The NICARDIA-XL-30 contains 30mg of Nifedipine.
Pharmacology: Pharmacodynamics: Nifedipine is a specific and potent calcium antagonist of the 1, 4-dihydropyridine type. Calcium antagonists reduce the transmembrane influx of calcium ions through the slow calcium channel into the cell. Nifedipine acts particularly on the cells of the myocardium and the smooth muscle cells of the coronary arteries and the peripheral resistance vessels. In hypertension, the main action of NICARDIA-XL-30 is to cause peripheral vasodilatation and thus reduce peripheral resistance. In angina, NICARDIA-XL-30 reduces peripheral and coronary vascular resistance, leading to an increase in coronary blood flow, cardiac output and stroke volume, whilst decreasing after-load. Additionally, nifedipine dilates submaximal both clear and atherosclerotic coronary arteries, thus protecting the heart against coronary artery spasm and improving perfusion to the ischaemic myocardium. Nifedipine reduces the frequency of painful attacks and the ischaemic ECG changes irrespective of the relative contribution from coronary artery spasm or atherosclerosis. NICARDIA-XL-30 administered twice-daily provides 24-hour control of raised blood pressure. NICARDIA-XL-30 causes reduction in blood pressure such that the percentage lowering is directly related to its initial level. In normotensive individuals, NICARDIA-XL-30 has little or no effect on blood pressure.
Pharmacokinetics: Absorption: After oral administration nifedipine is rapidly and almost completely absorbed. The systemic availability of orally administered nifedipine is 45 - 56 % owing to a first pass effect. Maximum plasma and serum concentrations are reached at 1.5 to 4.2 hours with NICARDIA-XL-30. Simultaneous food intake leads to delayed, but not reduced absorption.
Distribution: NICARDIA-XL-30 is about 95 % bound to plasma protein (albumin). The distribution half-life after intravenous administration was determined to be 5 to 6 minutes.
Biotransformation: After oral administration NICARDIA-XL-30 is metabolized in the gut wall and in the liver, primarily by oxidative processes. These metabolites show no pharmacodynamic activity. NICARDIA-XL-30 is excreted in the form of its metabolites predominantly via the kidneys and about 5 - 15 % via the bile in the faeces. The unchanged substance is recovered only in traces in the urine.
Elimination: The terminal elimination half-life is 6 - 11 hours, because of delayed absorption. In cases of impaired liver function the elimination half-life is distinctly prolonged and the total clearance is reduced. A dose reduction may be necessary in severe cases.
NICARDIA-XL-30 is a medicine for treatment of coronary heart disease; chronic stable angina pectoris (angina of effort). Treatment of hypertension.
As far as possible the treatment must be tailored to the needs of the individual. Depending on the clinical picture in each case, the basic dose must be introduced gradually. Unless otherwise prescribed, the following dosage guidelines are recommended for adults: For coronary heart disease: Chronic stable angina pectoris (angina of effort): NICARDIA-XL-30 tablet once daily (1 x 30 mg/day).
For hypertension: NICARDIA-XL-30 tablet once daily (1 x 30 mg/day).
In general therapy should be initiated with 30 mg once daily. Depending on the severity of the disease and the patient's response the dose can be increased in stages up to 120 mg once daily. Coadministration with CYP 3A4 inhibitors or CYP 3A4 inducers may result in the recommendation to adapt the nifedipine dose or not to use nifedipine at all (see Interactions).
Duration of Treatment: The attending doctor will determine the duration of use.
Administration: As a rule, NICARDIA-XL-30 tablet are swallowed whole with a little liquid, irrespective of meal times. Grapefruit juice is to be avoided (see Interactions).
Additional information on special populations: Children and adolescents: The safety and efficacy of NICARDIA-XL-30 in children below 18 years has not been established.
Geriatric patients: Based on pharmacokinetic data for NICARDIA-XL-30 no dose adaptation in elderly people above 65 years is necessary.
Patients with hepatic impairment: In patients with impaired liver function, careful monitoring and, in severe cases, a dose reduction may be necessary.
Patients with renal impairment: Based on pharmacokinetic data no dosage adjustment is required in patients with renal impairment (see Pharmacology: Pharmacokinetics under Actions). The tablets must not be chewed or broken up.
Symptoms: Overdosage or poisoning with NICARDIA-XL-30 may produce severe blood pressure fall, clouding of consciousness to the point of loss of consciousness, heart rhythm disturbances and breathlessness.
Treatment: As far as treatment is concerned, elimination of nifedipine and the restoration of stable cardiovascular conditions have priority. Elimination must be as complete as possible, including the small intestine, to prevent the otherwise inevitable subsequent absorption of the active substance. The benefit of gastric decontamination is uncertain.
a. Consider activated charcoal (50g for adults, 1g/kg for children) if the patient presents within 1 hour of ingestion of a potentially toxic amount.
b. Although it may seem reasonable to assume that late administration of activated charcoal may be beneficial for sustained release (SR, MR) preparations there is no evidence to support this.
c. Alternatively consider gastric lavage in adults within 1 hour of a potentially life- threatening overdose.
d. Consider further doses of activated charcoal every 4 hours if a clinically significant amount of a sustained release preparation has been ingested with a single dose of an osmotic laxative (e.g. sorbitol, lactulose or magnesium sulphate).
e. Asymptomatic patients should be observed for at least 4 hours after ingestion and for 12 hours if a sustained release preparation has been taken.
Haemodialysis serves no purpose as nifedipine is not dialysable, but plasmapheresis is advisable (high plasma protein binding, relatively low volume of distribution). Hypotension as a result of cardiogenic shock and arterial vasodilatation can be treated with calcium (10-20ml of a 10% calcium gluconate solution administered intravenously over 5-10 minutes). If the effects are inadequate, the treatment can be continued, with ECG monitoring. If an insufficient increase in blood pressure is achieved with calcium, vasoconstricting sympathomimetics such as dopamine or noradrenaline should be administered. The dosage of these drugs should be determined by the patient's response.
Symptomatic bradycardia may be treated with atropine, beta-sympathomimetics or a temporary cardiac pacemaker, as required. Additional fluids should be administered with caution to avoid cardiac overload.
NICARDIA-XL-30 must not be administered to patients with cardiovascular shock, with narrowing of the aorta (higher-grade aortic stenosis), with known hypersensitivity to NICARDIA-XL-30, with unstable angina pectoris and acute myocardial infarction (within the first 4 weeks).
NICARDIA-XL-30 should not be used to patients with extremely low blood pressure (severe hypotension with systolic blood pressure under 90mmHg) or existing (decompensated) heart muscle weakness.
NICARDIA-XL-30 should not be used for the treatment of acute attacks of angina.
NICARDIA-XL-30 should not be used for secondary prevention of myocardial infarction.
NICARDIA-XL-30 should not be administered concomitantly with rifampicin since effective plasma levels of nifedipine may not be achieved owing to enzyme induction.
NICARDIA-XL-30 should not be administrated to patients with hepatic impairment.
NICARDIA-XL-30 should not be administrated to patients with a history of gastro-intestinal obstruction, oesophageal obstruction or any degree of decreased lumen diameter of the gastro-intestinal tract.
NICARDIA-XL-30 must not be used in patients with a history of gastro-intestinal obstruction, oesophageal obstruction, any degree of decreased lumen diameters of the gastro-intestinal tract.
NICARDIA-XL-30 must not use in patient with a Kock pouch (ileostomy after Proctocolectomy).
NICARDIA-XL-30 is contra-indicated in patients with inflammatory bowel disease or Crohn's disease.
NICARDIA-XL-30 must be swallowed whole; under no circumstances should they be bitten, chewed or broken up.
Caution should be exercised in patients with hypotension as there is a risk of further reduction in blood pressure and care must be exercised in patients with very low blood pressure (severe hypotension with systolic blood pressure less than 90 mm Hg).
In patients with impaired liver function careful monitoring and, in severe cases, a dose reduction may be necessary.
NICARDIA-XL-30 may be used in combination with beta-blocking drugs and other antihypertensive agents but the possibility of an additive effect resulting in postural hypotension should be borne in mind. NICARDIA-XL-30 will not prevent possible rebound effects after cessation of other antihypertensive therapy.
NICARDIA-XL-30 should be used with caution in patients whose cardiac reserve is poor. Deterioration of heart failure has occasionally been observed with nifedipine.
Diabetic patients taking NICARDIA-XL-30 may require adjustment of their control as elevated blood glucose concentrations in serum (hyperglycaemia) upon taking.
Dialysis patients with severe, life-threatening high blood pressure (malignant hypertension) and irreversible kidney failure with reduced plasma volume (hypovolaemia) may experience particularly great blood pressure reduction through widening of blood vessels (vasodilation).
Nifedipine is metabolised via the cytochrome P450 3A4 system. Drugs that are known to either inhibit or to induce this enzyme system may therefore alter the first pass or the clearance of nifedipine.
Drugs, which are known inhibitors of the cytochrome P450 3A4 system, and which may therefore lead to increased plasma concentrations of nifedipine include, for example: Macrolide antibiotics (e.g., erythromycin); Anti-HIV protease inhibitors (e.g., ritonavir); Azole antimycotics (e.g., ketoconazole); The antidepressants, nefazodone and fluoxetine; quinupristin/dalfopristin; valproic acid; Cimetidine.
Upon co-administration with these drugs, the blood pressure should be monitored and, if necessary, a reduction of the nifedipine dose should be considered.
Treatment of high blood pressure with NICARDIA-XL-30 requires regular monitoring. Due to individually different reactions, alertness may be altered to such an extent that the ability to actively participate in road traffic or to operate machines or to work without a firm support is impaired. This applies especially at the start of treatment, when increasing the dose and when switching medicines as well as in combination with alcohol.
Pregnancy: NICARDIA-XL-30 should not be used during pregnancy unless the clinical condition of the woman requires treatment with nifedipine. NICARDIA-XL-30 should be reserved for women with severe hypertension who are unresponsive to standard therapy.
Careful monitoring of blood pressure must be exercised when administering NICARDIA-XL- 30 with I.V. magnesium sulfate, owing to the possibility of an excessive fall in blood pressure, which could harm both mother and foetus.
Lactation: NICARDIA-XL-30 is excreted in the breast milk. The NICARDIA-XL-30 concentration in the milk is almost comparable with mother serum concentration. For immediate release formulations, it is proposed to delay breastfeeding or milk expression for 3 to 4 hours after drug administration to decrease the NICARDIA-XL-30 exposure to the infant.
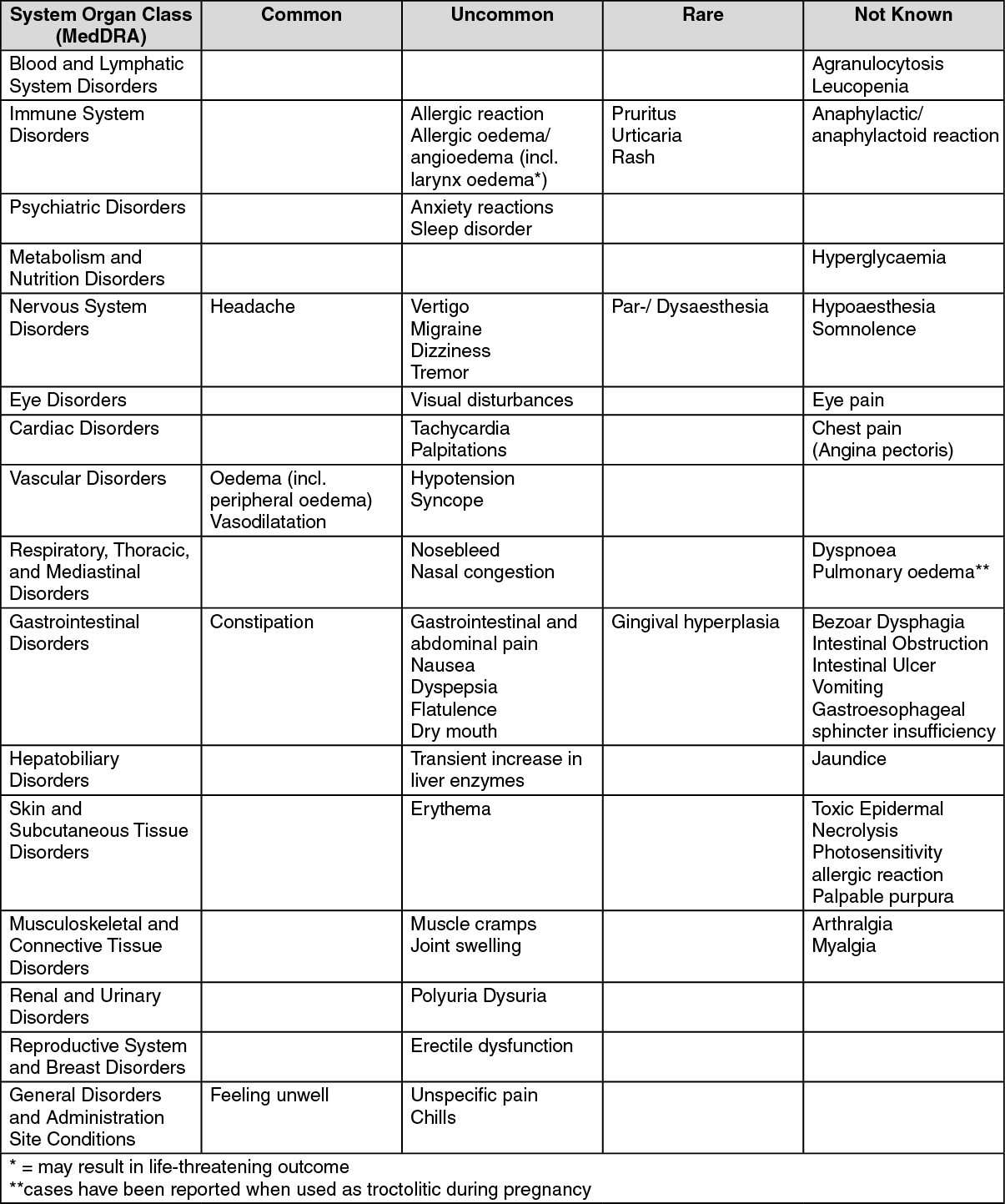
The most common side effects are headache, reddening of the face (flushing) and sensation of heat. Other common side effects reported include: See table.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
In dialysis patients with malignant hypertension and hypovolaemia a distinct fall in blood pressure can occur as a result of vasodilation.
Drugs that affect nifedipine: NICARDIA-XL-30 is metabolised via the cytochrome P450 3A4 system, located both in the intestinal mucosa and in the liver. Drugs that are known to either inhibit or to induce this enzyme system may therefore alter the first pass (after oral administration) or the clearance of NICARDIA-XL-30.
The extent as well as the duration of interactions should be taken into account when administering NICARDIA-XL-30 together with the following drugs: Rifampicin: Rifampicin strongly induces the cytochrome P450 3A4 system. Upon co- administration with rifampicin, the bioavailability of NICARDIA-XL-30 is distinctly reduced and thus its efficacy weakened. The use of NICARDIA-XL-30 in combination with rifampicin is therefore contraindicated.
Upon co-administration of known inhibitors of the cytochrome P450 3A4 system, the blood pressure should be monitored and, if necessary, a reduction in the NICARDIA-XL-30 dose considered. Drugs increasing NICARDIA-XL-30 exposure: Macrolide antibiotics (e.g., erythromycin); Anti-HIV protease inhibitors (e.g., ritonavir); Azole anti-mycotics (e.g., ketoconazole); Fluoxetine; nefazodone; quinupristin/dalfopristin; cisapride; valproic acid; Cimetidine; Diltiazem.
Upon co-administration of inducers of the cytochrome P450 3A4 system, the clinical response to NICARDIA-XL-30 should be monitored and, if necessary, an increase in the NICARDIA- XL-30 dose considered. If the dose of NICARDIA-XL-30 is increased during co-administration of both drugs, a reduction of the NICARDIA-XL-30 dose should be considered when the treatment is discontinued.
Drugs decreasing nifedipine exposure: rifampicin, phenytoin, carbamazepine, phenobarbital.
Effects of nifedipine on other drugs: NICARDIA-XL-30 may increase the blood pressure lowering effect of concomitant applied antihypertensives.
When NICARDIA-XL-30 is administered simultaneously with β-receptor blockers the patient should be carefully monitored, since deterioration of heart failure is also known to develop in isolated cases.
Digoxin: The simultaneous administration of NICARDIA-XL-30 and digoxin may lead to reduced digoxin clearance and, hence, an increase in the plasma digoxin level. The patient should therefore be subjected to precautionary checks for symptoms of digoxin overdosage and, if necessary, the glycoside dose should be reduced.
Quinidine: Co-administration of NICARDIA-XL-30 with quinidine may lower plasma quinidine levels, and after discontinuation of NCARDIA-XL-30, a distinct increase in plasma quinidine levels may be observed in individual cases. Consequently, when NICARDIA-XL-30 is either additionally administered or discontinued, monitoring of the quinidine plasma concentration, and if necessary, adjustment of the quinidine dose is recommended. Blood pressure should be carefully monitored and, if necessary, the dose of nifedipine should be decreased.
Tacrolimus: Tacrolimus is metabolised via the cytochrome P450 3A4 system. Published data indicate that the dose of tacrolimus administered simultaneously with NICARDIA-XL-30 may be reduced in individual cases. Upon co-administration of both drugs, the tacrolimus plasma concentrations should be monitored and, if necessary, a reduction in the tacrolimus dose considered.
Drug food interactions: Grapefruit juice inhibits the cytochrome P450 3A4 system. Administration of NICARDIA-XL- 30 together with grapefruit juice thus results in elevated plasma concentrations and prolonged action of nifedipine due to a decreased first pass metabolism or reduced clearance. As a consequence, the blood pressure lowering effect of NICARDIA-XL-30 may be increased. After regular intake of grapefruit juice, this effect may last for at least three days after the last ingestion of grapefruit juice. Ingestion of grapefruit/grapefruit juice is therefore to be avoided while taking NICARDIA-XL-30.
Other forms of interaction: Taking NICARDIA-XL-30 may increase the spectrophotometric values of urinary vanillylmandelic acid, falsely. However, HPLC measurements are unaffected.
Store below 30°C. Protect from light and moisture.
C08CA05 - nifedipine ; Belongs to the class of dihydropyridine derivative selective calcium-channel blockers with mainly vascular effects. Used in the treatment of cardiovascular diseases.
Nicardia-XL ER tab 30 mg
3 × 10's


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out
