558/560) of patients had H. pylori isolates which were considered to be susceptible (MIC ≤ 0.25 mcg/mL) to amoxicillin at baseline. Two patients had baseline H. pylori isolates with an amoxicillin MIC of 0.5 mcg/mL. (See Table 2.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imagePatients with persistent H. pylori infection following rabeprazole, amoxicillin, and clarithromycin therapy will likely have clarithromycin resistant clinical isolates. Therefore, clarithromycin susceptibility testing should be done when possible. If resistance to clarithromycin is demonstrated or susceptibility testing is not possible, alternative antimicrobial therapy should be instituted.
Amoxicillin Susceptibility Test Results and Clinical/Bacteriological Outcomes: In the U.S. multicenter study, a total of > 99% (558/560) of patients had H. pylori isolates which were considered to be susceptible (MIC ≤ 0.25 mcg/mL) to amoxicillin at baseline. The other 2 patients had baseline H. pylori isolates with an amoxicillin MIC of 0.5 mcg/mL, and both isolates were clarithromycin-resistant at baseline; in one case the H. pylori was eradicated. In the 7 and 10 day treatment groups 75% (107/145) and 79% (112/142), respectively, of the patients who had pretreatment amoxicillin susceptible MICs (≤ 0.25 mcg/mL) were eradicated of H. pylori. No patients developed amoxicillin-resistant H. pylori during therapy.
During treatment with antisecretory medicinal products, serum gastrin increases in response to the decreased acid secretion. Also, CgA increases due to decreased gastric acidity. The increased CgA level may interfere with investigations for neuroendocrine tumours.
Available published evidence suggests that proton pump inhibitors should be discontinued between 5 days and 2 weeks prior to CgA measurements. This is to allow CgA levels that might be spuriously elevated following PPI treatment to return to reference range.
Clinical Studies: Clinical efficacy: The results of open-labeled and double-blind clinical trials conducted with PARIET in patients with gastric ulcer, duodenal ulcer, reflux esophagitis and anastomotic ulcer are summarized in the following table. (See Table 3.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageThe overall improvement rate in 2 patients with Zollinger-Ellison syndrome was 100%.
It was demonstrated in clinical pharmacology studies that the increase in gastric pH was greater in the 20 mg group than in the 10 mg group, and the usefulness of PARIET in the treatment of intractable ulcer has been demonstrated using a dose of 20 mg once daily.
In addition, the clinical usefulness of PARIET in the treatment of gastric and duodenal ulcers has been demonstrated in double-blind clinical trials.
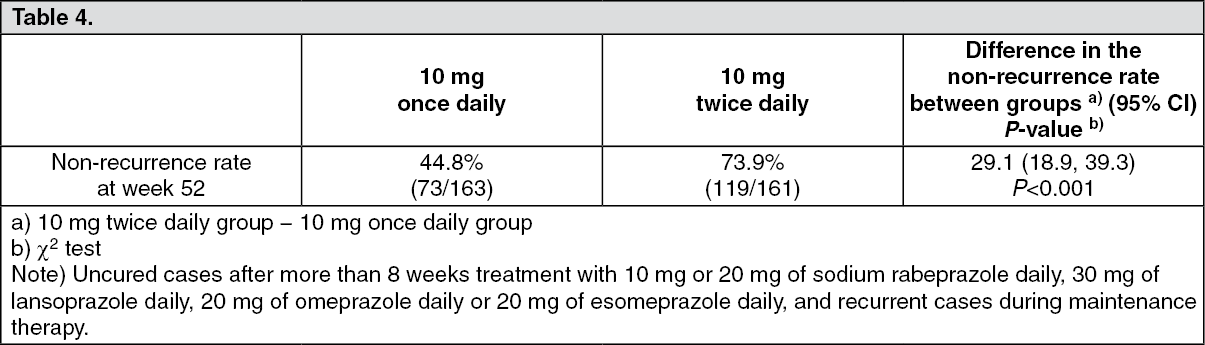
The following table shows endoscopic non-recurrence rate at week 52 in the Maintenance Period (Central Evaluation) with PARIET for patients with reflux esophagitis resistive to treatment note) with standard doses of proton pump inhibitors. (See Table 4.)
 Click on icon to see table/diagram/image
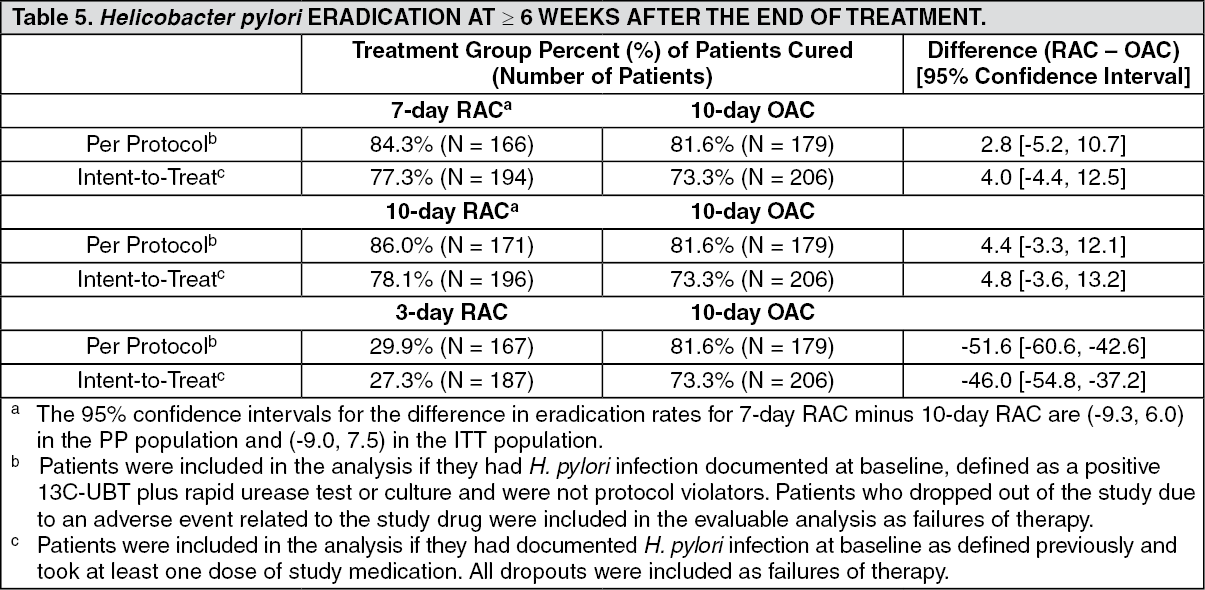
Click on icon to see table/diagram/imageHelicobacter pylori Eradication in Patients with Peptic Ulcer Disease or Symptomatic Non-Ulcer Disease in Adults: The U.S. multicenter study was a double-blind, parallel-group comparison of rabeprazole, amoxicillin, and clarithromycin for 3, 7, or 10 days vs. omeprazole, amoxicillin and clarithromycin for 10 days. Therapy consisted of rabeprazole 20 mg twice daily, amoxicillin 1000 mg twice daily, and clarithromycin 500 mg twice daily (RAC) or omeprazole 20 mg twice daily, amoxicillin 1000 mg twice daily, and clarithromycin 500 mg twice daily (OAC). Patients with H. pylori infection were stratified in a 1:1 ratio for those with peptic ulcer disease (active or a history of ulcer in the past five years) [PUD] and those who were symptomatic but without peptic ulcer disease [NPUD], as determined by upper gastrointestinal endoscopy. The overall H. pylori eradication rates, defined as negative 13C-UBT for H. pylori ≥ 6 weeks from the end of the treatment are shown in the following table. The eradication rates in the 7 day and 10 day RAC regimens were found to be similar to 10 day OAC regimen using either the Intent-to-Treat (ITT) or Per-Protocol (PP) populations. Eradication rates in the RAC 3 day regimen were inferior to the other regimens. (See Table 5.)
 Click on icon to see table/diagram/image
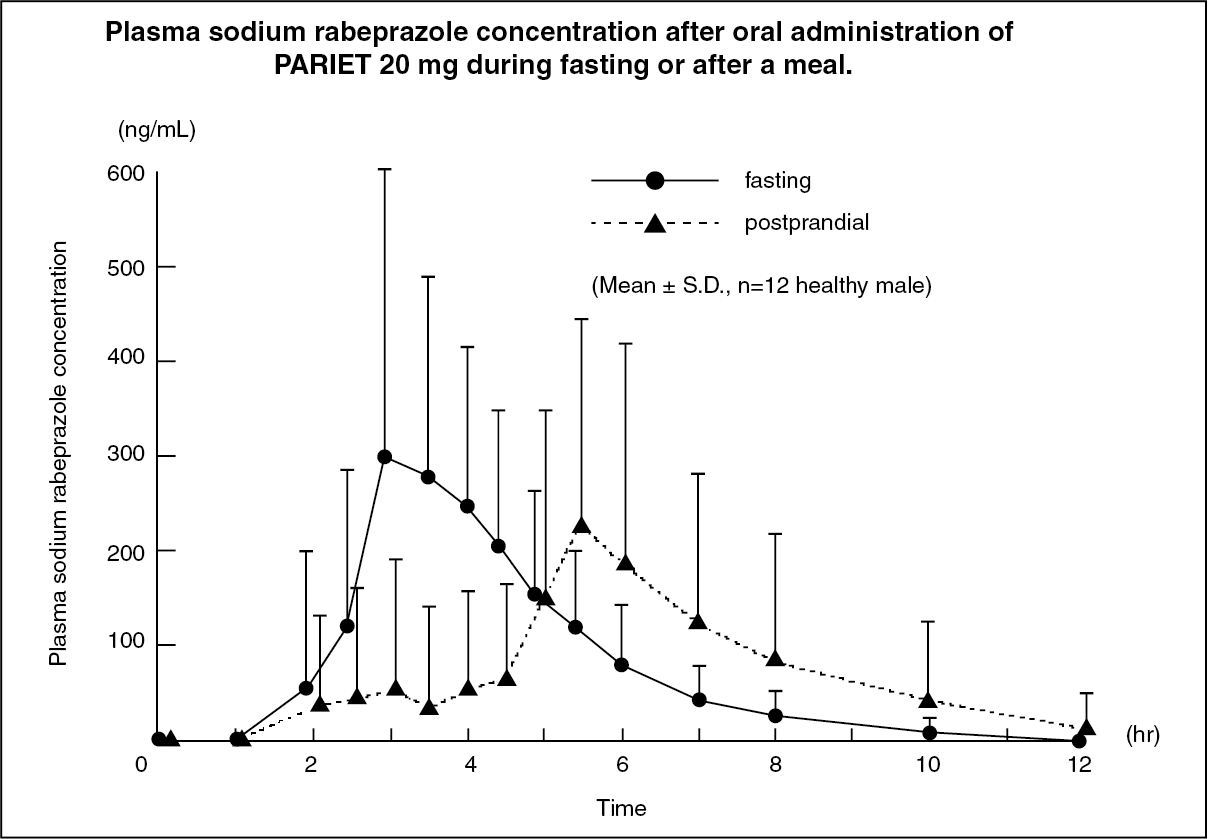
Click on icon to see table/diagram/imagePharmacokinetics: Blood concentrations: The changes over time in the mean plasma sodium rabeprazole concentration when administered orally to healthy adult male volunteers at a dose of 20 mg during fasting or after a meal are shown in the following figure. Mean values of pharmacokinetic parameters determined for individual subjects during fasting and postprandial administration of PARIET are presented in the following table. Tmax was prolonged by 1.7 hr after postprandial administration compared to administration during fasting, and inter-individual variations in absorption were observed. (See figure and Table 6.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageThe following table shows the mean values of pharmacokinetic parameters when sodium rabeprazole was administered orally to healthy adult male volunteers at doses of 10 mg and 20 mg during fasting. (See Table 7.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageMetabolism: When PARIET was administered orally to healthy adult male volunteers at single doses of 10 mg and 20 mg, the main metabolite recognized in plasma was its thioether-form product produced by non-enzymatic reduction reaction. Other metabolites were the demethylated products due to demethylation which involving the hepatic enzymatic metabolism of cytochrome P450 2C19 (CYP2C19), and the sulfone-form products due to sulfonation involving 3A4 (CYP3A4).
Urinary excretion: No unchanged drug was detected in the urine of healthy adult male volunteers up to 24 hr after oral administration of 20 mg of sodium rabeprazole, and about 29-40% of the dose was excreted in the urine as the carboxylic acid form and its glucuronide, and about 13-19% of the dose was present as the mercapturate conjugated-form.